Article Text

Abstract
After a stroke or transient ischaemic attack (TIA) there is a high risk of stroke, particularly in the early days and weeks, and of other serious vascular events. Several preventive medical treatments can reduce these risks; starting them as early as possible will maximise the absolute risk reduction, as long as the diagnosis is secure, there is no known or suspected net harm from treatment, and they are acceptable to the patient. Medical treatments with clear evidence of benefit include: lowering blood pressure after all types of stroke or TIA; lowering blood cholesterol with a statin after ischaemic stroke or TIA; antiplatelet treatment after ischaemic stroke or TIA; and warfarin instead of antiplatelet treatment in patients with ischaemic stroke or TIA who have atrial fibrillation and no contraindications to anticoagulation. Lifestyle changes (for example, stopping smoking, reducing excess alcohol intake, adopting a healthy diet) and careful management of diabetes are also important.
Statistics from Altmetric.com

People who have had an ischaemic stroke or transient ischaemic attack (TIA) are at substantial risk of stroke, and other serious vascular events. Recent studies have demonstrated that the very early risk of stroke is much higher than was previously thought: about 10% at one week, 14% at one month, and 18% at three months.1 Thereafter, the risk falls to around 5% per year, with in addition a 2–3% per year risk of myocardial infarction (MI).2–4 The annual long-term risks of stroke and other vascular events after an intracerebral haemorrhage are similar, but we do not know much about the very early risks.5
Twenty per cent of patients with ischaemic stroke have a preceding TIA or minor ischaemic stroke. With accumulating evidence for the beneficial effects of intervening very early, such non-disabling events provide a particular opportunity for prevention.1 Patients with a suspected stroke or TIA should therefore be seen as soon as possible to confirm the diagnosis, decide whether inpatient care is required, arrange appropriate investigations to establish the pathological type and subtype of stroke or TIA, and start preventive interventions promptly.
This article provides a guide to medical interventions for reducing the risk of stroke and other vascular events after an ischaemic stroke or TIA, or an intracerebral haemorrhage. Preventive treatments after subarachnoid haemorrhage, and specific interventions for unusual causes of stroke (such as arterial dissection or vasculitis) are not dealt with. Surgical and neuroradiological interventions have already been discussed recently in this journal.6
GETTING THE BLOOD PRESSURE DOWN
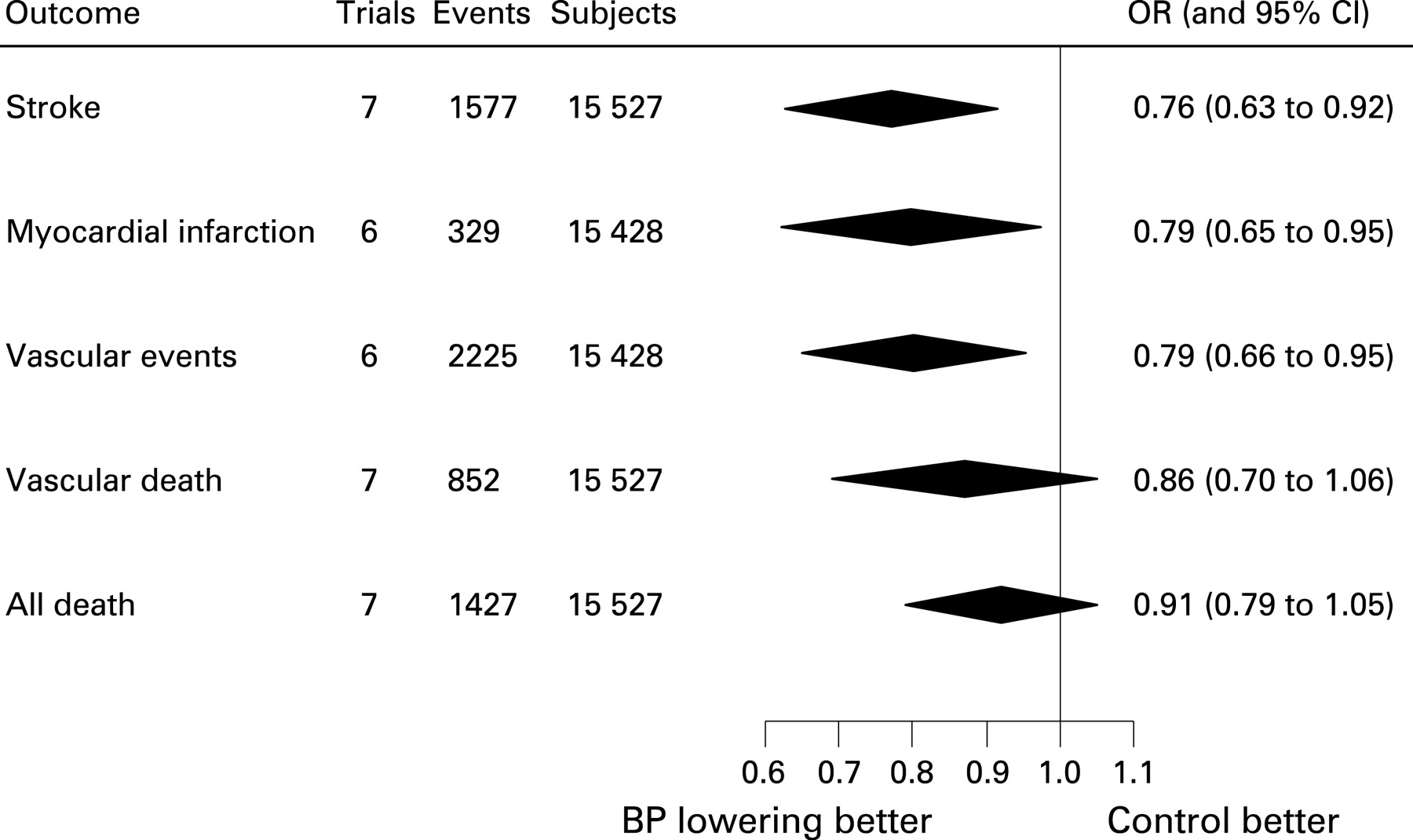
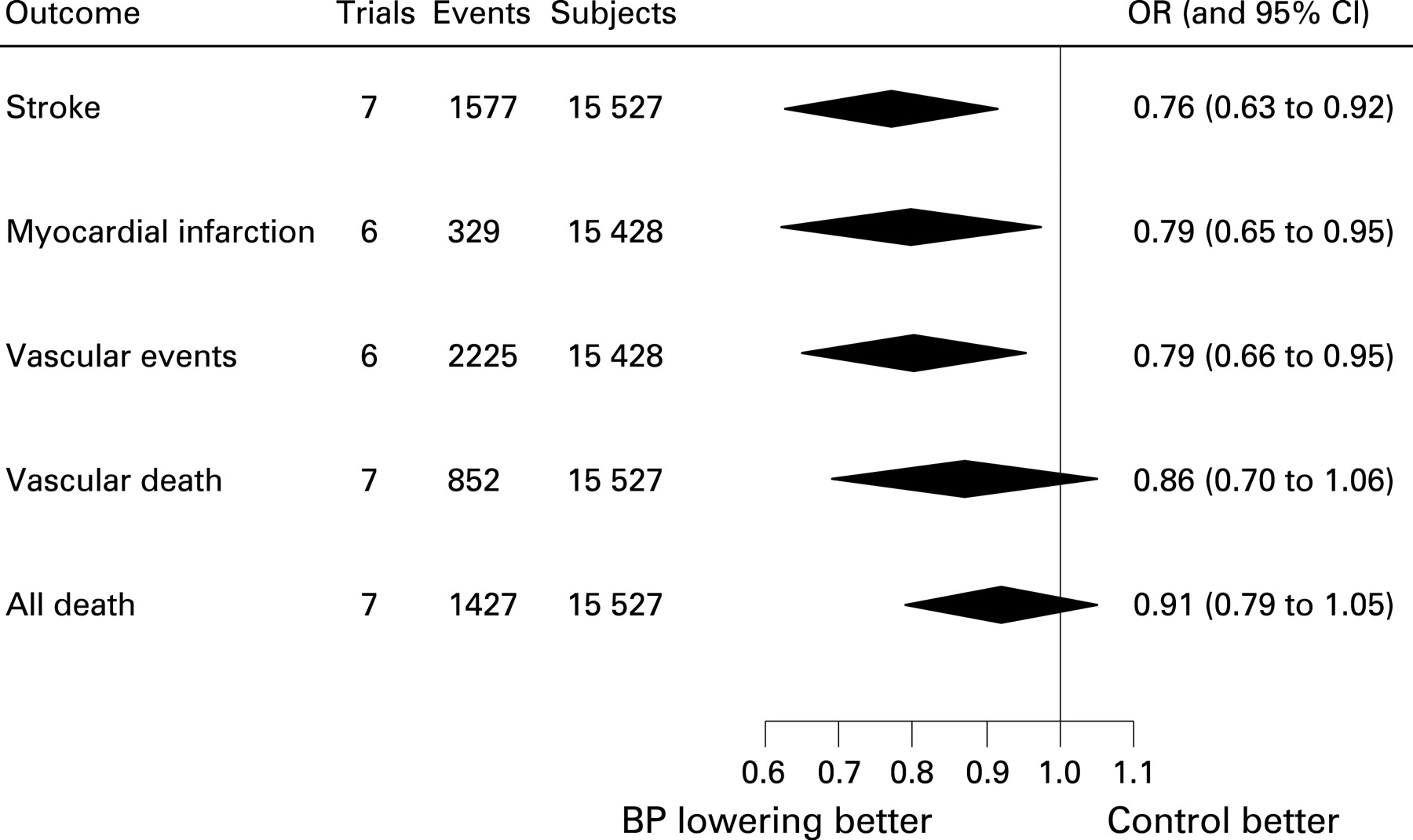
Increasing blood pressure is the most important modifiable risk factor for a first or recurrent stroke. There is now very good evidence from randomised controlled trials (RCTs) among patients with a prior stroke or TIA that pharmacological blood pressure reduction is beneficial: an average reduction of 8 mm Hg systolic and 4 mm Hg diastolic reduces the relative risk of recurrent stroke by about one quarter, and of serious vascular events (stroke, myocardial infarction or vascular death) by about one fifth (fig 1).7 For patients similar to those in the trials where the average annual control group risk of vascular events was about 5%, this corresponds to an absolute reduction of 1%, or 10 vascular events avoided per 1000 patients treated per year.7
Observational studies among people without a history of vascular disease, and among people with a prior stroke or TIA, have shown a continuous, log linear relation between usual blood pressure and stroke risk, which falls by about one third for every 10 mm Hg reduction in systolic blood pressure, with no lower threshold within the range observed.8, 9 Meta-analyses of randomised controlled trials (RCTs) of antihypertensive drugs among various different types of patients, including those with stroke or TIA, have confirmed that the more the blood pressure is lowered, the greater the reduction in risk of stroke, ischaemic heart disease and almost all other vascular outcomes (with the exception of heart failure) (fig 2).10

