


Abstract
Background About 15.4 million people in the UK live with a long-term condition. Of the health and social care spend, 70% is invested in caring for this population. Evidence suggests that group-work interventions offer patient support, improved outcomes, and reduce the costs of care.
Aim To review the current evidence base examining the effectiveness of group work in long-term physical disease where such groups are facilitated by healthcare professionals.
Design and setting Systematic review and narrative synthesis of studies of group-work interventions led by health professionals for adults with specified long-term illnesses.
Method MEDLINE, EMBASE, PsycINFO, and Cochrane databases were systematically searched using terms relating to group work and long-term conditions. Studies were included if they were randomised controlled trials (RCTs) with a control group that did not include group work.
Results The 14 included studies demonstrated a high degree of heterogeneity in terms of participant characteristics, interventions, and outcome measures and were of varying quality. The studies demonstrated some statistically significant improvements in pain, psychological outcomes, self-efficacy, self-care, and quality of life resulting from intervention.
Conclusion This review demonstrates significant benefits resulting from group participation, in adults with long-term disease. Results were mixed and some benefits were short-lived. Nevertheless, these results suggest that group work should be more widely used in the management and support of adults with long-term illness. There is a need for larger and better-quality studies to explore this potentially important area further.
INTRODUCTION
Evidence increasingly demonstrates the value of group work to manage long-term conditions.1,2 Long-term conditions are placing a growing burden on individuals, their families, and healthcare systems. Around 15.4 million people in the UK are currently living with a long-term condition and care of this population accounts for 70% of the health and social care spend in England.3 Group-work interventions may be a way to offer effective support, improve outcomes for patients, and reduce costs to health and social care services.
In England the Expert Patient Programme (EPP) launched by the Department of Health in 2001 is an adapted version of the Chronic Disease Self-Management Programme (CDSMP), devised by Lorig and colleagues.4 It is based on Bandura’s self-efficacy theory5 and has been used and adapted widely as the basis for many lay-led and some professionally led group projects. Studies have shown that the CDSMP can lead to an increase in physical exercise, a decrease in health distress, and improvements in self-care and self-efficacy.6
Professionally led groups can be highly structured, and examples include the ‘group outpatient model’ used in the US; see, for example, the work by Sadur7 and the UK pulmonary rehabilitation programme.8 Other groups are based on the CDSMP and yet others adopt a much more psychological approach, for example, Herschbach.9
In this review the authors asked whether group work in long-term physical disease facilitated by healthcare professionals was effective.
METHOD
The search strategy was designed to identify all relevant literature relating to professional-led group-work interventions for long-term conditions. Inclusion criteria are illustrated in Box 1. Only randomised controlled trials (RCTs) and articles written in English were included. An initial scoping search was undertaken to identify search terms. Following this, MEDLINE, EMBASE, PsycINFO, and Cochrane databases were systematically searched on 29 October 2017. A combination of medical subject headings and keywords were used that focused around ‘group work’ and ‘chronic illness’ (synonymous with ‘long-term’ illness). These terms were combined using Boolean operators (a list of operators is available from the authors on request). Grey-literature searches were conducted using OpenGrey. Reference lists of all full-text articles were reviewed; no time restrictions were applied. One researcher undertook the search. Titles, abstracts and full-text articles (n = 91) were then reviewed by two researchers. Where there was disagreement regarding inclusion or exclusion of an article a third researcher was consulted.
| Category | Criteria |
|---|---|
| Participants | Aged ≥16 years with one or more of the following long-term conditions: heart disease; diabetes; stroke disease; lung disease; or arthritis. |
| Intervention | Health professional-led face-to-face group work, minimum six sessions. |
| Control group | Usual care or waiting list control. |
| Outcomes | Patient-reported outcome measures (including measures of symptoms: somatic and psychological; self-efficacy; self-care; quality of life; and health-related knowledge). The duration of these effects was also studied. |
Inclusion criteria
How this fits in
Evidence suggests that group-work interventions in long-term conditions offer patient support, improved outcomes, and reduced costs. This review supports the case that groups facilitated by healthcare professionals can be beneficial in improving pain, psychological symptoms, self-efficacy, self-care, and quality of life. Such group work should be more widely used in the management of adults with long-term illness. More and higher-quality research is needed to evaluate and identify specific elements of the intervention, and to identify an effective duration of the intervention.
