Effect of early supervised physiotherapy on recovery from acute ankle sprain: randomised controlled trial
BMJ 2016; 355 doi: https://doi.org/10.1136/bmj.i5650 (Published 16 November 2016) Cite this as: BMJ 2016;355:i5650
- Robert J Brison, professor of emergency medicine1 2 3,
- Andrew G Day, senior biostatistician2 3,
- Lucie Pelland, associate professor of rehabilitation therapy4 5,
- William Pickett, professor of public health sciences1 3,
- Ana P Johnson, associate professor of public health sciences3,
- Alice Aiken, professor of rehabilitation therapy4,
- David R Pichora, professor of surgery5 6,
- Brenda Brouwer, professor of rehabilitation therapy4 5
- 1Queen’s University Department of Emergency Medicine, Kingston, ON, Canada
- 2Kingston General Hospital Research Institute, Kingston, ON, Canada
- 3Queen’s University Department of Public Health Sciences, Kingston, ON, Canada
- 4Queen’s University School of Rehabilitation Therapy, Kingston, ON, Canada
- 5The Human Mobility Research Centre, Kingston General Hospital and Queen’s University, Kingston, ON, Canada
- 6Queen’s University Division of Orthopaedics, Kingston, ON, Canada
- Correspondence to: R J Brison, Queen’s University, Clinical Research Centre, Victory 3, Kingston General Hospital, 76 Stuart Street, Kingston, ON, K7L 2V7, Canada brisonr{at}kgh.kari.net
- Accepted 18 October 2016
Abstract
Objective To assess the efficacy of a programme of supervised physiotherapy on the recovery of simple grade 1 and 2 ankle sprains.
Design A randomised controlled trial of 503 participants followed for six months.
Setting Participants were recruited from two tertiary acute care settings in Kingston, ON, Canada.
Participants The broad inclusion criteria were patients aged ≥16 presenting for acute medical assessment and treatment of a simple grade 1 or 2 ankle sprain. Exclusions were patients with multiple injuries, other conditions limiting mobility, and ankle injuries that required immobilisation and those unable to accommodate the time intensive study protocol.
Intervention Participants received either usual care, consisting of written instructions regarding protection, rest, cryotherapy, compression, elevation, and graduated weight bearing activities, or usual care enhanced with a supervised programme of physiotherapy.
Main outcome measures The primary outcome of efficacy was the proportion of participants reporting excellent recovery assessed with the foot and ankle outcome score (FAOS). Excellent recovery was defined as a score ≥450/500 at three months. A difference of at least 15% increase in the absolute proportion of participants with excellent recovery was deemed clinically important. Secondary analyses included the assessment of excellent recovery at one and six months; change from baseline using continuous scores at one, three, and six months; and clinical and biomechanical measures of ankle function, assessed at one, three, and six months.
Results The absolute proportion of patients achieving excellent recovery at three months was not significantly different between the physiotherapy (98/229, 43%) and usual care (79/214, 37%) arms (absolute difference 6%, 95% confidence interval −3% to 15%). The observed trend towards benefit with physiotherapy did not increase in the per protocol analysis and was in the opposite direction by six months. These trends remained similar and were never statistically or clinically important when the FAOS was analysed as a continuous change score.
Conclusions In a general population of patients seeking hospital based acute care for simple ankle sprains, there is no evidence to support a clinically important improvement in outcome with the addition of supervised physiotherapy to usual care, as provided in this protocol.
Trial registration ISRCTN 74033088 (www.isrctn.com/ISRCTN74033088)
Introduction
Ankle sprains are one of the most common and burdensome musculoskeletal injuries and are associated with a high rate of visits to the emergency department.1 2 3 4 5 6 In our own setting of Kingston, Canada, ankle sprains account for 7.5% of injury related visits, about 725 cases annually, which represents an annual rate of presentation to an emergency department of five per 1000 people. Nearly all ankle sprains are simple grade 1 (mechanically stable) or grade 2 (some joint laxity) ligament sprains. Grade 3 sprains (clinical and/or radiological evidence of instability) represent a small minority.7 8 9 Although the prevalence of grade 3 sprains is low, there is good evidence to support the use of immobilisation and, occasionally, surgical correction in the management of these injuries.10 11 12 Yet clinical standards for the acute management of grade 1 and 2 ankle sprains are not well defined.
