


Abstract
Background Recent years have seen the introduction of online triage allowing patients to describe their problem via an online form. Subsequently, a GP telephones the patient, conducting a telephone consultation or arranging a face-to-face consultation.
Aim This study aimed to explore patterns-of-use and patients’ experiences of using an online triage system.
Design and setting This retrospective study analysed routinely collected data (from all practices using the ‘askmyGP’ platform for the duration of the study period, 19 May 2017 to 31 July 2017), using both quantitative and qualitative approaches. Data originated from an online triaging platform used by patients in nine general practices across the UK.
Method Data from 5447 patients were quantitatively analysed to describe characteristics of users, patterns-of-use, and reasons given by patients for using the platform. Free-text comments left by patients (n = 569) on their experience of use were qualitatively analysed.
Results Highest levels of use were observed in females (65.5%, n = 3570) and those aged 25–34 years. Patterns of use were high between 0800 and 0959, and on Mondays and Tuesdays. Use outside of GP practice opening hours was low. Common reasons for using the platform were for medication-related enquiries, for administrative requests, and to report a specific symptom. Comments left by patients suggested advantages to using the platform, for example, convenience and the written format, but these did not extend to all users.
Conclusion Patterns-of-use and patient types were in line with typical contacts to GP practices. Though the age of users was broad, highest levels of use were from younger patients. The perceived advantages to using online triage, such as convenience and ease of use, are often context dependent.
INTRODUCTION
The number of consultations in NHS general practice increased by 10% between 2007 and 2016, and the number of full-time equivalent GPs has decreased by 1% in the same period.1 This is contributing to increasing workload pressure,1 and affecting GP morale and job satisfaction.2 Alternatives to face-to-face consultation are increasingly encouraged by policymakers as a way to help manage demand and workload, and patients are now able to contact their GPs using a range of methods, including phone, email, and online triage systems.3 Such vision is driven by underlying assumptions that alternative routes are more convenient and accessible for patients, and an efficient use of practitioners’ time.4,5 However, there is limited evidence to support these assumptions and, apart from increased use of telephone consultations, most practices have been slow to adopt these approaches.1,6,7
A lack of supporting evidence is a particularly salient issue for more novel methods of contacting GPs, such as online triage platforms. Such platforms allow patients to use an online form to enter information about their query. The general practice will respond to the patient based on this information, normally conducting a telephone consultation or arranging a face-to-face consultation. NHS England has supported the roll-out of these online triage platforms, providing ‘£45 million for a national programme to stimulate uptake of online consultation systems for every practice’.8
Currently, there are various online triaging platforms available within the NHS general practices (askmyGP: http://askmygp.uk/, eConsult: https://econsult.net/, and egton Online Triage: https://www.egton.net/all-services/online-triage/).
Survey-based evidence indicates that patients find the timeliness, quality, and experience of care to be acceptable when using online triage platforms.9 However, studies to date have shown that anticipated reductions in workload associated with the use of online triage have not been realised.10 The limited evidence base available suggests that an online triage platform is most frequently used during the working week, with overall low levels of use.11
This study is the first to focus on a particular platform, ‘askmyGP’,12 with all UK studies to date focusing on a different platform, eConsult. Both platforms are incentivised in England for use by general practice.8 This study aimed to explore use of the ‘askmyGP’ online triage platform by describing the characteristics of, and patterns-of-use by, patients, and by obtaining insight into patients’ perspectives and experiences of the platform at the point of use.
METHOD
This was a retrospective analysis of routinely collected data from 5447 patients, taking both qualitative and quantitative approaches.
