


Article Figures & Data
Figures
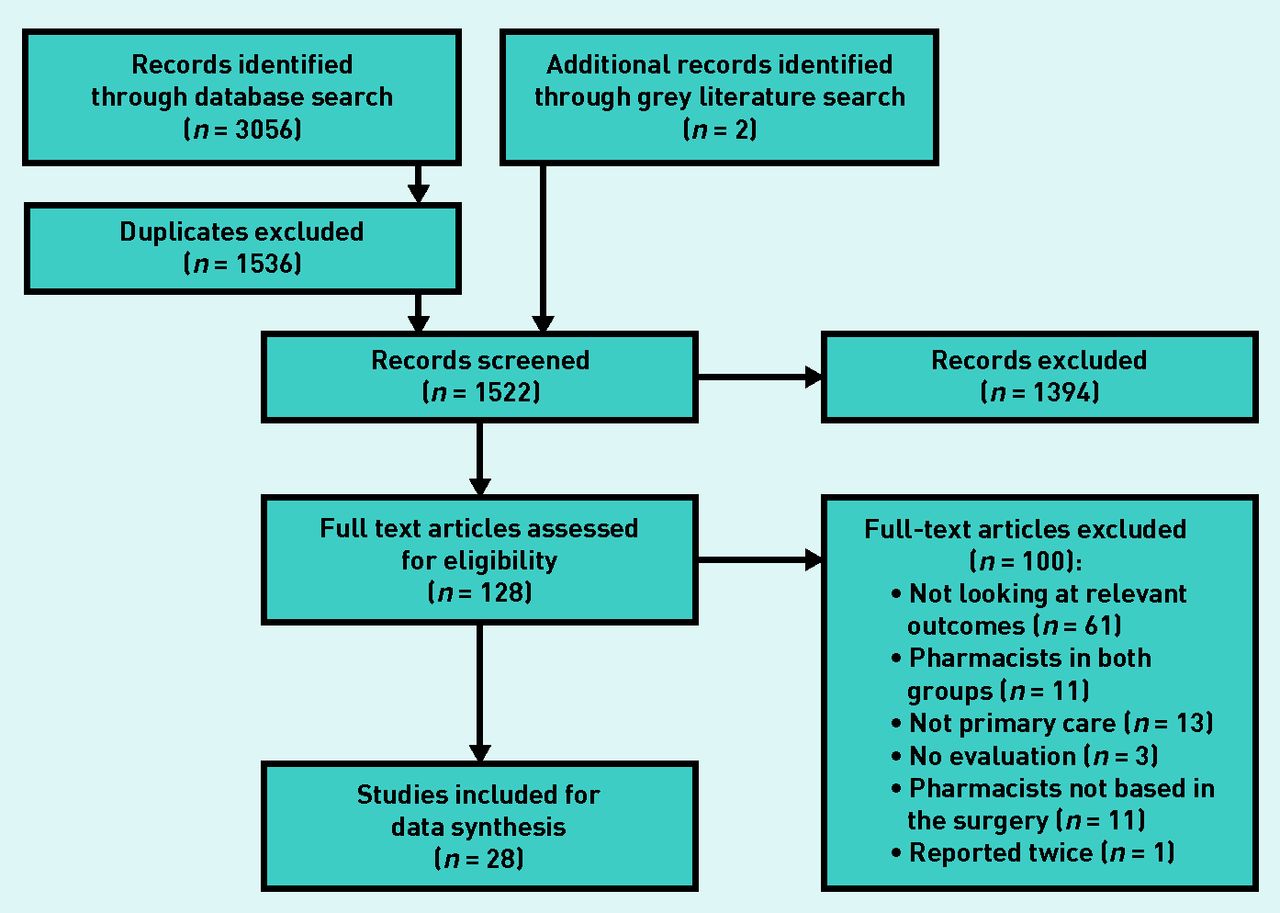
- Figure 1.
PRISMA flowchart: study inclusion.

