Article Text

Abstract
Background Despite the availability of medical abortifacients, and their potential use in primary care, only a small proportion of primary healthcare professionals provide medical abortion services. Understanding the perspectives of primary care providers on delivering medical abortion is pertinent to identifying barriers to medical abortion service provision and increasing access for women globally.
Objective To understand the knowledge, attitudes and practices of primary healthcare providers regarding medical abortion services.
Design Four databases (Medline, EMBASE, Web of Science (WOS) and Scopus) were searched using search terms related to medical abortion and primary care. The Joanna Briggs Institute Critical Appraisal tools were used to appraise the methodological quality of studies included.
Results Some 22 studies were identified, conducted across 15 countries, comprising 6072 participants. Study participants comprised doctors and residents (n=8), nurses and nursing students (n=5), and pharmacists (n=3) and six studies were conducted with mixed samples of providers. Medical abortion was deemed acceptable by some doctors, but fear of criminal prosecution, in countries where abortion is still restrictive, left doctors and nurses circumspect about providing medical abortion. Pharmacists referred women to other providers with only a small proportion dispensing medical abortifacients. General practitioners, nurses and trainees had mixed knowledge of medical abortion and emphasised the need for training on delivery of medical abortion and dissemination of guidelines. Conversely, pharmacists reported poor knowledge regarding medical abortion regimens and complications.
Conclusions Increased dissemination of training and resources is pertinent to supporting primary care providers delivering medical abortion services and to increasing access for women on a global scale.
- abortion
- general practice
- qualitative research
- service delivery
Statistics from Altmetric.com
Key messages
Within the primary care setting, doctors are more supportive of medical abortion service provision than are nurses and pharmacists.
Fear of criminal prosecution and conservative attitudes towards abortion impacted decisions on whether health professionals provided the service.
Most primary care providers have poor knowledge of medical abortion service provision and would benefit from increased training and education.
Introduction
Provision of medical abortion services through the primary care sector has the potential to increase access for women globally. General practitioners (GPs)/family physicians and nurses are ideally positioned to deliver medical abortions because they are the first point of contact for women with contraception and pregnancy-related issues.
Approximately one in four women will choose to terminate a pregnancy in their lifetime.1 Globally, the estimated abortion rate between 2010 and 2014 was 35 per 1000 women aged 15–44 years,2 which was 5 per 1000 women less than estimates in 1990–1994. However, no change in the abortion rate was seen in the developing world. The constant rate of abortions in low- and middle-income countries is largely attributable to poor access to effective contraception.3
One of the most important developments in terms of increasing access to abortion is the practice of medical abortions.4 Medical abortion is a safe and non-invasive alternative to surgical abortion used in the first trimester of pregnancy. The World Health Organization (WHO) recommends a medical abortion regimen comprising mifepristone and misoprostol.5 When this regimen is administered ≤63 days' gestation, the success rate of termination is approximately 98%.6 Additionally, this regimen is approved by the US Food and Drug Administration for use up to 70 days' gestation with a growing body of evidence indicating continued effectiveness in later gestations.7
While GPs, nurses and pharmacists can provide services and medication for women choosing medical abortion, it is still unclear whether medical abortion provision has been successfully integrated into the primary care setting. Understanding the perspectives of primary care providers on medical abortion service delivery is pertinent to identifying barriers and enablers to the successful integration of medical abortion into general practice and is critical to increasing access to these services for women globally.
Limited data show that GPs and pharmacists perceive medical abortion to be out of their scope or practice and that those delivering the service feel stigmatised, under-resourced and unsure about side effects associated with the procedure.8–10 However, to date there has been no systematic review of the literature relating to the knowledge, perceptions and behaviours of primary care providers on medical abortion service delivery.
The aim of this systematic literature review was to identify, assess and synthesise research addressing primary care providers’ knowledge, attitudes and practices (KAP) towards providing medical abortions.