Who should be treated?
The RCTs in patients with stroke or TIA found that the relative benefits of lowering blood pressure were similar irrespective of baseline blood pressure, age, and pathological type of stroke.7 11 Blood pressure lowering medication should therefore be started—or additional medication added in those already taking antihypertensive drugs—in almost all patients who have had an ischaemic stroke, TIA or intracerebral haemorrhage, whether or not they would conventionally be considered hypertensive. However, it seems reasonable not to treat those whose blood pressure is consistently around 130/70 mm Hg or less. Only a small proportion of patients in the RCTs had baseline blood pressures lower than this, and the observational studies of the relation between blood pressure and stroke risk do not tell us about the nature of the relationship below this level.7–9
How far should the blood pressure be lowered?
The optimum benefit should be achieved by aiming to get the blood pressure down as far as about 130/70 mm Hg in as many patients as possible. In practice, this will not always be achievable in all patients, because of imperfect adherence, drug intolerance and so on. In addition, there is some observational evidence to suggest that, in patients with severe stenosis or occlusion of more than one extracranial carotid artery (and perhaps the same applies to the vertebral arteries), lowering blood pressure below about 140–150 mm Hg systolic/80 mm Hg diastolic may be associated with an increased risk of recurrent stroke.12 In such patients, it is sensible to proceed particularly cautiously and to avoid lowering the blood pressure below about 140/80 mm Hg, at least until any arterial stenosis has been dealt with.12
Which drug or drugs?
The drug regimens shown to be beneficial specifically in patients with a prior stroke or TIA were a thiazide, or the combination of a thiazide with an ACE-inhibitor.7 The benefit appeared to be related to the blood pressure reductions achieved by these drugs, rather than due to a class- or drug-specific effect.7 Therefore, the choice of drug or drugs to reduce the blood pressure is likely to depend on the patient’s age, what other drugs are being taken, drug intolerance and adherence problems, comorbidities, and so on. It is also worth remembering that combining drugs from different classes at low or standard doses, rather than increasing the dose of one drug, tends to maximise the blood pressure reduction while minimising adverse effects.13
So, if there are no contraindications, it is reasonable to start with a thiazide in no more than the standard dose (for example, bendroflumethiazide 2.5 mg daily), and then add an ACE-inhibitor if necessary. However, if necessary or specifically indicated, other antihypertensive drugs may be used. Beta blockers should generally not be used first line, because they may have a less favourable ratio of benefit to adverse effects.14
How soon after the stroke or TIA should treatment start?
While there are no doubts that the long-term reduction of blood pressure is beneficial, it is unclear whether the same is true very early after an acute stroke. RCTs are underway to address this question (see http://www.enos.ac.uk/ and http://www.le.ac.uk/cv/research/COSSACS/COSSACShome.html). In the meantime, it is reasonable to start antihypertensive drugs promptly in patients with a non-disabling stroke or TIA,1 but in patients with an acute stroke requiring admission to hospital it is probably best to wait for a week or two (or at least until the blood pressure has stabilised—it tends to fall spontaneously) because of the risk of reducing cerebral perfusion during the critical early period. However, malignant hypertension should be treated without delay, and it seems reasonable to continue antihypertensive drugs that were already being taken at the time of the stroke or TIA unless there are problems with hypotension.
How long should treatment continue?
The relevant RCTs suggest that the benefits of treatment are maintained for at least several years.7 11 Treatment should therefore continue long term, as long as it continues to be tolerated and is required to keep the blood pressure well-controlled.