Online triage platform
Users access the ‘askmyGP Version 2’ (known hereafter as ‘askmyGP’) platform via their GP practice website and complete an online form detailing their background and query using a combination of tick-boxes and free-text boxes. Users have the option to identify themselves as a patient, parent, or carer. All users agree to the terms of use, which detail how the information they enter may be used and that the platform is not suitable for emergency complaints (see Appendix 1 for infographic of process). Users are informed that outside of practice opening hours their request will not be processed until the next working day. The practice receives the form and during opening hours a receptionist assesses the information and either completes an administrative request or passes a medical request to a GP, who then arranges either a face-to-face or phone consultation with the patient. If the request is received outside of practice opening hours, it is processed immediately at the beginning of the next working day (see Appendix 2 for infographic of process). All practices aim to respond within 1 hour of receiving the request. The ‘askmyGP’ platform has since introduced a two-way digital messaging facility with a GP, but this was not in place at the time of the present study and so was not examined.
How this fits in
Online triage platforms have been promoted by policymakers as they provide better access for patients and more efficient use of resources. However, such outcomes have not been demonstrated in research to date. This study examined patient users’ backgrounds and their patterns-of-use, and is the first study to examine feedback on using this specific platform. The findings both support and challenge some of the assumed benefits of using the platform.
Setting
The authors obtained data from all practices using the ‘askmyGP’ platform for the duration of the study period, 19 May 2017 to 31 July 2017. This excluded practices who started or ceased to use it during the study period, or ceased to use it before the study period. All practices were offering ‘askmyGP’ as an optional method of contacting the practice. The authors did not examine data before May 2017 as these data were not available in a consistent format.
Data collection
GP Access provided an anonymised dataset, comprising routine data collected by GP Access during the course of patient query submission to the ‘askmyGP’ platform. Names and contact details were removed from the original ‘askmyGP’ dataset before receipt by the research team. The names of general practices were replaced with codes to ensure anonymity.
The dataset for analysis included data that were automatically collected by the platform, such as time and date of encounter, and also included data provided directly by patients: age, sex, and reason for submitting a query, provided by the patient in a free-text box.
The dataset also included free-text comments on patient experience of leaving a query using the platform. Patients were invited to leave feedback after a query submission on a page loaded with the heading: ‘Please comment on your experience. (Do not enter personal details).’ Completion of this was not mandatory.
Analysis
Data analysis was conducted from August 2017 to October 2017. A small number of patients (n = 425) had used the platform more than once during the 3-month study period. Owing to the low numbers of patients to whom this applied, for the purposes of analysis, they were excluded and just the first encounter during the time period covered by the dataset was included. The authors could not confirm if the encounter in the dataset for each patient was the first encounter these patients had ever had with the platform, nor whether they had any other encounters with the general practice. The authors were not able to obtain information on how long each practice took to respond to the request or how it was resolved.
Quantitative analysis
The authors re-coded variables where necessary: patient age was re-coded into standard categories.13 Time of presentation was re-coded to create 2-hour slots starting from midnight (0000). Descriptive statistics were calculated for age, sex, time of use, and day of use. Data were analysed using SPPS (version 24).
Patients stated the reason for their query in a free-text box. There was an extensive number of different reasons for use given by patients, each written by patients in a different way. In order to present the reasons, the authors placed them into categories based on how the patients described their query and tabulated these for presentation. A practising senior clinician checked the content of each category against the data.
Qualitative analysis
The authors applied thematic analysis to all of the experience feedback comments from 569 patients, focusing on the barriers and facilitators of using the platform when raising a query. A coding framework was developed and adapted iteratively during the coding process using NVivo (version 10) software. Once organised, data were thematically analysed independently by two researchers. Conceptual maps were developed and compared, then key themes were identified. Contradictory data examples were sought and examined to further scrutinise identified themes. Interpretations of the data were discussed and explored between the two previous researchers and a third.
RESULTS
There was a total of 5447 unique entries. A total of 5140 patients (94.4%) left a free-text description of their reason for using the platform.
Quantitative analysis
Practice data
These came from nine general practices in the UK. They included practices from a range of rural, semi-rural, and urban areas, and with a range of deprivation scores, from 1–10 (most to least deprived) on the English indices of deprivation.14 One practice was using the platform as a trial during the study period. The number of patient users varied across the practices, with 59.4% of entries from users registered at practice 2 (Table 1).
