Article Text

Abstract
Background: Acute asthma episodes prompting consultation with general practitioners in the sentinel practices of the Weekly Returns Service (WRS) of the Royal College of General Practitioners increased through the 1980s and early 1990s, reaching a peak in 1993.
Aims and Methods: To report on trends in the incidence of asthma episodes in children reported to the WRS over the period 1980–2002.
Results: Data confirm the steady upward trend from 1980 to 1993. The downward trend since 1993 was consistent in both male and female preschool and school age children, in all regions of the country simultaneously, and during all seasons until 1999 since when it has stabilised. No causative factor has been identified and no temporal association found between factors previously postulated as causing the increase in acute asthma. The decline in acute asthma episodes in children is consistent with observed declines in all other respiratory infections in this community.
Statistics from Altmetric.com
Asthma is the most common chronic childhood respiratory disorder affecting 10–15% of schoolchildren in the developed world.1–4 It is now perceived as a public health problem affecting all developed countries.5 A variety of studies using different methodologies and different populations have all shown a real increase in the cumulative prevalence of asthma within the community.1–6 Hospital admissions for acute childhood asthma increased substantially between 1970 and 1990; acute asthma is responsible for 10–20% of all acute medical admissions to paediatric wards.7 It is an important cause for school absence, restricted activity, and anxiety for child and family.4 There are 20–30 deaths from asthma in children each year in the UK. Prescriptions for asthma are among the most expensive burden on the NHS, costing some £548 million in 1997 which compares with £206 million for antibacterials, £43 million for oral contraception, or £26 million for eczema and psoriasis medications.8 A number of aetiological theories have been advanced which essentially identify temporal associations between the rise and suggested causative factors, though without additional evidence temporal associations are not necessarily causal.
The majority of reports showing a rise in childhood asthma are based on either hospital studies where there is an uncertain and variable population denominator or parent questionnaires where there is uncertainty regarding the quality of clinical information.6 Sufferer based questionnaires do not always distinguish clearly between point prevalence (do you suffer from wheeziness now?) and cumulative prevalence (have you ever suffered from wheeziness?). An alternative tool to understand the pattern of active childhood asthma is the Weekly Return Service (WRS) of the Royal College of General Practitioners,9 which was established to monitor new episodes of illness, particularly to warn of epidemic conditions but also to provide data referable to environmental and meteorological conditions. For this purpose data on new attacks of asthma are more appropriate than data on first diagnosis or data on consultations, many of which are delivered when the condition is quiescent. The WRS provided an early indication of increasing trends in episodes of acute asthma and acute bronchitis in the early 1980s.10 It has also recently identified a decline in acute episodes of asthma and acute bronchitis in all ages between 1994 and 1996.11 There was no evidence of diagnostic transfer between acute bronchitis and acute asthma. We here report the rate of acute episodes of asthma in children presenting to general practitioners in the WRS between 1980 and 2002.
METHODS
The WRS is a network of general practices well distributed throughout England and Wales reporting from every consultation. Surveillance populations over the period were approximately 180 000 in each of three regions: North, Central, South (defined arbitrarily by lines on a map linking Liverpool with Hull and Bristol with Ipswich). Six per cent of the population were aged 0–4 years and 13% were aged 5–14 years: the age and gender distribution was similar to the national census population.
The general practitioners (and practice nurses) report the morbidity problem(s) at each consultation as a Read code together with its consultation or episode type differentiating new episodes of illness from ongoing problems. A new episode is defined as the initial contact in an illness episode; data on consultations for routine management review are collected and processed separately. Over the period of the study this provides population based, medically certified diagnoses for all patient contacts every week from approximately 110 000 children. We have abstracted information on new episodes of asthma for children aged 0–4 years and 5–14 years expressed as a proportion of the child population registered.
The weekly rate of acute asthma episodes per 100 000 child patients registered on the practice lists was analysed to produce an annual trend. Having previously identified the peak incidence in 1993, we examined seasonal patterns of acute asthma episodes in each subsequent year in three-week moving average incidence rates. In the interest of clarity we present data for three years, 1994, 1997, and 2000. Since 1994, the network has collected gender specific data in each age group and region which we include in this report.
RESULTS
Figure 1 shows the aggregated annual trends for acute asthma episodes for children aged 0–4 and 5–14 years. As example years, there were 6576 episodes (age 0–14) reported in year 1994, 4962 in 1997, and 3075 in 2000. This confirms that there had been a steady upward trend in the rate of acute asthma episodes reported between 1980 until the spring of 1993 for acute asthma (and early in 1994 for acute bronchitis11). Subsequently, there has been a downward trend until 1999, since when rates have stabilised in both of the age groups examined.