Data extraction
Data extraction involved using a bespoke form based on that used by Cochrane. Data extraction included the age, sex, and ethnicity of participants; location, group-work setting, theoretical basis, type of professional leader; and number and length of sessions. All primary and secondary outcomes relating to health and wellbeing were extracted.
Analysis
A narrative approach was taken to synthesis, as recommended in circumstances of heterogeneity of the methods, interventions, and outcome measures of the included articles.10 This process comprises five stages: problem identification, literature search, data evaluation, data analysis, and presentation.11
RESULTS
A total of 14 studies from six countries including 2578 participants were included (Figure 1).12

PRISMA diagram.12 N/A = not applicable. RCT = randomised controlled trial.
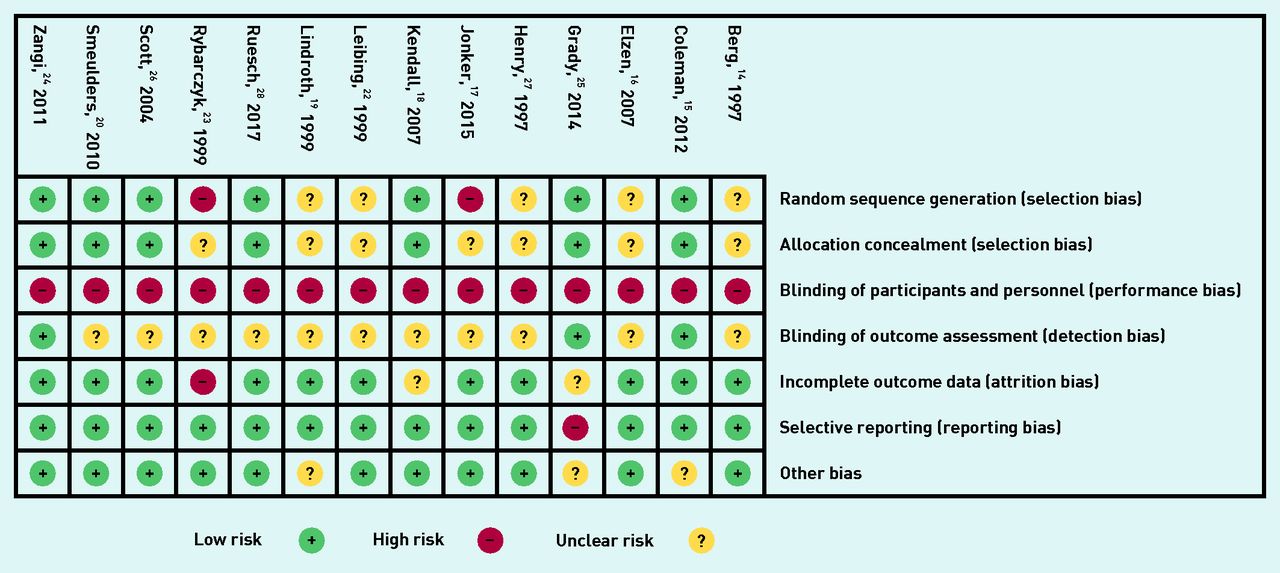
Risk of bias assessment was conducted for all included articles.13 Studies were judged low, unclear, or high risk based on seven methodological quality domains (Figure 2). Overall, though the methodological quality of the studies was mixed and there was some absence of reporting, they appeared to be reasonably robust in terms of risk of bias. For example, most of the areas of high risk were for blinding. Given the nature of the intervention (a healthcare practitioner-delivered group) and the control (waiting list) it would not have been possible to blind either participants or personnel.