GETTING THE CHOLESTEROL DOWN
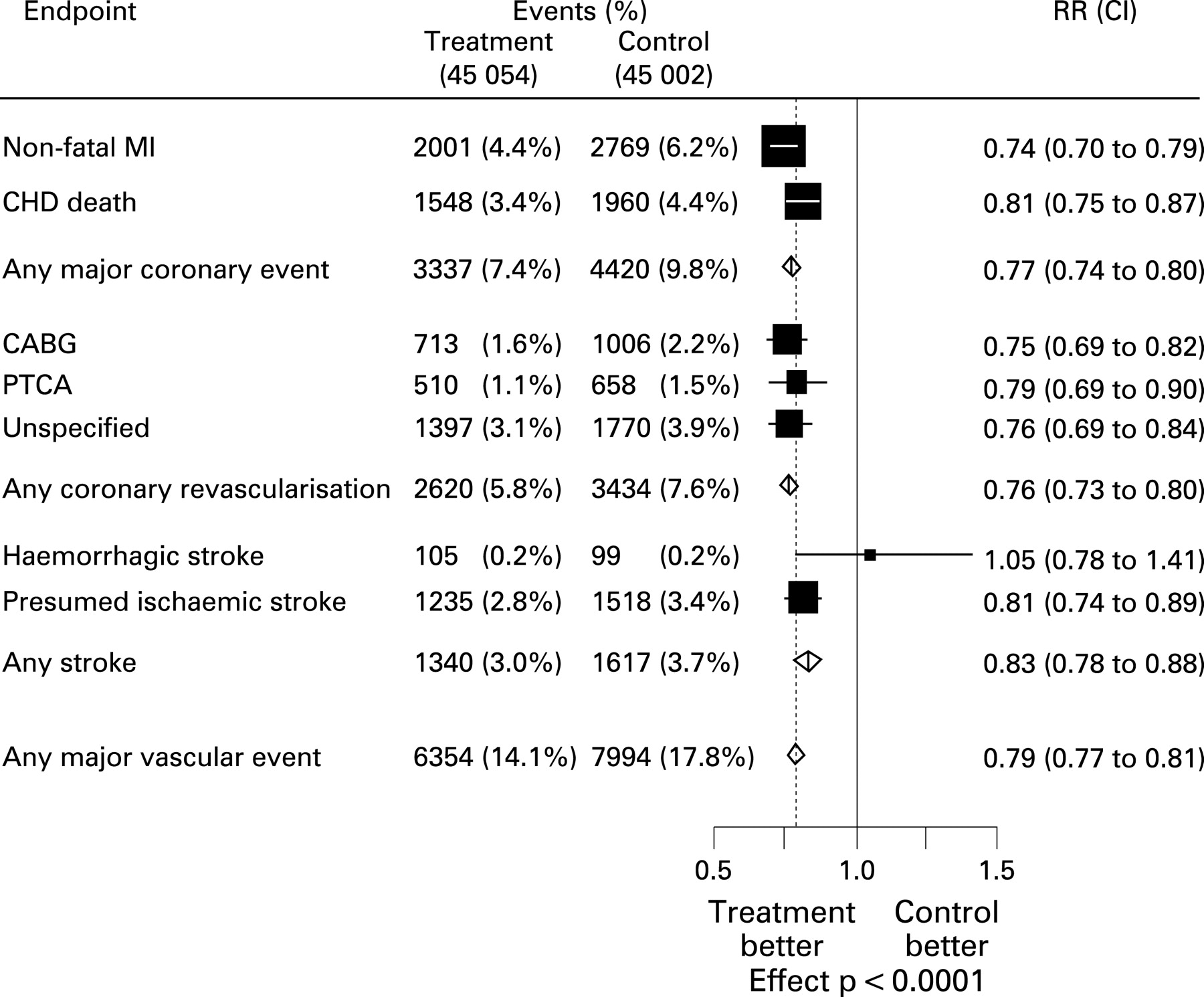
Large RCTs and systematic reviews have shown that reducing total (and more importantly LDL) cholesterol blood levels with a statin reduces the risk of vascular outcomes, including stroke. The Cholesterol Treatment Trialists’ (CTT) meta-analysis showed that a 1.0 mmol reduction in LDL produced highly statistically significant relative reductions in coronary events and revascularisations of almost a quarter, in stroke of 17%, and in the combined outcome of major vascular events (non-fatal MI, coronary death, coronary revascularisation or stroke) of about a fifth (fig 3).15 The 17% reduction in stroke reflected a 19% reduction in “presumed ischaemic” stroke (that is, ischaemic or unknown type) with no apparent difference in haemorrhagic stroke (fig 3). The relative reductions in vascular outcomes were proportional to the absolute reductions in LDL-cholesterol (analogous to the situation for blood pressure reduction—see above), and were similar irrespective of age and gender, previous history of ischaemic heart disease, diabetes or hypertension, and baseline lipid levels.15

Two large RCTs have specifically randomised patients with a prior (mainly ischaemic) stroke or TIA to a statin or placebo.16–18 The first, the Heart Protection Study (HPS), included over 3200 patients with a prior stroke or TIA among around 20 000 patients, all of whom were included in the CTT meta-analysis.16 17 The second and more recent, the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial, only included patients with a prior TIA or stroke (around 4700), and was not included in the CTT meta-analysis.18 Data for the stroke/TIA patients in both trials are shown in table 1. Both simvastatin 40 mg daily in HPS and atorvastatin 80 mg daily in SPARCL reduced LDL-cholesterol (by 1 mmol/l and 1.4 mmol/l respectively) and major vascular events. All types of stroke combined were reduced in SPARCL but not in the subgroup of patients with a prior stroke or TIA in the HPS (table 1) but the HPS results may have been a chance finding since this was one of several non-pre-specified subgroup analyses; in the main analyses of all 20 000 or so trial participants, simvastatin reduced the relative risk of all types of stroke by about 15%.16 17 In both trials, a reduction in risk of ischaemic stroke appeared to be partly offset by an increase in risk of haemorrhagic stroke. However, as this increased risk was not apparent in the CTT meta-analysis (fig 3),15 the effects of statin treatment on haemorrhagic stroke remain uncertain.
The average annual risk of a serious vascular event in the placebo groups in both trials was about 6%, so the observed relative reduction of around one fifth in this outcome produced an absolute reduction of about 12 vascular events avoided per 1000 patients treated per year.
Cholesterol lowering treatments do not increase the risks of cancer or suicide, and serious adverse effects of statin monotherapy (such as rhabdomyolysis or liver failure) are extremely rare.15, 19 However, the combination of a statin with a fibrate substantially increases the risk of rhabdomyolysis and should be avoided, or used only with extreme caution.20
Who should and who should not be treated?
HPS and SPARCL together provide secure evidence for routinely recommending cholesterol reduction with a statin in all patients with a prior ischaemic stroke or TIA with baseline total cholesterol >3.5 mmol/l, or LDL-cholesterol >2.6 mmol/l (table 1).16–18 In clinical practice, at least in European populations, it is rare to encounter patients with pre-treatment cholesterol levels below these cut-offs.
SPARCL recruited a very small number of patients with a prior intracerebral haemorrhage, not enough to assess the balance of benefits and hazards of treatment in these patients specifically. As reducing cholesterol levels may increase the risk of haemorrhagic stroke (see above), and because patients with a history of intracerebral haemorrhage are more likely to develop recurrent haemorrhagic than ischaemic stroke,21 cholesterol-lowering drugs should generally be avoided in patients with haemorrhagic stroke, unless they are at particularly high risk of future ischaemic vascular events, for example because of a history of ischaemic stroke or ischaemic heart disease.
Which statin and at what dose?