The absence of high quality evidence to inform effective management of ankle sprains in acute care settings is related largely to perceptions that grade 1 and 2 ankle sprains are relatively benign injuries.13 Short and long term morbidity from simple ankle sprains, however, has been documented among 30-70% of patients, ranging from six months to seven years after injury.10 11 12 14 15 Morbidity is reflected in lost time from school, work, leisure, and sports activities15 16 17; impairment in activities of daily living18; and multiple medical contacts in the time after injury.14
In an effort to reduce the likelihood of short and long term morbidity, several trials have been undertaken in recent years to evaluate the efficacy of supervised programmes of physiotherapy in improving outcomes of ankle sprains and accelerating return to activity.7 19 20 21 22 23 24 A recent systematic review of these trials identified considerable potential for bias related to methods of randomisation, concealment, and outcome measurement and concluded that current evidence for early implementation of supervised exercise is limited in terms of breadth and quality.25 We carried out a randomised clinical trial to address the findings of systematic reviews, including a 2002 Cochrane review, of persisting controversy as to the role of supervised physiotherapy in the management of acute ankle sprains and their call for sufficiently powered trials designed to limit bias.11 25
Methods
We undertook a parallel group randomised controlled trial of adults attending the emergency department with ankle injuries. We evaluated the efficacy of a standardised intervention of supervised physiotherapy plus usual emergency medical care versus usual emergency care alone in augmenting functional recovery from grade 1 or 2 ankle sprains at one, three, and six months. Recovery was assessed with a standardised patient assessed outcome score of ankle function—the foot and ankle outcome score (FAOS),26 as well as clinical and biomechanical measures of ankle function. The primary outcome of efficacy was defined, a priori, as “excellent” recovery (a total score ≥450/500) at three months. We hypothesised that a standardised evidence based programme of supervised physiotherapy20 21 23 27 would improve the near term functional outcomes of ankle sprains. In terms of clinical relevance, high quality evidence regarding the efficacy of physiotherapy would assist acute and primary care physicians in providing recommendations for treatment to patients with ankle sprains.24 28
Participants
Prospective participants were patients presenting for acute medical treatment of an ankle sprain to one of two acute care settings affiliated with Queen’s University in Kingston, Ontario, Canada. The Kingston General Hospital is a 450 bed tertiary care facility providing full emergency department care and the Hotel Dieu Hospital is an ambulatory care hospital with an urgent care setting. Together, these partner facilities manage 95 000-100 000 encounters with acute care patients each year, of which 20% are injury related.
We adopted broad inclusion criteria so that our trial cohort was representative of a general adult population presenting for assessment and treatment of ankle sprains. Eligibility criteria were age ≥16; clinical diagnosis of grade 1 or 2 ankle sprain, which could include clinically unimportant avulsion fractures (<3 mm of displacement),29 with injury sustained less than 72 hours before presentation for assessment; fluency in spoken English; competent to provide informed consent, based on clinical judgment during interview with the patient; willingness to participate in the assessments in the Queen’s University motor performance laboratory as per protocol at baseline and at one, three, and six months after injury; and a total FAOS <450 measured at the baseline visit in the motor performance laboratory. The exclusion criteria were injury mechanisms that were inconsistent with a ligamentous sprain (such as direct impact); the attending emergency physician determining the need for immobilisation of the injured ankle or surgery based on clinical findings; presentation with concomitant injuries; other mobility limiting conditions; inability to accommodate the time intensive study protocol; and a declared plan to seek physiotherapy for treatment outside the study protocol.
Participant involvement
No patients were actively involved in setting the research question or the outcome measures nor were they involved in the analysis, interpretation, and writing of the results. Their involvement in the design and implementation of the study was limited to providing informal feedback during a pilot phase to assess their tolerance and acceptance of data collection methods and procedures. Our findings from the trial will be shared with all participants, who will be provided a lay abstract of our study results and conclusions and access to the full manuscript.
Randomisation and follow-up
Eligible patients identified in the emergency department who were interested in participating in our trial provided consent to have their contact information shared with the research coordinator to schedule a baseline assessment in the motor performance laboratory at Queen’s University. Completion of the baseline assessment in the emergency department was impractical as the FAOS is not scored at the time of injury but rather is an assessment of dysfunction, and patients report limitations related to the injury over the previous week. The target appointment time for baseline assessment in the laboratory was, therefore, one week after injury. All potential participants completed both the baseline assessments of the FAOS and clinical and biomechanical measures before randomisation so that they understood the procedures and time commitment involved. The research coordinator then reviewed entry criteria, confirmed eligibility, and obtained informed consent for the study protocol.