{kind=link}
{kind=link}
Methodological quality of included articles.
An overview of the included studies is available from the authors on request. There was an extensive range of outcome assessment tools used (a table of outcome assessment tools used by studies and a description of the tools is also available from the authors on request). The studies covered a wide range of patient characteristics and of interventions. Many of the interventions were either loosely or more rigorously based on the CDSMP.14–20 Others offered a range of other psychological interventions. The interventions are presented in accordance with the TIDieR Consort criteria.21 Box 2 groups the studies by intervention used.
| Intervention used | Description of intervention | Applicable articles |
|---|---|---|
| CDSMP | Developed by Lorig and colleagues at Stanford University, the CDSMP29 is based on Bandura’s self-efficacy theory.5 It is a manual-driven programme30 and incorporates strategies to enhance self-efficacy. It is designed to be delivered by lay leaders, but many programmes are delivered by healthcare professionals. | Elzen,16 Jonker,17 Kendall,18 Lindroth,19 Smeulders20 |
| OAK | This is a disease-specific self-management programme based on social cognitive theory.31 It is designed to be delivered by healthcare practitioners with a specified minimum level of musculoskeletal education. | Coleman15 |
| Asthma Self-Management Programme | Based on behavioural and social learning theory32 and the programme is designed by Creer, Reynolds, and Kotses.14 | Berg14 |
| Group CBT | A structured psychotherapy that involves dealing with a participant’s beliefs in order to change the way they think and react to the things happening around them, used in a group setting. | Henry,27 Leibing,22 Ruesch28 |
| Mind–body wellness intervention | A multicomponent intervention. These can include instruction on the mind–body connection; relaxation training; CBT; problem solving; communication; and information on nutrition and exercise. | Rybarczyk23 |
| Vitality Training Programme | A mindfulness-based programme. It includes guided imagery, relaxation, use of music and art, and group discussion. | Zangi24 |
| Group care model | Not based on a particular theory or approach, this includes education, group discussion, and the opportunity for one-to-one meetings with the physician. | Scott26 |
| Group counselling | Not based on a particular theory or approach, a disease-specific self-management intervention that utilises coaching in self-management skills and problem solving, underpinned by behaviour change techniques such as self-monitoring and cognitive restructuring. | Grady25 |
CBT = cognitive behavioural therapy. CDSMP = Chronic Disease Self-Management Programme. OAK = Osteoarthritis of the Knee Self-Management Programme.
Interventions used in the studies
After analysis, seven themes emerged from the data. The first six are included in Box 3.
| Study | Somatic symptoms and physical functioning | Psychological symptoms | Self-efficacy | Self-care | Quality of life | Knowledge of illness or health |
|---|---|---|---|---|---|---|
| Berg,14 1997 | – Journal of daily asthma concerns including wheeze, cough, shortness of breath, and chest tightness | – | – (SEAMS)a | + Post-treatment inhaler use (observed) – (ASMAT) Ability to make good decisions in a variety of clinical scenarios, for example, severe asthma attack | – | – |
| Coleman,15 2012 | + Pain: WOMAC at 8 weeks, not maintained at 6 months + SF-36 body pain maintained at 6 months + (TUG) Hamstring strength and range of motion test (small improvements) maintained at 6 months | – | – | – | + (WOMAC — physical functioning and total scores: SF-36 physical function, physical role, vitality, and social function) At 8 weeks, maintained at 6 months | – |
| Elzen,16 2007 | – (RAND-36, physical component summary scale of the Dutch version) | – (RAND-36, mental component summary scale of the Dutch version) | – (GSES — Dutch version) | – Self-management behaviour using scales developed by Lorig for the CDSMP,29 frequency of exercise, cognitive symptom-management (coping with symptoms scale), and (quality of) communication with a physician (self-reported scale) | – | – |
| Grady,25 2014 | – (SF-36 — physical functioning scores) | – | – | – | – (QLI) | – |
| Henry,27 1997 | – | + (STAI) Anxiety and perceived stress (Hassles scale) – (BDI) Depression – Coping ability, frequency of hassles, and perceived coping ability (Hassles scale) | – | – | – | – |