Methods
Search strategy
We searched four databases (Medline, EMBASE, Web of Science (WOS) and Scopus) and manually searched reference lists of included papers. Our search was conducted between March and May 2019 and included all peer-reviewed articles with no restrictions on year of publication. The search strategy used to retrieve articles from Scopus is replicated here: TITLE-ABS-KEY (“induced abortion” OR “medical abort*” OR “mifepristone” OR “misosprostol” OR “methotrexate” OR “unintended pregnanc*”) AND TITLE (“knowledge” OR “perception*” OR “attitude*”) AND TITLE ((“primary care*”) OR (“general pract”) OR (“doctor*”) OR (“physician*”) OR (“pharmac*”) OR (“nurs*”)) AND (LIMIT-TO (LANGUAGE, “English”)).
The systematic search covered three topics: (1) induced abortion, (2) healthcare provider and (3) knowledge, attitudes and practices. For each of the topics, relevant medical subject headings (MeSH), alternate spellings and truncated versions of words were compiled. All search terms were then combined using ‘OR’ to provide a large range of studies for each theme. The three lists of search terms for each of the topics were then combined with ‘AND’ to generate high-sensitivity and low-specificity citations that were relevant to all three elements of the research question. The reference lists of the retrieved articles were screened to identify further relevant papers. Each search was limited to studies in English.
Inclusion criteria
Studies were included in this review if they met the following criteria: all primary qualitative and quantitative research studies in which surveys, in-depth interviews, focus group discussions or self-administered questionnaires were used to investigate the KAP of medical abortion services among primary care providers such as GPs, practice nurses and pharmacists as well as students in these professions. Studies were excluded from analysis if KAP were assessed among medical and pharmacy students, non-primary care health providers, or patients, in relation to medical abortion services, or if outcome measures related to emergency contraception use.
Selection of studies
The first author (AKS) selected and collected the articles for the review. All records identified from the electronic searches were then imported into bibliographic software Covidence for reference management. All duplicates were deleted, and a single copy of each record was retained. Titles and abstracts were reviewed to determine whether studies met the inclusion criteria. Full-text articles were then obtained and analysed according to the inclusion criteria. Each article was independently reviewed by two of the authors (AKS and SD) for inclusion. Differences of opinion were resolved by discussion.
Assessment of the quality of the study and data extraction