Participants’ personal information and FAOS were entered into a secure password protected web based central randomisation tool linked to a REDCap study database.30 The tool then disclosed the treatment assignment of the current participant to the research coordinator. Participants were randomised to one of two arms of the study: the usual care arm, in which participants received usual care in the emergency department, or the physiotherapy arm, in which participants received usual care plus a regimen of supervised physiotherapy. The randomisation tool used a stratified randomisation list created electronically by the study statistician, who was not involved in recruitment or follow-up. A 1:1 allocation in permuted blocks was used within four strata defined by the baseline FAOS, where the four strata were based on the quartiles obtained from pilot study work. The permuted blocks were of variable random size of at most eight, with the size of the blocks unknown to anyone except the trial statistician. An audit trail was recorded, with concealment guaranteed for all future treatment assignments.
Participants assigned to either arm of the trial were booked for a follow-up assessment of outcome variables in the motor performance laboratory one month after the baseline appointment. Participants randomised to the physiotherapy arm additionally had their contact information provided to the physiotherapy clinic at Queen’s University. The clinic arranged the first appointment within two business days of the baseline laboratory visit to document history and clinical findings relevant to the care of the injured ankle. Participants allocated to the physiotherapy arm were asked not to reveal this allocation to our research staff.
The research associate who performed the registration and randomisation also coordinated follow-up of participants. Research staff blind to group allocation collected both follow-up and outcome data.
Description of the trial arms
Participants assigned to the usual care arm received standard emergency department care, consisting of a medical assessment and a one page written summary of instruction for basic management of the injury at home, including ankle protection, rest, cryotherapy (ice), application of a compression bandage, elevation, use of analgesics as necessary, graduated weight bearing activities, and information about expected recovery. No information regarding physiotherapy was discussed with patients in the usual care arm of the study.
Participants assigned to the physiotherapy arm were provided with usual care (as above) plus a regimen of supervised physiotherapy. This intervention included a first appointment to assess the injury and establish a treatment plan and as many as seven subsequent clinic visits at no financial cost to participants. The physiotherapy intervention followed a standardised plan based on current evidence for the use of functional exercises progressed according to four general stages of recovery of ankle sprains20 21 23 27 31 32 33: decreased pain and swelling; increased range of motion, strength, and weight bearing; active range of motion and increased exercise tolerance; and restoration of full activities and dynamic ankle stability. Specific treatment goals and therapeutic interventions were provided for each stage of recovery, with clearly defined criteria for progression to the subsequent stage, or discharge. Figure 1⇓ summarises the intervention.

Fig 1 Schematic representation of standardised programme of supervised physiotherapy, showing stages of progression, treatment goals for each stage, and criteria for progression or discharge. PRICE=protection, rest, ice, compression, elevation; ROM=range of motion; AROM=active ROM
{kind=link}
Treatment sessions were 30 minutes in length and were augmented by standardised home exercise plans of active ankle range of motion exercises, isometric strengthening, and resistance exercise, using therapeutic elastic resistance bands or body weight. A home exercise programme was recommended based on each patient’s functional recovery. Icing was used when swelling persisted, but no manual therapies or immobilisation (for instance, taping) or brace devices were used. The treatment plan was implemented by one of three assigned physiotherapists, with a single therapist providing all treatment for an individual participant, whenever possible. At each session, the therapist assessed each individual’s stage of recovery and recorded compliance with appointments and home exercise programmes.
Outcome measurements
The FAOS is a self administered questionnaire specific for feet and ankles developed to assess week-to-week change in symptoms and function after foot and ankle injuries.26 The FAOS includes 42 items, assessing five domains of recovery from the ankle and/or foot injury: pain, symptoms, function in activities of daily living, function in sport and recreation, and quality of life.26 34 Each scale is scored from 0 to 100, with a total best possible score of 500.
The primary outcome of efficacy, stated a priori, was “excellent recovery” from the ankle sprain, defined as a total score ≥450/500 at the three month time point of assessment after randomisation.35 36 37
An evidence based FAOS cut off score of excellent recovery has yet to be defined. In our trial, we selected the score of 450/500 based on a previously published study by one of the authors of the FAOS.38 Using the ankle function scoring scale, a precursor to the FAOS, Karlsson and Peterson38 used a scale score of 90% as the criterion for excellent recovery, which translates to a FAOS cut off of 450/500. All FAOS outcome data were collected by trained interviewers using a standard interview script and protocol.