| Jonker,17 2015 | – | + (CES-D) Depression scores at 6 months – Positive affect (CES-D assessed separately using a specific subscale of the CES-D) | + (12-item version of the perceived self-efficacy scale) + (Abbreviated version of the Pearlin Mastery scale). People with less education (≤9 years) benefited more. Those with >9 years of education showed no significant effect | – | + (Dutch version of VOL-scale) At 6 weeks and 6 months | – |
| Kendall,18 2007 | – | – | – (Lorig SES) | – | + (SSQoL – which includes domains measuring physical, psychological, and social wellbeing). At 9 months for family roles and fine motor tasks + A trend towards significance (P = 0.05) in relation to work productivity and self-care – Physical, psychological, and social domains of the SSQoL | – |
| Leibing,22 1999 | – Disease activity + (VAS) Pain at 9 months’ follow-up + Affective pain score | + (STAI, DS, AHI) + Anxiety, depression, and helplessness + Coping (adapted BeCoMo), positive acceptance, and resignation | – | – | – | – |
| Lindroth,19 1997 | + (VAS) Pain at 3 months, not maintained at 12 months | – (Single question) | – (Swedish version of the AHI) Perceived helplessness did not change + (Single question) Self-confidence at 3 and 12 months | + (Interview) Joint protection behaviours at 3 and 12 months and more home exercises at 3 months + (Single question) Capacity to ease pain at 3 and 12 months | + (Swedish version of the Stanford HAQ). Perceived disability at 3 months, not maintained at 12 months | + (Assessed on five key questions with yes or no answer options). At 3 and 12 months + Change in knowledge about inflammation and different arthritis treatments correlated positively with a reduction in helplessness. The intervention group reported fewer problems due to lack of knowledge about disease, diet, and physical therapy at 3 and 12 months |
| Ruesch,28 2017 | – | + (Depression subscale of the German version of HADS) immediately post-intervention but not maintained – Global psychological distress (German version of the BSI — Global Severity Index calculated the means of all items) | – | – | + Health-related quality of life (German version of SF-12): on mental composite scores immediately post-intervention but not maintained at 2 months + On physical composite scores treatment group significantly improved post-treatment and at 2 month’s follow-up | – |
| Rybarczyk,23 1999 | – (MSCL) In frequency of medical symptoms + (SF-MPQ and MSCL sleep, pain) | + (BAI, CES-D) Significant decrease in anxiety and depression symptoms + Those defined as having clinical levels of anxiety – Those defined as having clinical depression | + (MHLC) Belief that chance factors influence health – Internality, powerful others | – Health behaviours | – | – |
| Scott,26 2004 | – (Advanced, household, and basic ADLs Functional outcomes: a composite measure derived from two established tools) | – | + (Scales drawn from Lorig29) Communicating with physicians – Managing their disease, doing chores, participating in social/recreational activities, and controlling/managing depression (scales drawn from Lorig29) | – | + (QOL score) 10-point self-reported quality-of-life scale at 24 months | – |
| Smeulders,20 2010 | – | – (HADS) | + Psychosocial attributes (GSES — Dutch version: Cardiac Self-Efficacy Questionnaire). (Pearlin Mastery scale) Perceived control + (Coping With Symptoms Scale — Lorig) Cognitive symptom management not maintained at 6 and 12 months’ follow-up | + (EHFScBS) Self-care, short-term effect not maintained at 6 and 12 months | + (RAND-36, KCCQ, Perceived autonomy VAS and HADS) short-term effect not maintained at 6 months | – |
| Zangi,24 2012 | + (Numerical Rating Scales) Fatigue post-treatment that improved at 12 months – Effects in pain and the patient global assessment of disease activity | + (GHQ-20, EAC) Psychological distress at 12 months in the intervention groupb + Emotional processing – Emotional expression | + (Pain and symptoms subscales from the Arthritis SES) Self-efficacy pain indicating better ability to manage pain despite the lack of significant improvement in symptoms – Self-efficacy – general, cardiac, symptom management | + (10-point NRS) Self-care ability and overall wellbeing maintained at 12 months | – | – |
↵a Assessment tool used by study is shown in brackets.