Episodes of asthma in general practice; mean weekly incidence by year.
To determine whether the decline was due to disappearance of a particular seasonal segment, the weekly return data on asthma episodes were examined by week for the years 1993–2000 and illustrated with data for three example years in ages 0–4 (fig 2) and 5–14 (fig 3). This analysis shows that there were six peaks of acute asthma episodes throughout the calendar year and that a decline in the rate of new episodes has occurred uniformly across the seasons—all of the peaks are at a lower level; no one seasonal “epidemic” has disappeared to account for the lowered rate.

Episodes of asthma in general practice; children aged 0–4 years (3 week moving average).

Episodes of asthma in general practice; children aged 5–14 years (3 week moving average).
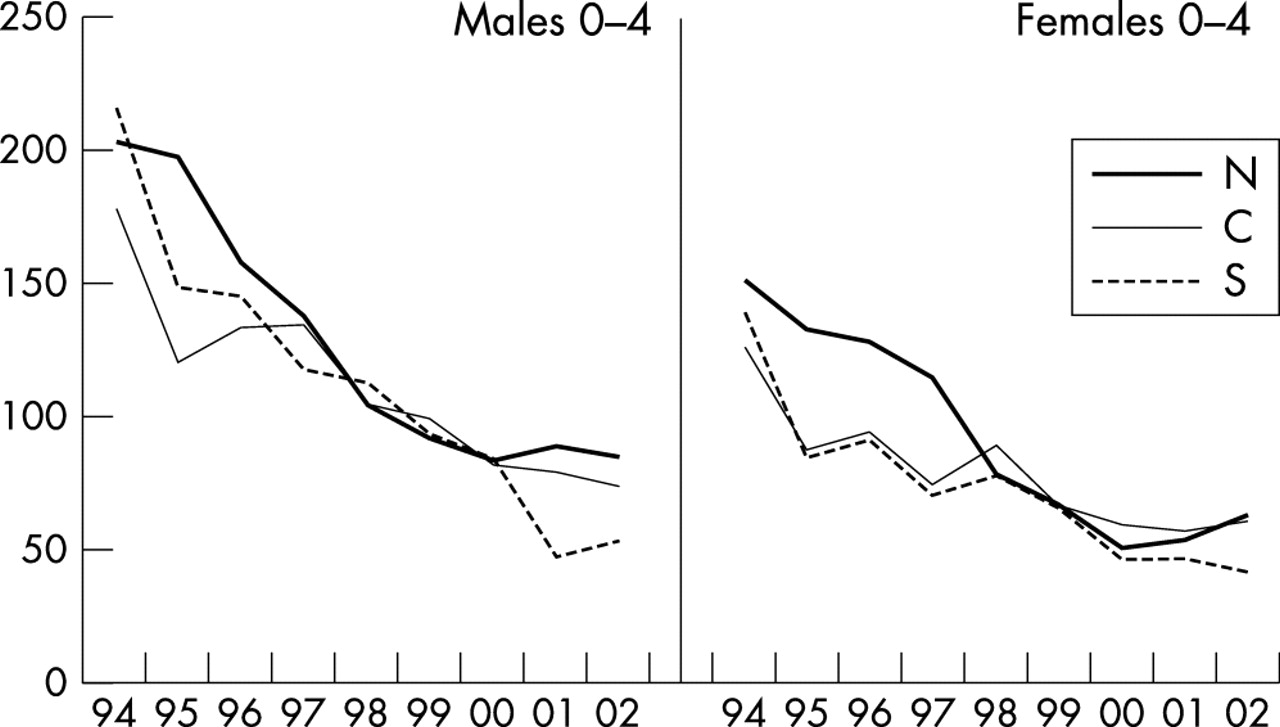
Analysis of the data in the three regions (North, Central, South), by gender and age (0–4 years, fig 4; 5–14 years, fig 5) shows the decline until 1999 to be consistent in all regions and in both age and gender groups. Regional rates also show recent evidence of stabilisation. Incidence was higher in males than females, especially in preschool children, and higher in preschool children than in the older age group.