Practice characteristics
Characteristics of users
Of those using the platform, 65.5% (3570/5447) were female. The mean age of users was 36 (range 0 to 95) years, with the highest number of users in the 25 to 34 years age group (22.7%, 1234/5447). Levels of use reduced as age increased, and fewer than 1% of users were aged ≥85 years. Age was not reported for 5.4% (292/5447) of the sample (Table 2).
Patient characteristics, N = 5447
Patterns of use
Levels of use varied according to the day of the week: total number of encounters was highest on a Monday (25.6%, 1392/5447) and Tuesday (19.2%, 1046/5447), with the lowest levels of use on a Saturday (2.2%, 118/5447) and Sunday (5.1%, 279/5447) (Table 3).
Number of patient encounters by day of the week, N = 5447
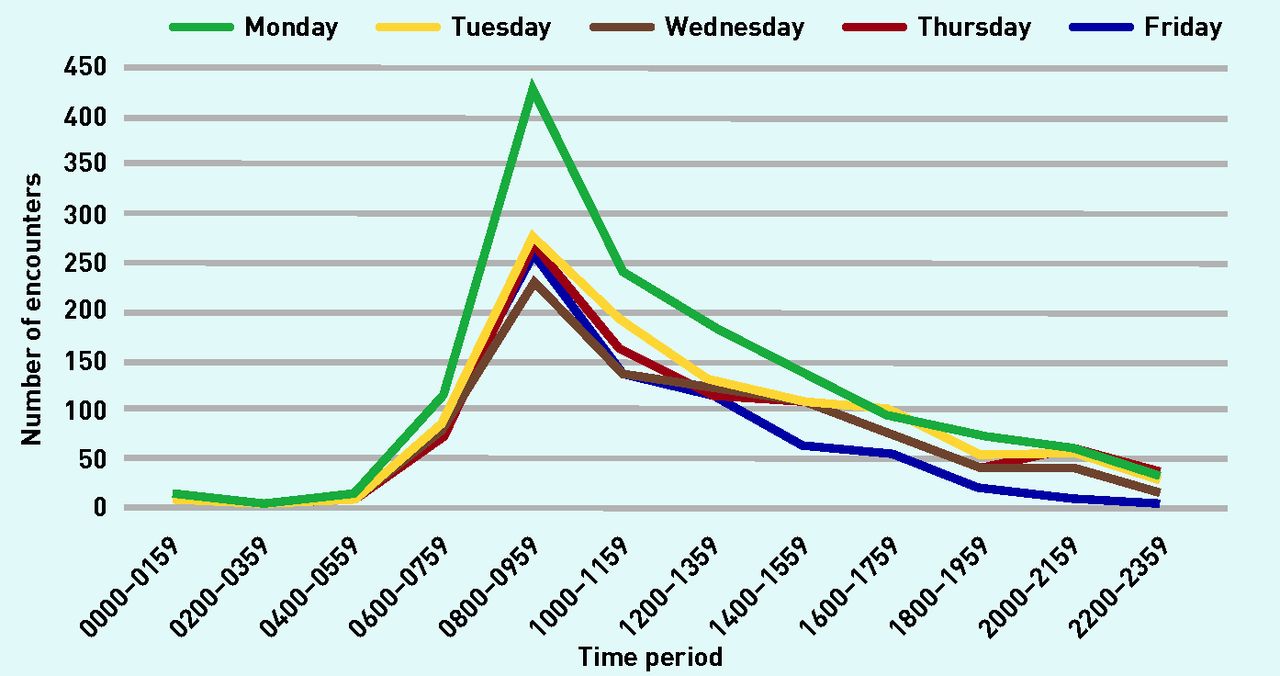
Across the week, highest usage levels occurred between 0800 and 0959 (27.4%, 1494/5447), and lowest levels of use were between 0200 and 0359 (0.2%, 13/5447) (Table 4).