↵b Number of participants exceeding the GHQ-20 threshold of 23 (indicating significant psychological distress) was reduced from 13 (36%) at baseline to 2 (6%) at 12 months compared with 10 (29%) at baseline to 8 (24%) at 12 months in the control group. + = statistically significant outcome – = no statistically significant outcome. ADL = Activities of Daily Living. AHI = Arthritis Helplessness Index. Arthritis SES = Arthritis Self-Efficacy Scale. ASMAT = Asthma Self-Management Assessment Tool. BAI = Beck Anxiety Inventory. BDI = Beck Depression Inventory. BeCoMo = Bernese Coping Modes Tool. BSI = Brief Symptom Inventory (German version). CDSMP = Chronic Disease Self-management Programme. CES-D = Centre for Epidemiologic Studies Depression Scale. DS = Depression Scale. EAC = Emotional Approach to Coping Scale. EHFScBS = European Heart Failure Self-Care Behaviour Scale. GHQ-20 = General Health Questionnaire. GSES = General Self-Efficacy Scale. HADS = Hospital Anxiety and Depression Scale. HAQ = Stanford Health Assessment Questionnaire (Swedish version). KCCQ = Kansas City Cardiomyopathy Questionnaire. MHLC = Multidimensional Heath Locus of Control Scale. MSCL = Medical Symptoms Checklist. NRS = numerical rating scale. QLI = Quality of Life Index (cardiac version). QOL = quality of life. RAND-36 = RAND. SEAMS = Self-Efficacy for Asthma Management Scale. SES = self-efficacy scale. SF-12 = Short Form (12 item) Health Survey (German version). SF-36 = Short Form (36 item) Health Survey. SF-MPQ = Short-form McGill Pain Questionnaire. SSQoL = Stroke Specific Quality of Life Scale. STAI = Spielberger State-Trait anxiety scale. TUG = Timed ‘Up and Go’ test. VAS = Visual Analogue Scale. VOL-scale = Value of Life scale. WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index.
Themesa
Somatic symptoms
In studies that measured pain as an outcome,15,19,22,23 all except Zangi24 demonstrated statistical improvement in the intervention group compared with control. In some studies this effect is short-lived (8 weeks,15 3 months19), whereas in others it persisted for 9 months.22 In people with osteoarthritis of the knee, functional parameters improved and were maintained at 6 months.15 A reduction in fatigue that further improved by 12 months following group participation was observed in people with inflammatory joint disease.24 There were no changes in asthma symptoms,14 physical components of the RAND-36 and SF-36 measure,16,25 ‘disease activity’,22,24 and activities of daily living (Box 3).26
Psychological symptoms
Most studies that evaluated this found statistically significant improvements in some psychological outcomes following group participation.17,22–24,27,28 Henry27 found improvement in anxiety and perceived stress, but not depression and coping ability. Jonker17 reported improvement in depression but not in ‘positive affect’. Ruesch28 found improvements in depression scores immediately post-intervention, not maintained at 2 months and no effect on ‘global psychological distress’. Zangi24 found improvement in psychological distress and ‘emotional processing’ maintained at 12 months, but not in ‘emotional expression’. Leibing22 found positive effects in anxiety, depression, feelings of helplessness, and some aspects of coping. Rybarczyk23 demonstrated improvement in anxiety and depression scores. Three studies found no positive psychological effect (Box 3).16,19,20
Self-efficacy
Self-efficacy theory is a key foundation of the CDSMP.5 Therefore, it is not surprising that several studies have looked at the effect of their intervention on self-efficacy. Six studies found some statistically significant positive effect on self-efficacy following group intervention.17,19,20,23,24,26 Jonker17 found improvements in self-efficacy and mastery maintained at 6 months. This effect was seen in those with less high school education, but not in those with more education. Zangi24 found benefits that improved between immediate post-treatment analysis and 12 months. Other studies19,20,23,26 reached mixed conclusions on self-efficacy parameters. Three 14,16,18 found no significant changes in self-efficacy measures (Box 3).