There are no direct comparisons of different statin regimens specifically in patients with a history of stroke or TIA, but indirect comparisons show that greater benefits arise from increasing LDL-cholesterol reductions.15 Direct randomised comparisons between intensive and moderate lipid-lowering statin regimens in patients with ischaemic heart disease confirm this, albeit at the expense of an increased risk of abnormal liver function tests.22 At present, it seems reasonable to use the HPS regimen of simvastatin 40 mg daily, or the SPARCL regimen of atorvastatin 80 mg daily for patients at particularly high risk of further ischaemic vascular events in whom the absolute benefit of increasing the intensity of cholesterol lowering treatment will be greatest, because these have been directly assessed in patients with a prior stroke or TIA. Cost may also influence the choice since, at least in the UK, atorvastatin is currently substantially more expensive than simvastatin.23 Sometimes, patients who cannot tolerate one particular statin can tolerate another, making it reasonable to use alternative statins to simvastatin or atorvastatin if necessary. Approximate equivalent doses of other statins to simvastatin 40 mg daily are shown in table 2.16
How soon after stroke or TIA should treatment start?
Although there is no specific evidence for the use of statins in the very early period after an ischaemic stroke or TIA, impressive reductions in ischaemic vascular events, including stroke, have been reported with their use within the first few days of acute coronary syndromes.24 Furthermore, there is no reason to suppose that the potential adverse effects of statins should be any greater early after an ischaemic stroke or TIA, while the high absolute risk of recurrence at this time should make the absolute benefits of treatment greater. It therefore seems reasonable to start a statin as soon as possible.
How long should treatment continue?
The full benefits of cholesterol lowering with a statin emerge over the first 2–3 years of treatment and continue for each year of treatment thereafter.15 It therefore makes sense for statin treatment to continue long term, assuming no contraindications develop.
The role of non-statin cholesterol-lowering drugs
Because the evidence for statins is more extensive and compelling than for other lipid-lowering drugs, these should generally be the first choice. For patients with very abnormal lipid profiles (very high cholesterol, triglycerides, or both), other lipid-lowering drugs such as anion-exchange resins, ezetimibe, or—with great caution because of the increased risk of rhabdomyolysis—fibrates may be used in addition. This is generally best done under the supervision of a lipid specialist. For patients unable to tolerate a statin, it seems reasonable to use an alternative drug to try to lower the LDL-cholesterol concentration to some extent, as this seems very likely to reduce the risk of vascular events.
ANTITHROMBOTIC TREATMENT
Both platelets and fibrin are important components of thrombi, and they are also involved in the process of atherogenesis itself. Antiplatelet drugs and anticoagulants should therefore reduce the risk not only of ischaemic stroke but also of myocardial infarction and other serious thrombotic events in both arteries and veins, such as intracranial venous thrombosis and pulmonary emboli. Their most important potential adverse effect is bleeding, particularly intracranial haemorrhage because it is so frequently fatal or disabling, and serious extracranial haemorrhage (mainly from the gastrointestinal tract). Therefore, the best outcome to assess the net benefit of antithrombotic treatment is probably “serious vascular events”—that is, stroke (both ischaemic and haemorrhagic), myocardial infarction or vascular death (including deaths from extracranial haemorrhage).
Antiplatelet treatment
The Antithrombotic Trialists’ (ATT) meta-analysis of RCTs comparing antiplatelet treatment with placebo or open control among many thousands of patients with a prior ischaemic stroke or TIA found relative reductions of about one fifth in serious vascular events. With an average annual control group vascular event rate in the relevant RCTs of about 7%, this translates into an absolute reduction of about 14 vascular events per 1000 patients treated per year. The absolute excess risk of major bleeding in the trials was <1 intracranial haemorrhage and 1–2 serious extracranial haemorrhages per 1000 patients treated per year. Thus, the overall benefits of treatment greatly outweigh the risks, and patients should be prescribed antiplatelet treatment routinely, unless there are clear contraindications or anticoagulants are more appropriate (see below).25
Who should not be treated with antiplatelet drugs?
Patients with recent gastrointestinal or other major bleeding, or with symptoms of active peptic ulceration should generally not receive antiplatelet drugs. Those with a definite allergy to aspirin or another antiplatelet drug should avoid it and use an alternative wherever possible. And those with neutropenia or thrombocytopenia should avoid the thienopyridines, clopidogrel and ticlopidine.
As antiplatelet drugs increase the risk of intracranial haemorrhage, it seems illogical to give them to somebody with a spontaneous or traumatic intracerebral haemorrhage. However, it seems reasonable to use antiplatelet treatment for secondary prevention in patients with an intracerebral haemorrhage who are at particularly high risk of future ischaemic vascular events, for example those with ischaemic heart disease or a previous ischaemic stroke.26, 27
How soon after ischaemic stroke or TIA should antiplatelet treatment start?
Two very large RCTs in patients within 48 hours of acute ischaemic stroke have shown net benefit from immediate aspirin.28 Early brain imaging is needed to exclude haemorrhagic stroke, preferably before any aspirin is given. In addition, it is probably best to avoid aspirin in the first week or two after acute ischaemic stroke with visible haemorrhagic transformation on brain imaging, although such patients should receive antiplatelet treatment in the long term. In the trials, 160 or 300 mg aspirin was given daily for the first two weeks, but it is perfectly reasonable to give this dose just once for rapid onset of action, and then reduce the dose to 75 mg daily for long-term treatment (see below). Patients with mild ischaemic strokes and TIAs were not included in the trials, but it seems entirely reasonable to assume that they will also benefit from this immediate treatment policy.
How long should antiplatelet treatment continue?
Although meta-analyses showed an apparent decline in benefit over several years of follow-up, this may be explained by decreasing adherence to treatment over time, and by bias in the comparisons in later years produced by the longer delay of vascular events in high-risk patients in the active treatment group.29 Thus, it seems sensible to continue treatment indefinitely in patients who remain at high risk of a serious vascular event, unless some contraindication develops.
Antiplatelet treatment: aspirin alone
Until about a decade ago, aspirin alone was the undisputed gold standard antiplatelet regimen for long-term prevention.25, 29 75 mg aspirin per day is as effective as higher doses and produces less adverse effects, although controversy remains about whether or not lower doses are as effective.25, 30
Antiplatelet treatment: alternatives to aspirin alone
There is still no evidence that any single alternative antiplatelet drug is definitely superior to aspirin alone.