To assess the methodological quality of the included studies, we used the Joanna Briggs Institute Critical Appraisal tools11 commonly used for assessing qualitative and quantitative studies for inclusion in reviews. Studies that did not meet the pre-set methodological quality criteria were excluded (online supplementary appendix 1).
Supplemental material
Following the appraisal of the included studies, we extracted the following information: author, year, region and country, aim, study population, and method of data collection.
Synthesis
The results from the included studies were analysed using content analysis that has previously been used for synthesising results in systematic literature reviews of qualitative and quantitative studies.12 The 22 studies included in this review were first assessed to categorise key descriptive themes. The key descriptive themes were then systematised in a matrix, and similarities, differences and contradictions were examined. Analytical themes were developed to answer our question about the KAP of primary care providers towards medical abortions.
Results
Search results and study characteristics
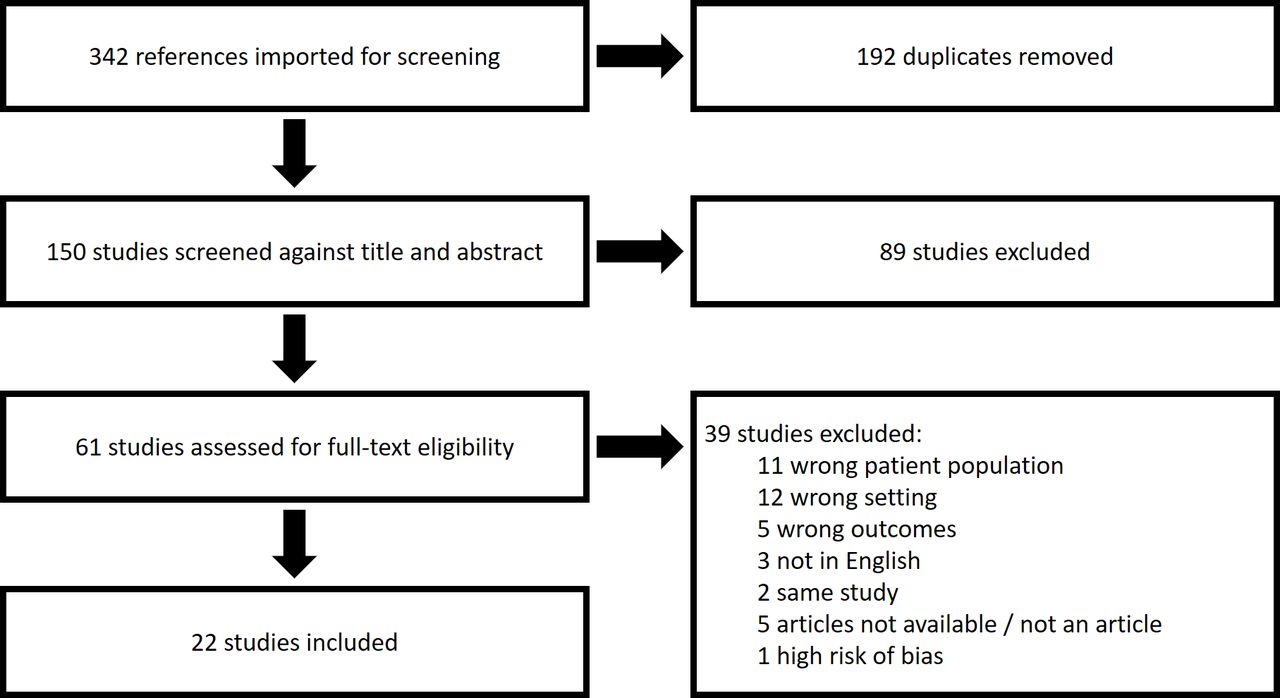
From 342 studies identified, 192 duplicates were removed (figure 1). Titles and abstracts for the remaining 150 studies were reviewed, and then 61 study abstracts were considered for further review. After conducting a risk of bias assessment for articles that met the inclusion criteria, one article was removed due to receiving a high risk of bias score13 (online supplementary appendix 1). Subsequently 22 studies were included in this review. Overall, these 22 studies provided a total of 6072 participants (table 1).

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of search strategy and selection process.
Characteristics of studies included in the review
The 22 studies included in the review were published between 1981 and 2019 and described healthcare professionals’ perceptions of and attitudes towards medical abortions (table 1). The studies were conducted in 15 countries: Italy and France,1 Turkey,2 Northern Ireland,1 Scotland,1 USA,7 Honduras, Mexico, Nicaragua and Puerto Rico,1 Australia,4 Bangladesh,1 Senegal,1 Kenya2 and Vietnam.1
In eight of the studies9 14–20 researchers investigated KAP of medical abortion among doctors and medical interns. Five studies21–25 were conducted on samples of nurses and nursing students, three research groups8 26 27 investigated KAP in pharmacists and six studies28–33 included data from mixed groups of health professionals.
In 12 of the studies14 15 18–25 32 33 researchers used surveys as their method of data collection. Interviews were used in five studies,17 27 28 30 31 and in the remaining five studies8 9 16 24 26 29 multiple methods of data collection were used such as focus group discussions, in-depth interviews, surveys and mystery client visits to pharmacies.
Primary care provider KAP data were further categorised into analytical themes based on content.