Patient encounters by time of day, N = 5447
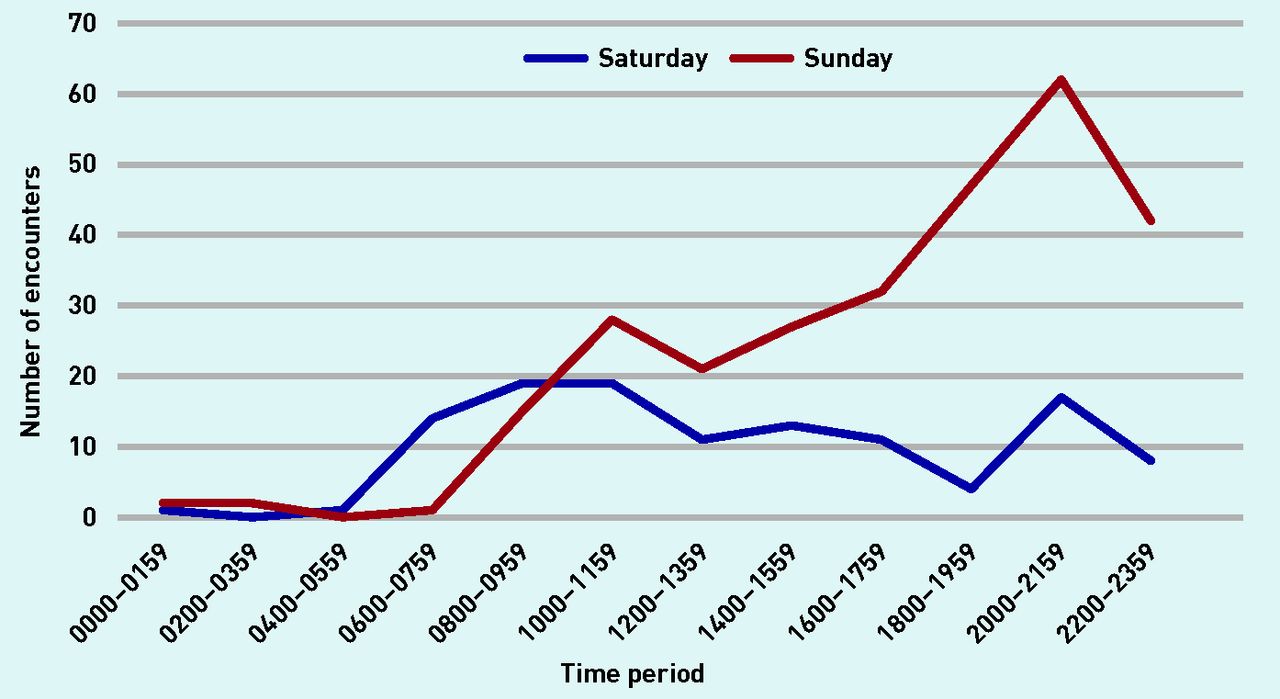
During Monday to Friday, usage was highest between 0800 and 0959 (28.9%, 1460/5050) (Figure 1). A different pattern was observed at the weekend with highest levels of use observed between 2000 and 2159 (19.8%, 79/397 [total weekend users]). Levels of weekend use were higher on a Sunday (70.3%, 279/397) than a Saturday (29.7%, 118/397) (Figure 2).

Time of use by patients during the week.

{kind=link}
{kind=link}
Time of use by patients at the weekend.
Reasons for query
The authors report 34 different categories of ‘reason for query’ given by patients. The most common was an enquiry about medication: 10.29% (529 out of 5140 reasons). Subsequent reasons were: to place an administrative request, 8.44% (434/5140); to report a specific symptom, 8.35% (429/5140); to report a skin condition, 7.98% (410/5140); to report an ear, nose, and throat-related query, 5.80% (298/5140); and for musculoskeletal issues, 5.76% (296/5140). The least common queries stated by patients were neurological, 0.06% (3/5140) and to request access to a specific service, 0.08% (4/5140).
Mental health-related queries accounted for 4.47% of queries (230/5140). Just 1.61% (83/5140) reported wanting to discuss multiple conditions. The full list of categories can be viewed in Table 5.