Clopidogrel
A large RCT in patients with a history of ischaemic stroke, MI or peripheral arterial disease found the thienopyridine antiplatelet drug, clopidogrel, to be at least as effective as aspirin, and possibly somewhat more so.31 The two drugs have different adverse event profiles: aspirin produces more upper gastrointestinal adverse effects (haemorrhage, nausea, vomiting), while clopidogrel produces more diarrhoea and skin rash, and a very small (but not negligible) risk of thrombocytopenia and thrombotic thrombocytopenic purpura.31, 32 Because it is substantially more expensive than aspirin and not definitely more effective, clopidogrel should generally only be used in patients who are genuinely intolerant of or allergic to aspirin.33 Furthermore, in patients developing upper gastrointestinal adverse effects with aspirin, the addition of a proton pump inhibitor to aspirin is both safer and cheaper than switching to clopidogrel.34
Dipyridamole or triflusal
These antiplatelet drugs have both been compared directly with aspirin in randomised trials but neither drug reduces vascular events better than aspirin alone, and indeed they may even be inferior.25, 35
Aspirin plus clopidogrel
RCTs have found that, in long-term secondary prevention, this combination does not reduce vascular events but produces more haemorrhages than either clopidogrel or aspirin alone.36, 37 However, the combination may perhaps be beneficial very early after ischaemic stroke or TIA when the recurrence risk is particularly high.37 This needs confirmation from further RCTs, but it would be in keeping with the benefit after acute coronary syndromes or coronary catheterisation,38 and with a randomised trial showing that adding clopidogrel to aspirin reduced transcranial Doppler ultrasound signals (thought to represent asymptomatic emboli) in patients with severe carotid stenosis.39
Aspirin plus dipyridamole
Although RCTs of aspirin plus dipyridamole versus aspirin alone before the mid-1990s did not find the combination to be superior (due perhaps to the play of chance and insufficient statistical power, or to the lower dose and standard formulation of dipyridamole then in use),25 two subsequent large RCTs found that in patients with a prior ischaemic stroke or TIA, the combination of aspirin and dipyridamole (specifically modified-release dipyridamole 200 mg twice daily) reduced the risk of vascular events by about one fifth compared with aspirin alone, without any increase in major bleeding (fig 4).40 Thus, in patients able to take aspirin, it is appropriate to consider the addition of modified-release dipyridamole 400 mg daily, as long as the patients can manage more pills and consider the additional absolute benefit worthwhile.40 In the more recent of the two RCTs, the annual risk of a vascular event in the aspirin-only treatment arm was about 5%, falling to 4% in the aspirin plus dipyridamole arm, a reduction of 10 vascular events per 1000 patients treated with the combination per year.40 Patients should be warned of the risk of dipyridamole-related headache, which occurs in up to a third of patients, but it usually settles in 1–2 weeks.40 Although a combined preparation of 200 mg modified release dipyridamole and 25 mg aspirin, designed to be taken twice daily, is available, physicians (like me) who are more comfortable with continuing a daily aspirin dose of 75 mg can advise their patients to add 200 mg modified release dipyridamole twice daily separately.23

Anticoagulants in patients without atrial fibrillation
In patients with a presumed non-cardioembolic prior ischaemic stroke or TIA (essentially those without atrial fibrillation), RCTs mainly in the 1960s and 1970s comparing long-term treatment with anticoagulants (generally oral anticoagulants) versus control, and in the 1990s and 2000s comparing oral anticoagulants (mainly warfarin, with target INR covering the range 1.4–4.5) with antiplatelet treatment (mainly aspirin) found that anticoagulants increased the risk of haemorrhage compared with either control or aspirin without any clear evidence of net benefit.41, 42 Anticoagulants should therefore not be used for the long-term prevention of recurrent stroke and other vascular events.
Anticoagulants in patients with atrial fibrillation
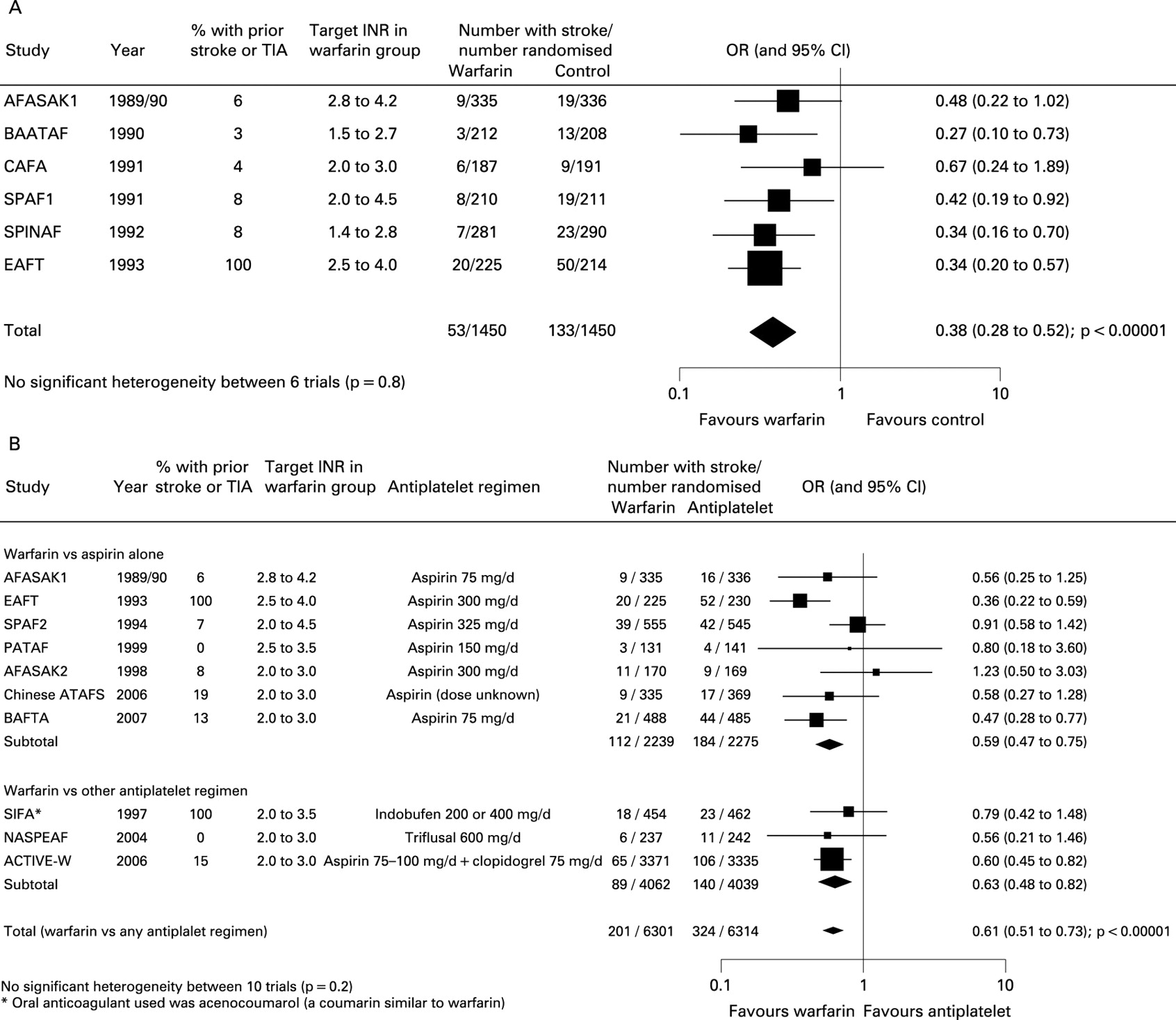
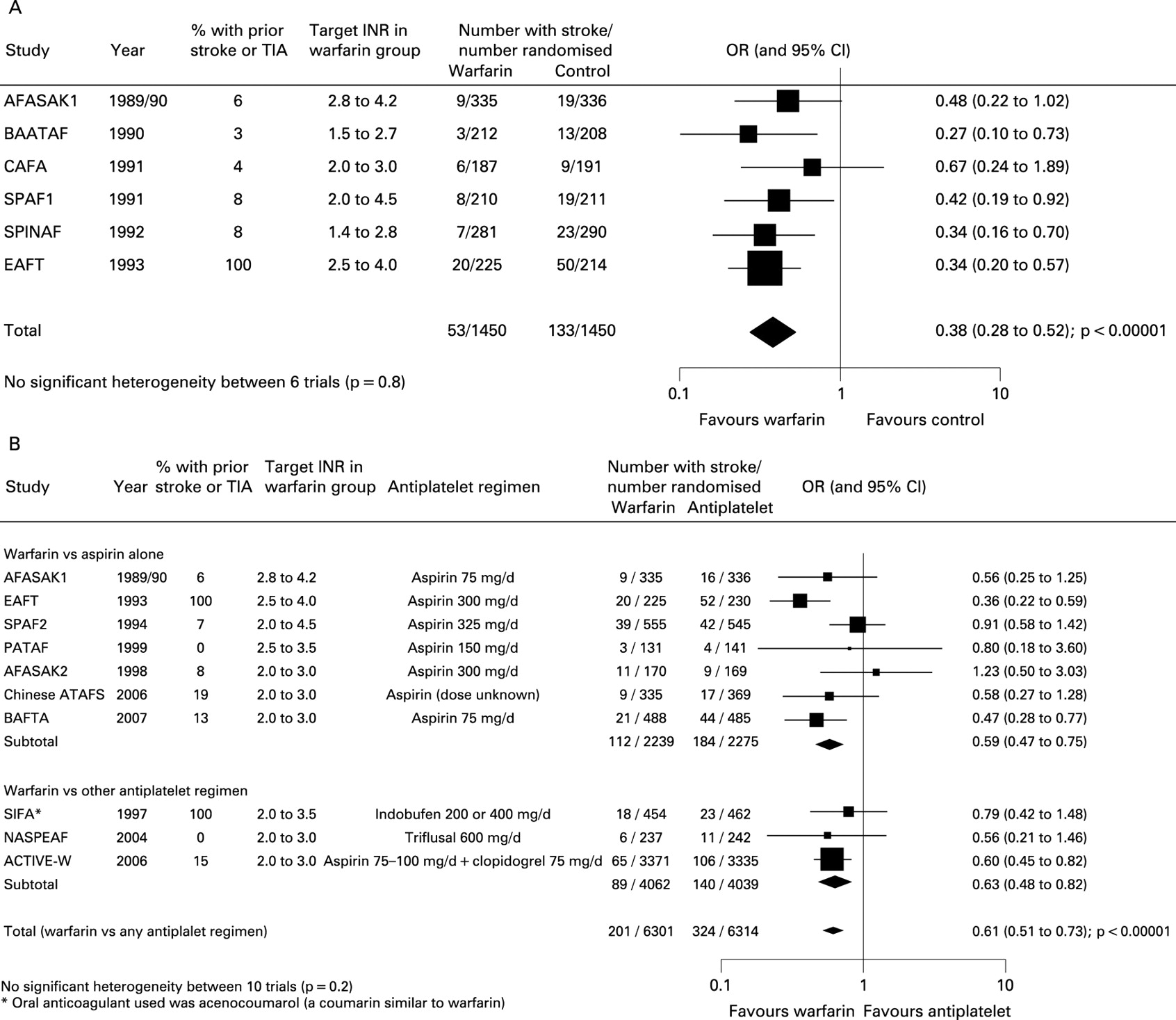