Poor knowledge of medical abortion provision
Primary care providers generally were unaware of the efficacy and possible adverse effects related to medical abortion.8 9 14 26 27 Some GPs believed that uterine perforation, cervical laceration and pelvic infection were complications related to medical abortion.14 Internists from California had poorer knowledge about the safety and efficacy of mifepristone compared with family practitioners (59% vs 90%, p<0.004).20 Similarly, nursing students from Italy and Sweden24 and nurses in a Kenyan study demonstrated deficient knowledge in all aspects of induced abortion.21 The majority of pharmacists in Vietnam knew medical abortifacients by trade names rather than generic names8 whereas those practising in Kenya and Senegal had poor knowledge of mifepristone and misoprostol treatment regimens.26 27
Dual influence of legislative restrictions on abortion
Legislative restrictions were perceived to be both a frustration and a necessity, depending on the location of the health professional. The majority of primary healthcare providers believed that medical abortion should be available on request.15 18 21–23 29 33 Some providers considered access to medical abortion as a right for women who requested it regardless of the law.16 22 30 32 In one study, GPs in Queensland, Australia, where abortion was restrictive at the time, were frustrated with legislative restrictions on abortion. They commented that these restrictions not only limited their confidence in providing abortions but also created gaps in their medical training.17However, family physicians in rural Idaho, USA were strongly opposed towards providing RU-486 to their patients due to conservative political and religious views which were shared by the community in which they practised.19 This opposition was also shared by nurse-midwives (n=510) in the USA, 66% of whom said they would leave their place of work if they were allowed to perform abortions.22
Fear and concern
Fear of being labelled an abortion doctor and risk of criminal prosecution were reported to be reasons for not providing medical abortion services by GPs in Australia.16 17 Similarly, doctors in a study conducted in South America, reported to offer mifepristone and methotrexate clandestinely because only surgical abortion was legal.9 These doctors also asserted that they had a fear relating to tele-abortion: the risk of potential misuse and self-medication by women, if mifepristone were to become approved in their countries.9 In another study conducted in Scotland on a small sample of nurses and doctors there was also a shared concern that women may be unable to cope with seeing an expelled embryo if abortion drugs were self-administered.28 Interestingly, from the lens of the provider, internists and family practitioners from California reported concerns about receiving adequate 'back up' access to vacuum aspiration services, lack of access to ultrasound and management of bleeding
Responsibility, scope of practice and demand
There were mixed opinions on who should be responsible for providing medical abortion services. Family planning doctors in Northern Ireland believed gynaecologists should be responsible,15 while some GPs in Australia asserted that dedicated abortion clinics would provide a better service to women than those working in primary care.16 Conversely, in one study conducted in the USA in 1998, with 46 family planning doctors, more than 50% believed that if medical abortion was routinely available that it should be available from primary care physicians.18 Some nurses were comfortable providing medical abortion services if given the opportunity,23 32 but most referred women to other providers, similar to practices among pharmacists in Africa.22 26 27
Despite demand for medical abortion being reported as low in two studies conducted with GPs in Australia,16 17 these GPs still contended that they had concerns about being inundated with requests for medical abortion which would dominate their scope of practice.16
Non-conventional medical abortion models of care
Some alternative medical abortion practices were noted in studies relating to telemedicine and traditional culturally specific methods. In one study conducted in Iowa, USA telemedicine was seen to be acceptable to providers in terms of having a greater reach of physicians and more efficient use of resources compared with standard medical abortion service provision.31 The only challenges cited were documenting the Rhesus status of patients and organising anti-D injections, and amalgamating patient documentation. Conversely, doctors in Honduras, Mexico, Nicaragua and Puerto Rico did not support telemedicine in their countries because they suspected that women would misuse the drugs at home.9 Interestingly these same doctors reported prescribing herbs and teas to induce an abortion or facilitate a complete termination.9
Need for resources
All primary care providers stated that there was a need for more resources and training materials related to medical abortion service provision.9 16 17 33 Lack of training opportunities was cited as the largest barrier to performing medical abortion or assisting another provider in performing medical abortion by nurse practitioners in California.32 Only a small proportion of nurse practitioners and GPs stated they were not interested in receiving medical abortion training because of the concern for needing surgical back-up.33 GP providers in Australia discussed gaps in peer support to ensure continuity of care and professional development and that appropriate policies and procedures need to be developed, particularly on patient follow-up, within practices.16 GPs in South America also reported a lack of information and commented on the poor quality of resources available for them on medical abortion.9 Suggestions for strategic dissemination of information included public information campaigns, creating an informal website for health professionals about medical abortion, and distributing printed materials among doctors.9
Discussion
From our review of 22 studies including 6072 participants, we found that GPs were largely supportive of medical abortion services being available to women, while nurses and pharmacists reported mixed attitudes. Most primary care providers demonstrated relatively poor knowledge of processes and noted that more training and educational materials on medical abortion service provision would be welcomed. Some primary care providers practising in countries where abortion is still restrictive had concerns about providing medical abortion services, due to fear of prosecution and stigma. Despite most primary care providers claiming to support medical abortion, this rarely was reflected in their practice as provision was still poor. Finally, we also demonstrate a gap in the literature for information on medical abortion service provision within the primary care setting, as demonstrated by studies on nurses and pharmacists comprising fewer than 30% of studies included in this review.