Reason given by patient for query, grouped into categories, N = 5140
Qualitative analysis
Of 5447 patients in the dataset, 569 (10.4%) left feedback about their experience of using the platform as a free-text comment.
Characteristics of users leaving comments
The 569 users who left a comment comprised more females (62%) than males (38%) and mean age was 44.2 (range 0 to 91) years (data not shown).
Findings
Key themes identified were: nature of a remote contact, quality of communication, perceived appropriateness, demand, and the role of online triage.
The authors observed both positive and negative perceptions of the same issues, suggesting that experiences of using the online platform were complex and relative to the patient and their characteristics, as well as the context in which the patient made the contact.
Nature of a remote contact
The nature of the alternative route for making contact with general practice was important in how patients perceived it. Some users found the type of access offered by the platform was positive, whereas others felt it to be negative. This was due in part to the mixed-mode approach: the initial patient contact is made online via the platform but the response from the practice is by telephone.
For some, the removal of the need for verbal interaction was viewed positively:
‘Love this. If you are feeling poorly the last thing you want to do first thing in the morning is make a phone call, so this online facility works perfectly.’
(Female [F], 35 years)
Conversely some patients felt that verbal interaction was important:
‘This a very frustrating way of dealing with patients. I want to explain to a person not a computer.’
(Parent/guardian of child [P/G], aged 3 years)
There were certain health conditions where a non-verbal form of communication was easier:
‘For a deaf person it is marvellous to be able to communicate without using a voice phone.’
(Male [M], 83 years)
Though this was not always the case and the online visual element could be a disadvantage, for example, in a patient with sight problems:
‘Having a sight problem, I need help to fill this in. It makes things less confidential for me.’
(F, 63 years)
Some patients expressed a dislike of the asynchronous interaction offered by the platform:
‘If you’re under stress because you’re poorly, I’d prefer to speak to a human!’
(F, 47 years)
‘Would rather see a doctor face to face not sure how you can tell someone is ill over the phone.’
(F, 51 years)
This linked into concerns about how patients could be adequately assessed remotely. How the problem would subsequently be dealt with on the telephone was a key element of the patient experience of the platform.
Despite the initial encounter being online, the logistical process of taking the telephone call response from the practice could be difficult. This was sometimes due to work responsibilities:
‘Difficult to wait by phone to take a call as driving instructor.’
(P/G, 15 years)
Some patients appeared to have encountered problems with the telephone call back. Some claimed they missed, or did not receive, the follow-up call from the GP surgery and subsequently were unsure how to proceed, or started the process again:
‘I have had to request a response multiple times this week for the same problem and have not had any contact from a doctor. This has meant I am now almost out of my medication and am worried about what might happen if I do not get a repeat.’
(F, 23 years)
‘Sometimes I have missed a call because I have been busy at work but the doctor does not retry at a later time, so I have to go through the whole process of raising a call again … ’
(F, 44 years)
Comments were indicative of teething problems associated with trying a new approach.
Quality of communication
Some noted how this method of contacting their GP may potentially influence the quality of communication. Some saw it as a potential improvement where they could take the time to write about what they wanted to discuss, whereas others highlighted concerns about the quality of the description they were able to leave in reference to their problem:
‘… would probably mention things you might forget when you are face to face.’
(P/G, 13 years)
‘I like this option because I can explain myself better.’
(P/G, <1 year)
Perceived appropriateness
Some users found the platform particularly appropriate for certain problems but less appropriate for others, especially where the patient was not sure what was wrong:
‘Difficult to know if symptoms are being overlooked by the patient.’
(F, 73 years)
For example, if a patient was sure they wanted to book a face-to-face appointment, using the platform was seen as a barrier to doing this:
‘ Very long-winded when in a rush and I just want to see a doctor.’
(F, 27 years)
However, users who were unsure whether their problem warranted an appointment considered the service as a useful way of checking:
‘Great service as don’t really want to waste an appointment if nothing can be done with problem but good to check.’
(F, 37 years)
The online element caused concern because of the need for patients to have computer skills. These comments tended to relate to hypothetical persons and not the person leaving the comment:
‘The system is good if you are computer savvy; however, for older patients they might find [the] system difficult to comprehend.’