By contrast, there is clear evidence supporting the use of oral anticoagulants for prevention of stroke and vascular events in patients with atrial fibrillation (including those with paroxysmal atrial fibrillation or atrial flutter). This comes from RCTs comparing oral anticoagulants with control, and with antiplatelet treatment (mainly aspirin alone).43, 44 My updated meta-analysis for the purposes of this review and incorporating all relevant RCTs with over 100 participants, followed up for at least three months and with published data available at the time of writing, found that oral anticoagulants (mainly warfarin, with an average INR of about 2.5) reduced the relative risk of stroke (ischaemic and haemorrhagic combined) by about two thirds compared with control, and by about 40% compared with antiplatelet treatment (fig 5). These benefits were apparent in those both with and without a prior ischaemic stroke or TIA, and in all age groups, the most recent trial showing that the advantages of warfarin over aspirin did not diminish with increasing age up to 85 years and over.44 Because patients with a history of ischaemic stroke or TIA and atrial fibrillation are at substantial risk of stroke (about 12% per year in the control arms of the relevant trials), the absolute risk reductions in these patients are substantial: about 70 strokes prevented per 1000 patients treated for a year with oral anticoagulants rather than control, and about 50 strokes prevented per 1000 patients treated for a year with oral anticoagulants rather than antiplatelet treatment. Excess risks of major extracranial haemorrhage with anticoagulants versus control or antiplatelet treatment in the RCTs were an order of magnitude smaller than the benefits, about 2–3 per 1000 per year.43, 44
Thus, in the types of patients with a history of an ischaemic stroke or TIA included in the trials, the benefits of adjusted-dose warfarin with a target INR of around 2.5 far outweigh the risks, so long as there are no contraindications. Below about 2.0, the risk of ischaemic stroke increases, while above about 3.0 there is an increased risk of major bleeding.45, 46 Clearly, high-quality monitoring and management of anticoagulation are required to maintain the net benefit and low rate of adverse effects.
Anticoagulants in patients with atrial fibrillation: who not to treat
Because of the increased risk of anticoagulant-related haemorrhage, contraindications include recent gastrointestinal bleeding, alcoholic liver disease, confusion or dementia, tendency to falls, and difficulty accessing an anticoagulant clinic.45, 46 There is some evidence to suggest that extensive leukoaraiosis and the presence of brain microbleeds on brain imaging are associated with an increased risk of intracerebral haemorrhage, but as yet there is not enough information to know whether these features should influence decisions about using of oral anticoagulants.45–47 As discussed above for antiplatelet treatment, most patients with a history of intracerebral haemorrhage should not take anticoagulants, but they may be appropriate for those with a particularly high risk of future ischaemic vascular events.27 Some patients consider that the inconvenience of taking an oral anticoagulant, with the need for careful monitoring, outweighs the potential benefits. For patients unable or unwilling to take anticoagulants, aspirin is a reasonable alternative, albeit less effective.25, 43
The addition of antiplatelet treatment to anticoagulants
Randomised controlled trials suggest that the combination of oral anticoagulants with aspirin or another antiplatelet drug should generally be avoided because of the increased risk of major bleeding.48 However, the greater benefit of the combination may outweigh the bleeding risk in some patients at particularly high risk of thromboembolism (for example, those with mechanical heart valves).49, 50
How long should oral anticoagulants continue?
Most of the trials lasted only a few years and none directly compared different treatment durations. In the absence of clear evidence on this issue, it seems reasonable to continue anticoagulants indefinitely if a patient remains at high risk (whatever their age), no bleeding events have occurred, and no factors that might increase the risk of bleeding (such as dementia or a tendency to falls) have developed.
What about rhythm control for patients in atrial fibrillation?