Knowledge appeared to be relatively poor across all primary care providers. Some GPs were aware of procedures and follow-up care because they provided the service. Poor knowledge was understandably more common among primary care providers practising in countries where abortion is still restrictive such as Turkey, Kenya, Senegal and some countries in South America. Therefore, national colleges of practitioners around the world should advocate on behalf of the evidence to change legislation so that the best-available evidence around medical abortion provision can be implemented in the form of national guidelines and instruction manuals.
Most doctors supported medical abortion provision, but strong opposition to medical abortion, based on conservative or political views, was still prevalent among some doctors and nurses.19 22 This opposition is problematic when considering the WHO’s recommendation for task-sharing medical abortion models of care whereby doctors and nurses are encouraged to share responsibilities and delegations during provision of medical abortion services to women.34 Therefore, findings from this review support more technical training and values clarification for nurses and midwives to increase provision of safe and high-quality medical abortion care.35
Only a small proportion of primary care health professionals reported providing medical abortion services and dispensing medical abortifacients. Legislative restrictions on abortion, personal objections, and a lack of training and availability of resources were common factors that negatively impacted on service provision. More attention should be given to training and education on personal challenges relating to medical abortion service provision in medical, nursing and pharmacist training. University and college curriculums should comprise clear and comprehensive guidelines on how to manage the ethical dilemmas associated with medical abortion along with training modules on comprehensive medical abortion care, coupled with counselling in family planning and abortion.35
Strengths
To the best of our knowledge, this is the first systematic review to evaluate primary care providers KAP related to medical abortion provision. Studies included in the review spanned several continents, thus providing data on medical abortion service provision in primary care setting within countries with highly disparate legislation on abortion. Additionally, given the strong movement, led by the WHO,5 in support of providing medical abortions at the primary care level, this work is pertinent to understanding how we can improve medical abortion service provision within the primary healthcare sector to fundamentally increase access for women.
Limitations
Studies included in this review comprised various methods of data collection and posed different research questions across studies. Most studies included assessments of knowledge and attitudes relating to medical abortion services without direct assessment of practices. Additionally, adjustment for confounding factors such as age, sex and length of employment were rarely considered.
Conclusions
From this systematic literature review of 22 studies we show that doctors working within the primary care setting are more supportive of medical abortion service provision compared with nurses and pharmacists. Fear of criminal prosecution and conservative attitudes towards abortion determined whether or not health professionals provided the service and or referrals. We also highlight that the majority of primary care providers have poor knowledge of medical abortion service provision and would benefit from quality training and education. Changes in legislation and accessibility to resources are required globally to ensure that primary care providers have the confidence and training to perform abortions safely and become exemplars of abortion advocacy in their respective countries.
Additional Educational Resources
Dawson A, Bateson D, Estoesta J, et al. Towards comprehensive early abortion service delivery in high income countries: insights for improving universal access to abortion in Australia. BMC Health Serv Res 2016;16:612.
Barnard S, Kim C, Park MH, et al. Doctors or mid‐level providers for abortion. Cochrane Database Syst Rev 2015;7:CD011242. DOI: 10.1002/14651858.CD011242.pub2.
World Health Organization. Clinical Practice Handbook for Safe Abortion [Electronic Handbook]. 2014. https://apps.who.int/iris/bitstream/handle/10665/97415/9789241548717_eng.pdf;jsessionid=F68376B09CA2FA832C14B3C8342DC63C?sequence=1.
References
Footnotes
Contributors AKS and DM were responsible for the conception and design of the study. AKS conducted the literature search and extracted the data. AKS and SD independently reviewed articles for inclusion. AKS analysed and interpreted the data and wrote the manuscript. All authors critically reviewed the manuscript and provided important intellectual content.
Funding This study was funded by the National Health and Medical Research Council (NHMRC), Australia (1153592) Centre of Research Excellence in Sexual and Reproductive Health for Women in Primary Care (SPHERE).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.