(M, 64 years)
This was especially interesting because the patients were not directly invited to comment on suitability for others or indeed themselves, but did this regardless, deeming it to be an important factor.
Demand and the role of online triage
Patients referred to having to use the system out of necessity, because of prohibitively busy phone lines or because they had been signposted by reception staff to use the platform in lieu of booking an appointment. The comments referenced a general dissatisfaction with current routes for accessing GPs, including online triage:
‘Have used system because I was told on phone I would be unlikely to get a response via phone as practice too busy.’
(P/G, 9 years)
‘When a person is ill it would be helpful if they could speak to a person to book an appointment rather than giving personal details out across the internet. The hold time on your telephone is now at least 10 minutes.’
(F, 35 years)
Those who felt it was a useful intermediary step often showed concern about their personal use of resources, viewing the system as a potential way to save GPs’ time and prioritise appointments:
‘A really good idea for relieving GP surgeries of unnecessary appointments.’
(M, 31 years)
‘… saves ringing and making an appointment which another patient could have.’
(F, 64 years)
Some patients perceived it as working better than booking via the phone, whereas others commented on previous experiences of it working well for them:
‘Last time when I used it, I got a prompt and helpful response. No waiting on the lines and being stressed any more.’
(F, 36 years)
‘I have always got a great response.’
(F, 45 years)
There were clearly patients for whom online triage offered distinct advantages.
DISCUSSION
Summary
Overall, patients were using the platform in much the same way they used contact with a receptionist, with a wide range of users accessing the platform on a Monday morning, mirroring the busiest time for patients contacting their practice via telephone.15 The users of the platform were mostly female, and the majority of users were relatively young, aged 25 to 34 years.
In the sample of 5140 reasons given by a patient for a query, it was common for patients to leave a query about medication, a symptom, administrative query, an ear, nose, and throat-related concern, or musculoskeletal complaint.
The comments left by patients on experiences of using the platform suggested advantages, including convenient access, and the opportunity to write comprehensive descriptions of their problems. However, there were patients who found using the platform inconvenient and unsuitable. Experience of use is influenced by patients’ circumstances and perception of the ease of access currently available to them at their practice, and this has been described elsewhere.16
This study provides insights into the views of those using an online triage platform to contact their GPs. Patients seem to use it at similar times and for similar reasons as a traditional initial contact with a general practice. The suitability and convenience of online triage appears to be contingent on various factors such as the users’ background, preferences, their responsibilities, health status, and the issue they are consulting about.
Strengths and limitations
This was an independent evaluation of a dataset obtained from a commercial provider, allowing the authors to conduct the first exploration of the use of this platform; this was timely given online triage platforms are currently promoted by official bodies and policymakers in the UK.3,17 The present study made use of recent data on how patients are using the platform in real time and in a ‘real world’ way. A major limitation when analysing the routine datasets was that the authors were only able to analyse what was available and this could be extremely variable because the data were not collected by GP Access with the intention that it was to be used as a tool for research. Use of routine data has limitations in relation to completeness; the researchers were missing age data for some participants. The platform, ‘askmyGP’, is regularly revised to improve the service and changes are made to the forms that patients use. As a result, the authors were limited to a dataset comprising a 10-week period when the data were consistent and they had the personnel to conduct this study.
Use of real-world data means that one practice was particularly over-represented in the sample. However, this reflected the pattern of use of the platform at the time of the analysis in UK general practice, and, as might be expected, usage has grown to include more practices in the intervening period. The practice that accounted for the majority of the data was in an urban area with low levels of deprivation (as measured by the English Indices of Deprivation),14 and thus the applicability of the findings outside of this type of area may be reduced.
The authors observed disparity in levels of uptake of the platform by patients between practices and this is likely because of how individual practices are implementing the platform.16 Information on how individual practices promoted the platform to patients would have been useful while interpreting findings from this study, and future studies should ensure that this is explored.