Despite theoretical attractions, in particular the avoidance of long-term anticoagulants, RCTs do not suggest any definite advantage of either electrical or pharmacological cardioversion over rate control with long-term anticoagulation, and there may be some excess risks of pharmacological rhythm control. Thus rate control (plus anticoagulation if possible, and antiplatelet treatment if not) is a highly acceptable strategy for most patients.51, 52
LIFESTYLE MODIFICATION
Smoking
Given the clear association between smoking and a range of serious illnesses, including stroke, all smokers, including those with a history of stroke or TIA, should be advised to stop. Stopping smoking halves the risk of mortality due to ischaemic heart disease within a year, and the risk of stroke declines substantially within 2–5 years. RCTs and systematic reviews support the use of interventions such as counselling, nicotine replacement and antidepressants.53
Alcohol
Everyone, including those who have had a stroke or TIA, should avoid heavy drinking, but observational data suggest that a couple of units of alcohol per day may protect against future vascular events, including stroke, so it is safe for light drinkers to continue.54
Dietary modification
Overweight individuals should be encouraged to lose weight using dietary—or if necessary pharmacological or surgical—interventions, and all patients should receive general advice about a healthy diet, low in saturated fat and salt, with plenty of fish, fibre, fruit and vegetables. RCTs have shown beneficial effects on vascular risk factors which seem likely to translate into small reductions in vascular outcomes.55 In particular, reducing dietary salt and saturated fat intake produces small reductions in blood pressure and cholesterol levels respectively.56, 57
Exercise
There is no evidence that exercise reduces the risk of recurrent stroke or other vascular events, but there may be other benefits such as increased well-being and reduced risk of falls. It seems reasonable to encourage patients to return to normal physical activities as much as possible after a stroke.
Dietary supplements
At present there is no evidence to support the use of homocysteine-lowering with folate supplements or of antioxidant supplements to prevent vascular events.58–60
MANAGEMENT OF DIABETES MELLITUS
Randomised controlled trials show that good glycaemic control in patients with diabetes reduces the risk of microvascular—and may reduce the risk of macrovascular—complications.61–63 This will usually be most appropriately done in a specialist diabetes clinic.
IMPLEMENTING THE TREATMENT RECOMMENDATIONS IN PRACTICE
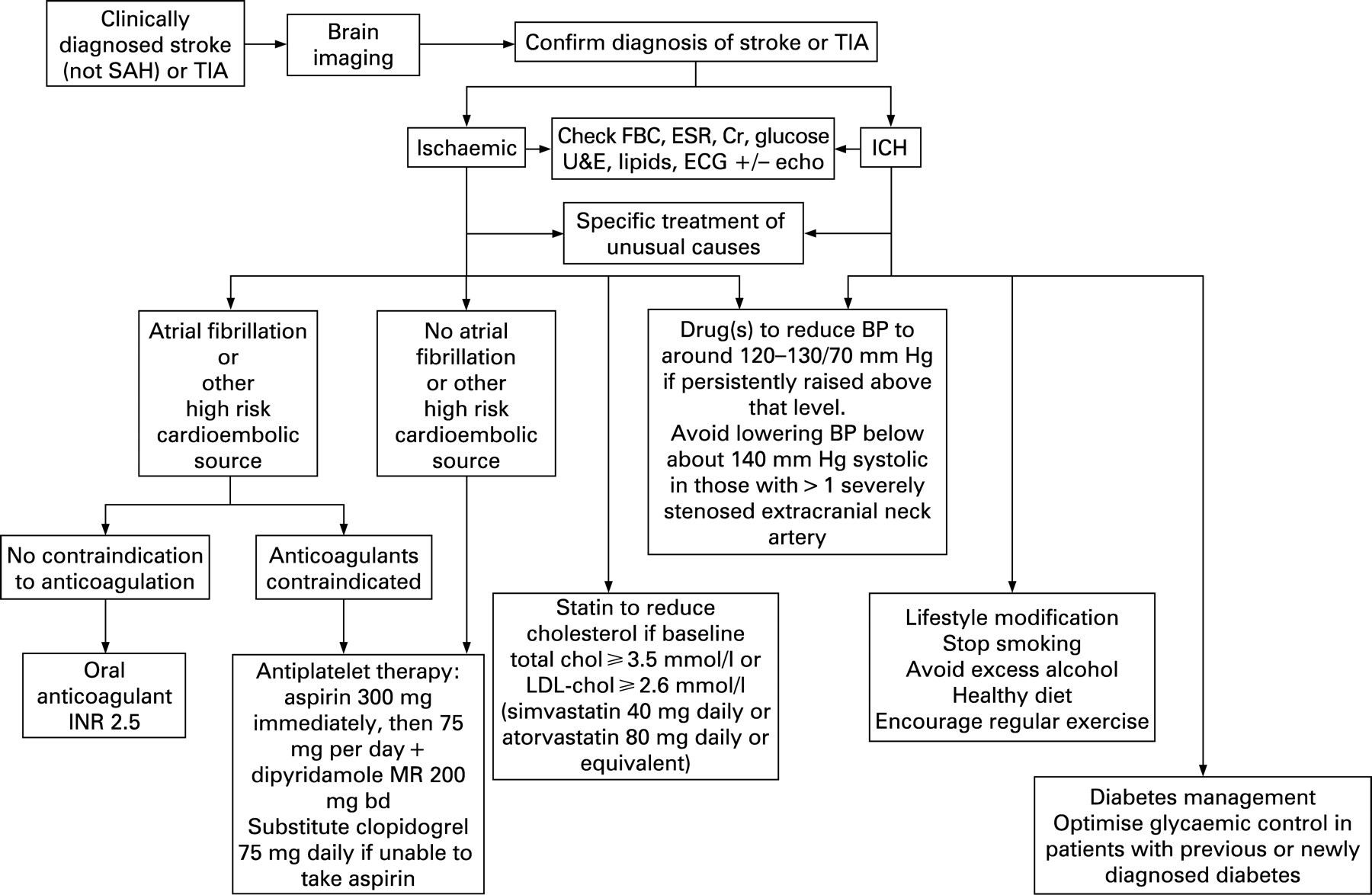
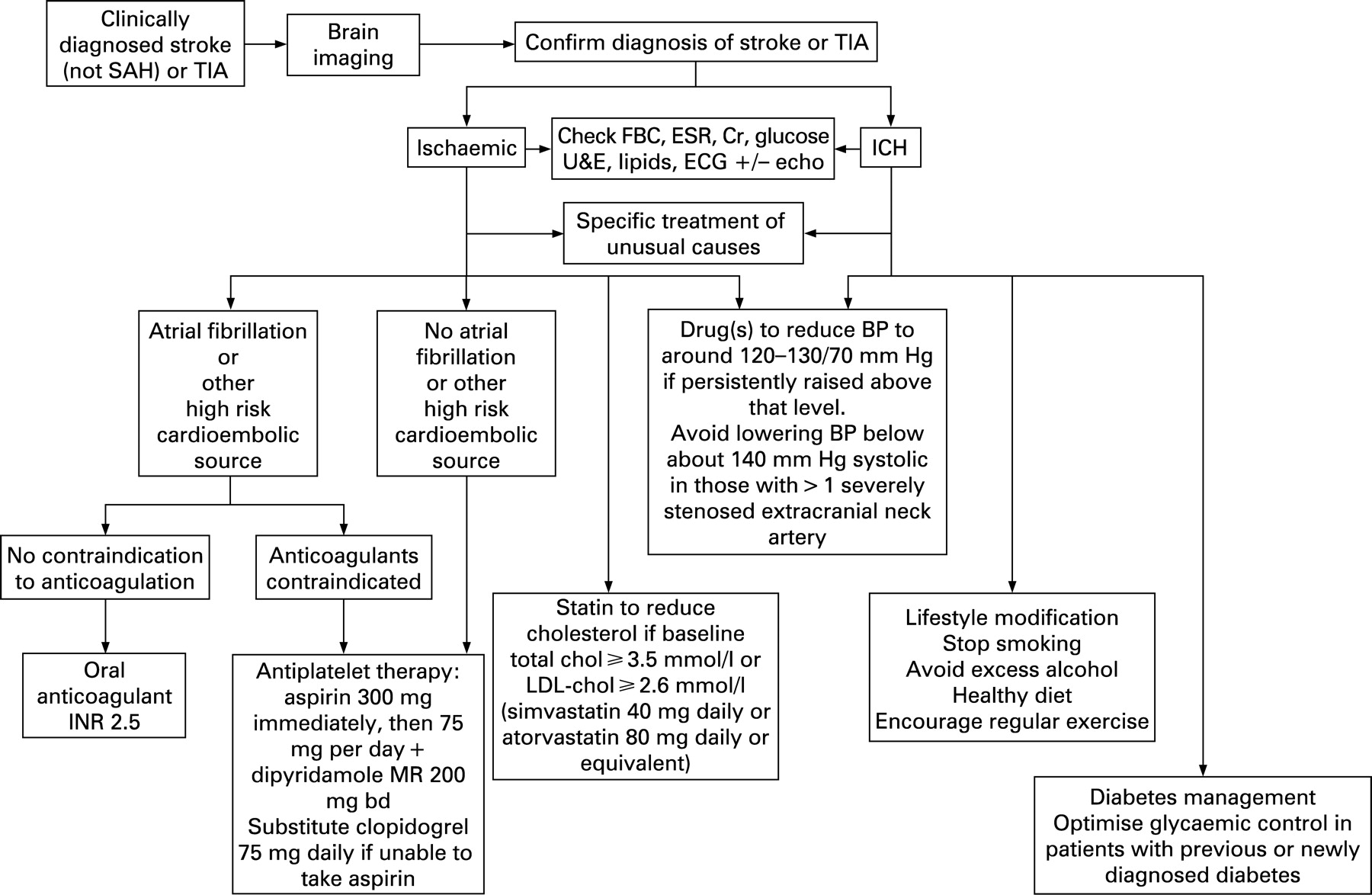
Figure 6 summarises the treatment recommendations given in this article. However, this is not a recipe and treatment must be tailored to the individual patient. For example, although supported by good evidence, the combination of two antiplatelet drugs, a statin, and possibly several antihypertensive drugs may not be appropriate for all patients in sinus rhythm with a history of ischaemic stroke or TIA. Managing large numbers of pills each day may be particularly difficult for very elderly patients (who are often under-represented in the trials), especially those with cognitive impairment, while for some patients the small absolute gain obtained from the addition of yet one more drug may simply not seem worthwhile.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
To illustrate the reduced absolute benefit to an individual patient from the addition of each new treatment, and the influence of the order and timing of introduction of various treatments in relation to the rapidly falling risk of a further vascular event in the early weeks, consider the case of a patient with a non-disabling ischaemic stroke shown in the box above and table 3 (this table is difficult and needs to be taken slowly!). The time after the stroke to starting each of the various treatments is particular to this case (see box), and might well vary depending on factors such as whether the patient is admitted to hospital, and how quickly various investigations are obtained and communicated to those initiating the treatments. The principles, however, are that:
each new treatment adds approximately the same relative reduction in risk of a vascular event (20%);
the absolute risk reduction depends on what the patient’s absolute risk is at the time of adding the new treatment;
the patient’s absolute risk at any particular time depends both on the time since their event (falling rapidly during the early weeks and then stabilising) and any treatment already started.
The case (see table 3)