{kind=link}
Tables
How this fits in
Evidence shows that pharmacists working in primary care teams can improve clinical outcomes and increase patients’ level of satisfaction with their care. However, pharmacists’ impact on healthcare system-related outcomes is unclear. This review indicates that pharmacists integrated into primary care may reduce the number of GP appointments needed, as well as emergency department attendance; however, they appear to increase primary care use overall. Further research is needed to establish the long-term impact of the integration of pharmacists at scale. Author(s) Year Country Study design Sample size Population/sample demographic Health system outcome(s) Key findings/conclusions Borenstein et al 32 2003 US Randomised comparative trial 197 Patients aged >18 years with uncontrolled hypertension with capitated health insurance recruited from two primary care offices Primary care visits, primary care costs, medication costs Physician–pharmacist comanagement for patients with uncontrolled hypertension resulted in improved BP control and reduced primary care physician visit rates, and reduced average visit costs per patient. Britton and Lurvey28 1991 US RCT 572 Patients registered at a primary care medical centre who were receiving ≥5 prescription or non-prescription medications Number of medications, medication costs, medical supplies Medication profile review by a clinical pharmacist statistically significantly reduced both the number and the cost of drugs for patients receiving ≥5 medications Brunisholz et al 33 2018 US Retrospective observational study 1358 Patients with high BP and/or diabetes mellitus within a primary healthcare network Hospitalisations, ED visits. primary care visits, specialty visits Pharmacist intervention was associated with improved disease management, but statistically significantly increased visits to primary care, specialty care, care managers (registered nurse), and the ED Bush et al 43 2018 UK Retrospective observational study 5.4 WTE pharmacists Clinical pharmacists within 49 GP practices in Dudley CCG Primary care visits, healthcare costs In a 4-month period, pharmacists saved 628 GP appointments, 647 GP hours in medication review/repeat prescribing and led to a total savings of approximately £1.5 million Campins et al 45 2017 Spain RCT 503 Community-dwelling polymedicated (>8 drugs) older people (aged >70 years) Number of medications, primary care visits, ED visits, hospitalisations, medication costs, healthcare costs Intervention reduced medication use by 5% with no observed health risks. There were more primary care visits with the intervention (difference became non-significant at 12 months), but no differences in ED visits or hospitalisations. The intervention led to a 7% reduction in medication costs Finley et al 27 2003 US RCT 125 Patients registered at a primary care medical centre, recently started on antidepressants for depressive symptoms Primary care visits, ED visits, healthcare use, medication costs Clinical pharmacists had a favourable effect on multiple aspects of patient care, but did not show a statistically significant difference in resource use Harris et al 30 2009 US Prospective observational cohort study 92 Patients registered at a university based family medicine clinic, had ≥5 medications, multiple medical conditions, and/or medical conditions that resulted in high use of health care Number of medications Medication therapy review and intervention by pharmacist resulted in a small reduction in average number of medications per patient Hirsch et al 21 2014 US Randomised pragmatic trial 166 Patients with uncontrolled hypertension registered at a university-based general medicine clinic Primary care visits Pharmacist intervention was more effective at lowering BP than usual care, and associated with fewer primary care physician visits Hunt et al 22 2008 US RCT 463 Patients with uncontrolled hypertension registered at one of nine primary care clinics within a primary care research network Primary care visits, number of medications, use of generic medications Patients with pharmacist hypertension management had more total primary care visits, but fewer primary care physician visits. Intervention patients were statistically significantly more likely to be prescribed generic antihypertensive medications but there was no statistically significant effect on overall pill burden Lenander et al 44 2014 Sweden RCT 209 Patients registered at a large primary care centre, aged ≥65 years with ≥5 different medications Hospitalisations, primary care visits, number of medications Pharmacist intervention resulted in reduction in the number of drugs per patient Lowrie et al 39 2012 UK Cluster-randomised controlled, event driven, trial 2164 Patients registered at 174 NHS general practices. Eligible patients were aged ≥18 years and had left ventricular systolic dysfunction confirmed by cardiac imaging Hospitalisations A pharmacist intervention resulted in modest improvements in the prescribing of disease-modifying medications. There was no difference in hospitalisation between groups Mourão et al 47 2013 Brazil RCT 100 Patients registered at six public health system primary care centres, aged ≥18 years, using oral antidiabetic medications, and had presenting HbA1c levels of ≥7% Number of medications The number of drugs taken by the control group remained the same, while the intervention group showed a statistically significant increase Neilson et al 40 2015 UK Pilot RCT 125 Patients registered at six general practices, aged ≥18 years, and receiving regular prescribed medication for pain Primary care visits, specialist visits, hospitalisations, medication costs, specialist visit costs, hospitalisation costs, primary care costs Pharmacist-led intervention for chronic pain was more costly and provided similar QALYs to treatment as usual Obreli-Neto et al 46 2015 Brazil RCT 200 Patients registered at a primary healthcare unit, aged ≥60 years, diagnosed with diabetes or hypertension, and receiving drug treatment for diabetes or hypertension Primary care visits, specialist visits, ED visits, number of medications, healthcare cost Pharmacist intervention was associated with statistically significantly higher GP and specialist visit rates, but statistically significantly lower ED visit rates. There was no difference in overall healthcare costs