The authors analysed the largest dataset to date on ‘reason for query’. This information was collected from patients using free text, thus any attempt to categorise these reasons as written by patients required a degree of interpretation. The ‘reasons for query’ did not fit into clinical categories in the way they would have if this information was taken from the patient record. It raises questions about the importance of this information to the receiving clinician.
Free-text comments provided a broad range of perspectives, allowing comprehensive analysis of patients’ views at the point of use, but was limited to data from those who chose to leave feedback comments. However, these people were well matched to the overall sample with regard to age and sex. The data collected on experience of using the platform were collected directly after the patient had registered their query, thus findings are based solely on their experiences of using the platform rather than the entire process (including subsequent consultations). This limits the generalisability of the findings.
Comparison with existing literature
The evidence base for use of online triage is in its infancy, with all published studies on online triage being published since 2017.9–11,18,19 The present study showed that the most frequent users of ‘askmyGP’ were female (65.5%) and aged 25 to 34 years. This corroborates evidence elsewhere finding similar proportions of online triage platform use in these groups.10,11 In line with findings from the present study, another study showed relatively low levels of use, with use occurring most frequently earlier in the week and during practice opening hours.11 They suggested this may be due to habit or low demand for out-of-hours contact, which has been evidenced elsewhere.20
A recently published study showed that the most common reasons for consulting face-to-face were musculoskeletal and administrative, for example, test results, medication-related issues, and skin symptoms,21 which closely matched the authors’ findings. A previous study that examined the reasons for query in 485 online triage consultations, as taken from the medical record, found the common reasons for use were for an administrative issue, for infection/immunological issues, and for musculoskeletal issues.11 These were also common reasons for online triage use in the present study.
The authors found that some patients liked writing a description of their problem and thought that this would improve the quality of their subsequent consultation. This finding is supported by an interview study with practice staff using an online triage platform, who felt the process allowed better preparation for, and quality of, subsequent consultations.10
Implications for research and practice
Practitioners should note that patients appear to be using the platform to obtain access in much the same way as they do via telephone, and for similar reasons. This information is useful in deciding what an online triage platform may bring to an individual practice and to patients, and practices should consider the intended purpose of introducing an online platform, and possible limitations when considering implementation. It has been argued that the development of such technologies within healthcare services is driven by aims to innovate, rather than a response to patients’ needs.19 It is important for practices to provide clear information about the process and how patients can best utilise it.
As official bodies and policymakers continue to promote use of digital services, additional research into patients’ demand for such services, and the barriers and enablers to using them, is necessary. Research into how such innovations are adopted and used will provide an understanding of unintended consequences and impact on access for some groups, for example, those who lack digital literacy. Further research should focus on the nature of the approach rather than the individual platform characteristics and should take a prospective approach, taking into account all the contacts a patient has with the practice and not just those with online platforms.
Acknowledgments
The authors wish to thank Harry Longman, creator of ‘askmyGP’, who provided data for independent analysis. They also thank Jeremy Dale for proofreading this article and Andrew Beggs for checking the categorisation of patient reasons for use.
Appendix 1.

How askmyGP works for the patient. ©GP Access Ltd.
Appendix 2.

How askmyGP works at the practice. ©GP Access Ltd.
Notes
Funding
Michael Hopper received a bursary from the University of Warwick’s ‘Undergraduate Research Support Scheme’. No additional funding was received.
Ethical approval
Ethical approval was obtained from the Biomedical and Scientific Research Ethics Sub-Committee of the University of Warwick (reference number: REGO-2017-2054). The data used in this study have been previously collected and are owned by a commercial company. The company are licensed to use data for any purposes in anonymised form. Each time a patient uses the platform they consent to an end user licence agreement. In doing so they agree to their anonymised data being shared with third parties and used for research purposes.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received October 26, 2018.
- Revision requested October 31, 2018.
- Accepted December 4, 2018.
- © British Journal of General Practice 2019
This article is Open Access: CC BY–NC 4.0 licence (http://creativecommons.org/licences/by-nc/4.0/).
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