Self-care
Six studies reported the effect of group work on patient self-care.14,16,19,20,23,24 Statistically significant improvements were seen in inhaler use,14 joint protection and exercise,19 capacity to ease pain,19 self-care in heart failure,20 and overall self-care and wellbeing (maintained at 12 months).24 Three studies, however, found no significant effect on self-care in some or all of the parameters measured (Box 3).14,16,23
Quality of life
Seven studies demonstrated statistically significant improvements in quality of life (QOL) measures.15,17–20,26,28 In some of these studies improvements were maintained at 6 months15,17 and 24 months.26 One article did not find statistically significant QOL effects,25 but the control group had information and some telephone contacts with health professionals and improvement was seen in both treatment and control groups (Box 3).
Knowledge
Only one article specifically measured changes in participants’ knowledge (about rheumatoid arthritis).19 There was significant improvement at 3 and 12 months and a correlation was seen between knowledge increase and reduction in helplessness (Box 3).
Duration of effects
Six studies demonstrated most, or all, of their statistically significant effects at or beyond 6 months post-intervention.15,17,22,24,26,28 There were both short-term (<6 months) and longer-term effects seen in Lindroth’s study19 whereas Smeulders’ study20 demonstrated predominantly short-term effects only. The remaining studies either did not demonstrate any significant effects14,16,25 or did not clearly specify time points of data collection.23,27 Zangi’s24 study demonstrated further improvement at 12 months (compared with immediately post-intervention) on several parameters. There were no adverse events reported.
DISCUSSION
Summary
The authors set out to address the hypothesis that, by enhancing an individual’s self-care skills within the context of a group facilitated by health professionals, their capacity to cope with and manage their health issues is enhanced. This review supports the case that such groups are beneficial for individuals with the long-term conditions studied in improving pain, psychological symptoms, self-care, self-efficacy, and quality of life. These results are potentially of interest to policymakers and providers. More work is needed in order to determine what specific elements are effective and at what ‘dose’, but this review supports the case for more widespread use of group work in long-term conditions.
Strengths and limitations
The review presented here included 14 articles that considered the effectiveness of group work facilitated by healthcare professionals for patients with long-term conditions. The included studies covered a range of interventions and outcome measures. Even when a specific outcome was measured, for example, self-efficacy, a range of tools was used. It is difficult to draw any conclusions about what specific intervention(s) may be effective. The four studies that demonstrated most improvements are those by Coleman,15 Leibing,22 Scott,26 and Zangi.24 These interventions were each very different: CDSMP, mindfulness, cognitive behavioural therapy (CBT), and the US group outpatient model.
The present review was comprehensive as no date limit was set on included articles, but keywords may not have been fail-safe in procuring all relevant articles. However, the authors’ citation searching was thorough and a significant number of the final articles were found this way. The studies in this review were varied in terms of participant characteristics and intervention delivered making meta-analysis not feasible. The results of some included studies14,23,27 should be considered with caution due to the small number of participants, short length of follow-up (7 weeks in one case),27 and number of group-hours offered (as few as 9 hours).27 In some cases the instruments used lacked validity.14 Some studies had areas of uncertainty, and some high risk of bias.17,23,25 The Cochrane review of lay-led group work1 experienced many of the above limitations and in particular noted short-term assessment of outcomes, mostly only up to 6 months.