Mean weekly incidence of asthma episodes by region and gender; children aged 0–4 years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean weekly incidence of asthma episodes by region and gender; children aged 5–14 years.
DISCUSSION
This study shows conclusively that the incidence of new episodes of asthma in children presenting to general practitioners in England and Wales increased between 1980 and 1993, corroborating the increased prevalence reported by others.1–5 The incidence subsequently declined continuously until 1999, although it may now be levelling off (fig 1). The decline occurred simultaneously at all seasons, in both preschool and school aged children and in all regions of the country. These three facts combined cannot be explained by local changes in management or clinical practice.
There have been concerns that the reported “epidemic” of asthma was merely a diagnostic transfer from previous diagnoses such as wheezy bronchitis. The WRS has a special strength in refuting this suggestion. Analysis of trends for both acute bronchitis and acute asthma episodes showed no evidence of diagnostic transfer.10,11 The WRS is based on continuous recording in a limited number of practices with infrequent practice changes optimising its usefulness in monitoring trends. Many practices have been included for more than 15 years, recording discipline is well established and consistent; the practice location and environment is constant, though a few patients change address each year (approximately 7%). As in all longitudinal paediatric studies, age group specific populations change every year.
It is tempting to speculate that changes in medication, especially the increased use of inhaled steroids, may be responsible for the reduction in rate of acute asthma episodes. The available evidence to date however shows a continued increase in prescribing of both bronchodilators and inhaled steroids.8 We can find no temporal association between national changes in management of asthma and the observed decline in rate of acute episodes. However, confidentiality protocols prevent identification of individual children in these data which precludes exclusion of the possibility of some individual change (such as a new treatment).
We have previously argued that asthma may also be declining in severity.11 A further possibility—that there has been a significant change in the vulnerability or biological constitution of children—seems implausible in the short time scale but cannot be excluded. The congruence of the decline with boys and girls might argue against a genetic factor. Acute asthma episodes were reported more frequently in male than female children, whereas in adults the opposite applies.11–14 The finding of these well known gender differences in the present data provides further validation of the sentinel practice database.
These data are more consistent with a significant change in the causative factors of asthma. Reduction in family size would reduce the likelihood of nosocomial infection, but the increasing availability of nursery places in Britain after 1996 would act the other way, increasing the chance of respiratory droplet infections. Pathogens may change in virulence and this may be relevant to understanding the trends we have shown. The decline in acute asthma episodes in childhood is consistent with the observed decline in all respiratory infections.15 Improvements in air quality may be significant, but the data show a decrease of asthma at all times of the year and not solely at those times we associate with poor air quality. Reduced passive smoking may also be a factor, and this is less dependent on seasonal variation.
It could reasonably be asked why this decline in acute asthma episodes has not been reported previously. We initially considered that the reversal in trend may be temporary and only published after the trend was well established.11 The majority of publications on trends in asthma in children are based on data collected prior to 1998 and many are based on a two point comparison. We present here data from consecutive years, and although incidence increased during the 1980s and early 1990s, in 2000 it was similar to that in the late 1980s (fig 1).
The downward trend in the rate of acute asthma episodes in children has been confirmed.11 We have not yet identified any factor which shows a temporal correlation of increase from the 1970s to the mid 1990s and a subsequent decrease. This study stimulates searches for possible aetiological factors and calls for a review of the thinking of the causes of acute asthma episodes.