for intervention and control groups. Okamoto and Nakahiro31 2001 US Prospective, randomised, comparative study 330 Patients in hypertension and general medicine clinics within a managed care organisation, who were ≥18 years old and diagnosed with hypertension, and taking specified antihypertensive drugs Number of medications, primary care visits, ED visits, hospitalisations, medication costs, specialist visit costs, ED costs, hospitalisation costs There were more primary care visits in the pharmacist managed group, with associated higher visit costs. There were four ED visits in the control group, and none in the pharmacist group. BP measurements were statistically significantly lower in the pharmacist-managed group with cost-effectiveness ratios for BP mangement lower in the pharmacist intervention group. Phelan et al 41 2008 UK RCT 106 Patients aged ≥55 years registered with one of 15 participating general practices, who consulted their GP with pain, stiffness, or both in one or both knees Medication costs Pharmacists can make a positive contribution to the management of patients with knee pain in primary care; pharmacist intervention may reduce medication-related costs Price-Haywood et al 34 2017 US Retrospective observational study 5044 Adult patients (>18 years) with diabetes and/or hypertension who attended a community health centre Primary care visits Patients who saw a pharmacist within the collaborative care model saw their primary care provider more often. The intervention did not lead to any differences in BP or glucose control Ragucci et al 26 2005 US 1-year observational study 191 Patients with diabetes at three university-based primary care clinics Healthcare costs Pharmacists achieved significant improvements in HbA1c values, BP, and aspirin use. Statistically significant cost avoidance was calculated based on HbA1c reductions Roth et al 29 2013 US Prospective, observational pilot study 64 Patients registered at a community-based primary care medical practice, aged ≥65 years, who were taking at ≥5 medications Hospitalisations, ED visits A pharmacist intervention resulted in a statistically significant reduction in medication-related problems, and a non-significant reduction in acute health services use Rothman et al 23 2005 US RCT 217 Patients registered at a university general internal medicine practice with type 2 diabetes and poor glycaemic control (HbA1c level ≥8.0%) Primary care visits, urgent care visits, hospitalisations Pharmacist intervention resulted in statistically significant improvement in BP and glycaemic control, but had no statistically significant impact on the use of clinical services Rudd and Dier24 2010 US Retrospective medical record review 996 Patients registered at 25 outreach primary care health centres, receiving long-term anticoagulation therapy with warfarin Hospitalisations, ED visits Pharmacist anticoagulation management services resulted in a statistically significant reduction in rates of anticoagulation-related ED visits and hospitalisations, with financial impact through avoided costs. Sellors et al 35 2001 Canada Randomised, observer-blinded, controlled trial 132 Patients aged ≥65 years from four family practices, who were taking ≥4 regular medications Number of medications, medication costs Results suggested a statistically non-significant trend towards lower medication costs through face-to-face medication reviews carried out by pharmacists Sellors et al 36 2003 Canada RCT 48 family physicians and 889 patients Patients ≥65 years, taking ≥5 medications, registered in 24 family practices Number of medications, medication costs, healthcare costs The intervention did not demonstrate any statistically significant effect on health system outcomes. Physicians were receptive to recommendations on drug-related problems, suggesting feasibility of collaboration between physicians and pharmacists Siaw et al 48 2017 Singapore RCT 411 High–risk patients aged ≥21 years with uncontrolled type 2 diabetes, polypharmacy, and comorbidities; registered at four outpatient healthcare institutions Primary care visits, visit costs, laboratory test costs, medication costs Pharmacist intervention was associated with fewer physician visits, but slightly higher visit costs due to additional pharmacists visits. Overall healthcare costs were lower with pharmacist intervention, with medication costs the greatest contributor to this reduction. Simpson et al 37 2011 Canada RCT 260 Patients with type 2 diabetes registered at five primary care clinics Healthcare costs, ED visits, hospitalisations, specialist visits, healthcare contacts Pharmacist intervention was associated with statistically significant increase in healthcare-related contacts, but the majority of these were protocol-driven visits to the pharmacist as part of the intervention Simpson et al 38 2015 Canada RCT 123 Patients with type 2 diabetes registered at five primary care clinics ED visits, hospitalisations, specialist visits, healthcare contacts Adding pharmacists to primary care teams was a cost-effective strategy for reducing cardiovascular risk in patients with type 2 diabetes Stergachis et al 25 1987 US RCT 17 physicians Two clinical pharmacists working with patients registered in two family practices Medication costs Pharmacists were unable to produce statistically significant change in medication costs. This programme was not economically self-sustaining during the first 6 months Zermansky et al 42 2001 UK RCT 1188 Patients registered at four general practices, aged ≥65 years, receiving at least one repeat prescription Number of medications, medication costs, primary care visits, specialist visits, hospitalisations Monthly medication costs rose less in the pharmacist intervention group. Patients in the intervention group also had a statistically smaller rise in the number of medications prescribed than in the control group. BP = blood pressure. CCG = clinical commissioning group. ED = emergency department. NHS = National Health Service. QALY = quality-adjusted life year. RCT = randomised controlled trial. WTE = whole-time equivalent.
In this issue

British Journal of General Practice
Impact of integrating pharmacists into primary care teams on health systems indicators: a systematic review








Jump to section
More in this TOC Section
Related Articles
Cited By...
Intended for Healthcare Professionals