In terms of non-CDSMP interventions one of the most effective interventions appeared to have been Zangi,24 which was a study based on mindfulness. The improvements were sustained and improved at 12 months post-intervention. In this study, perhaps significantly, there were many more hours of group time (45 hours) than the other studies (most were <20 hours) suggesting a potential ‘dose–response’ effect.
Comparison with existing literature
Some interventions were theoretically underpinned and included theories such as self-efficacy or social cognitive theory5 and CBT.33 Both these approaches include constructs such as cognition, emotion, self-beliefs, and mastery, and personal and environmental factors. Social cognitive theory incorporates the concept of self-efficacy as a key component. Self-efficacy is ‘the belief in one’s capabilities to organize and execute the courses of action required to manage prospective situations’.34 A systematic review demonstrated that the CDSMP (underpinned by self-efficacy theory) led to increased physical exercise, less health distress, improved self-care, and self-efficacy.35 There is some systematic-review evidence of efficacy of CBT in long-term physical illness.36 The study presented here included studies that demonstrated CBT to impact pain and psychological, but not functional, outcomes.22,28 It is feasible that, although self-efficacy and cognitive constructs are useful, there may be additional determinants at play, such as attitudes, social influences, and motivation.37 This possibility is supported by Elzen’s study16 where, despite there being no statistically significant findings, the intervention was very popular among participants with very high attendance rates, suggesting that the patient gains may not have been identified by the outcome measures used. There is also evidence that interventions that are tailored according to assessed determinants are more effective than those that are not.38
As the CDSMP is such a widespread intervention it is worth considering the results of the six CDSMP studies.14–16,18–20 Improvements were found in treatment concordance,14 quality of life,15,18,20 and other outcomes such as somatic symptoms,15 self-care, and self-efficacy.20 This is consistent with findings from an RCT of a lay-led CDSMP intervention,29 which showed improvements at 6 months in health behaviours, for example, exercise, self-reported health, social or role activities, and fewer hospitalisations and days in hospital. The Cochrane review of lay-led group work1 demonstrated improvements in self-efficacy, self-rated health, cognitive symptom management, and frequency of aerobic exercise.
Implications for research and practice
The present study adds to the evidence that supports the more widespread use of group work in adults with long-term illness.
Not all included articles underpinned their interventions with theory. In the future the authors recommend that interventions should be underpinned with theory in accordance with the National Institute of Health and Care Excellence guidelines39 and the guidelines for complex interventions development.40
Future research could usefully examine which specific elements of group interventions are useful, perhaps by comparing different group approaches in a similar population, and more rigorous analysis of long-term outcomes. Other questions to address are: what qualities in facilitators produce greater impact on outcomes?
To be able to evaluate group work with greater clarity (including meta-analysis) consistency in the use of outcome tools is essential. There should be some evaluation of the relative merits of professional versus lay-led group work to include economic evaluation. The authors found only two studies that made comparisons between these.41,42 They both studied the same intervention (the CDSMP) in individuals with arthritis and therefore cannot be generalised. Further consideration, including the economic impacts of a possible ‘dose–response’ effect, would also be relevant.
Overall the authors recommend professionally led group-based interventions to support people with long-term conditions. There are many positive outcomes reported. Further research in this area is needed.
Acknowledgments
The authors acknowledge the support of Dr Dean McMillan, clinical psychologist and researcher, Hull York Medical School and the Department of Health Sciences, University of York, in the design of this systematic review.
Notes
Funding
This study was funded by the Scientific Foundation Board of the Royal College of General Practitioners (grant number: SFB 2013-08) and is registered with Prospero (registration number CRD42017079708).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received September 17, 2018.
- Revision requested October 9, 2018.
- Accepted November 6, 2018.
- © British Journal of General Practice 2019
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