A 75-year-old female on no regular medication experiences acute right-sided weakness and speech disturbance, with near complete recovery over the next few days. Two days after onset, she sees her general practitioner (GP), who makes a diagnosis of likely ischaemic stroke, starts aspirin 75 mg daily and refers her to the local rapid access stroke specialist clinic. When she is seen there 5 days later (7 days after onset), the specialist makes a clinical diagnosis of carotid territory stroke, and finds her to be in sinus rhythm with a clinically normal heart and a blood pressure of 140/83. A CT brain scan confirms that the stroke was ischaemic and ultrasound shows some minor atheroma of both carotid bulbs but no significant stenosis. Blood tests reveal a normal full blood count, ESR and renal function, random blood glucose of 5 mmol/l and cholesterol of 5.2 mmol/l. The specialist gives the patient some written information about stroke and lifestyle advice, and recommends the addition to her aspirin of a statin (simvastatin 40 mg daily) and modified release dipyridamole 200 mg twice daily, with the introduction over the next week or so of blood pressure-lowering drugs if her blood pressure remains persistently above about 120–130/70 mm Hg, the suggested first-line treatment being a thiazide diuretic plus an ACE-inhibitor if needed. The GP introduces this medication a week later.
Table 3 shows that treatments started earlier are associated with a larger absolute benefit than those started later, and that the absolute benefit from each treatment separately and all treatments combined during the first year (which incorporates the early high-risk period) is larger than during subsequent years of treatment. However, while it is important to start appropriate treatments as early as possible to maximise benefit, a delay between starting different new treatments may be necessary or at least sensible, even in a well-streamlined clinical service, to allow the patient to get established on one drug without experiencing adverse effects before the next is introduced, and to give time for a few repeat measurements of blood pressure before deciding whether or not to treat, and so on.
Practice points
Patients with a suspected stroke or TIA should be assessed, diagnosed, investigated and started on appropriate treatment as quickly a possible.
Blood pressure lowering after a stroke or TIA is of net benefit, down to about 120–130 mm Hg systolic/70 mm Hg diastolic in most patients.
Take care with lowering blood pressure very early after a disabling stroke (best to wait a week or two) and in lowering blood pressure too far or too fast in those with severe bilateral carotid stenosis.
Cholesterol lowering with a statin benefits patients with a history of ischaemic stroke or TIA and an untreated cholesterol level of >3.5 mmol/l.
Aspirin 300 mg acutely and then 75 mg daily reduces the risk of vascular events in patients with ischaemic stroke or TIA.
Clopidogrel 75 mg daily is a suitable alternative for patients genuinely intolerant of aspirin.
When added to aspirin, modified-release dipyridamole 200 mg twice daily further reduces risk of vascular events, and although headache is a common adverse event, this is said to be transient.
All of the above preventive treatments reduce the relative risk of vascular events by about one fifth. The absolute risk reduction achieved depends on how soon after stroke or TIA treatment is started and what treatments the patient is already taking to reduce their risk.
It is important not to forget the role of lifestyle modification (smoking, alcohol, diet etc) and careful management of diabetes.
Acknowledgments
This article was reviewed by Graeme Hankey (Perth, Australia), Craig Anderson (Sydney, Australia) and Jane Armitage (Oxford, UK) who have all contributed earlier but separate articles to Practical Neurology on secondary stroke prevention.
REFERENCES
Footnotes
Funding: The author was supported by a Wellcome Trust Clinician Scientist Award (063688).
Other content recommended for you
- Drugs to prevent vascular events after stroke
- Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients
- Prevention of ischaemic stroke
- Concurrent intracranial and extracranial artery stenosis and the prognosis of transient ischaemic symptoms or imaging-negative ischaemic stroke
- Should I start all my ischaemic stroke and TIA patients on a statin, an ACE inhibitor, a diuretic, and aspirin today?
- Retinal microvascular signs and recurrent vascular events in patients with TIA or minor stroke
- Antithrombotic and interventional treatment options in cardioembolic transient ischaemic attack and ischaemic stroke
- Long term risks of stroke, myocardial infarction, and vascular death in “low risk” patients with a non-recent transient ischaemic attack
- Antiplatelet regimens in the long-term secondary prevention of transient ischaemic attack and ischaemic stroke: an updated network meta-analysis
- Antithrombotic treatment in atrial fibrillation