Based on the FAOS, we additionally evaluated a series of secondary outcomes, also defined a priori. These included excellent recovery at one and six months (score ≥450/500) and change from baseline on the total and domain specific FAOS, measured as a continuous variable at one, three, and six months. We included a six month time point of measurement based on previous studies that have shown considerable residual morbidity at six months after injury.39 40
We also obtained selected clinical and biomechanical measures for secondary analysis, providing a quantitative assessment of ankle function and recovery from injury. We assessed oedema, quantified using a figure of eight measurement (mm)41; manual muscle testing of the ankle dorsiflexors and plantar flexors to provide a grade from 0 (no visible contraction) to 5 (full strength through range of motion); and end range of dorsiflexion, assessed using the lunge test.42 We used a Biodex System 3 dynamometer (Biodex Medical Systems, Shirley, NY) to quantify the biomechanical measures43 end range (in degrees) of passive and active dorsiflexion and plantar flexion, with the end point of passive range determined either as the point at which resistance reached 5 Newton metre (Nm) or the point at which the patient terminated the movement; and peak dorsiflexion and plantar flexion torque (Nm), defined as the highest torque produced over five dorsiflexion-plantar flexion cycles at a velocity of 30°/s. We calculated change in clinical and biomechanical measures of ankle recovery from baseline at one, three, and six months.
Any recurrence of injury of the same ankle was monitored at the one, three, and six month follow-up assessments. Additionally, all participants were asked whether they had accessed any other healthcare provider, including physiotherapy services that were not part of the study.
Statistical analysis
Sample size
The study protocol targeted enrolment of 256 participants per arm to achieve a power of at least 80%, at a two sided α of 0.05, to detect an absolute increase in excellent recovery (that is, FAOS ≥450) from 60% to 75%. This sample size estimation includes an inflation factor of 1.63 to allow for intent to treat analysis with a 15% loss to follow-up and 15% treatment cross over. The estimated rate of excellent recovery in the control arm was based on our pilot work. The 15% difference between arms was based on previous literature and the results of our survey of 22 emergency department clinical physicians, most of whom responded that a 15% improvement in excellent recovery would be required to justify routine referral to physiotherapy.
Analysis of primary outcome
Our primary test of efficacy compared the two arms at three months after randomisation using the Mantel-Haenszel test, stratified by baseline total FAOS quarter at a two sided 5% significance level. We calculated the absolute difference in excellent recovery rates between the two arms, adjusted for baseline quarter, with 95% confidence intervals.
Analysis of secondary outcomes
The primary analysis was repeated at one and six months after randomisation. Using continuous FAOS data, we estimated the expected mean changes in total and domain specific score from baseline to one, three, and six months after randomisation by arm, with differences between arms (and 95% confidence intervals) depicted graphically. These estimates were obtained by restricted maximum likelihood from a repeated measures linear model as implemented in the MIXED procedure of SAS.44 This approach used all available assessments including baseline as outcomes, allowing for a flexible (unstructured) covariance structure within individual patients, which is less susceptible to bias from missing data than cross sectional approaches45 and is no less effective than using multiple imputation.45 46 47 Predictors in the model included baseline FAOS quarter as a factor, time as a factor, treatment arm as an indicator variable, and the interaction between time and treatment arm to allow the treatment effect to vary over time. We constructed contrasts to estimate the change from baseline within each arm and the difference in the change between arms at one, three, and six months. We evaluated clinical and biomechanical measures from each time point using the same statistical method. The rate of re-injury of the same ankle was evaluated over the six month follow-up, with differences between arms evaluated by χ2 test.
For all outcomes, we performed intent to treat analysis for our primary assessment of efficacy and a supplementary per protocol analysis. The per protocol analysis excluded contamination from participants who were randomised to the physiotherapy arm and did not attend at least one physiotherapy clinic visit in the first three months of the trial, as well as patients randomised to the usual care arm who independently received physiotherapy during the first three months.
We performed the following subgroup analyses: sex, men versus women; age, comparing outcomes for participants aged ≤30 versus >30; injury characteristic, non-sports versus sports injury; and grade 1 versus grade 2 sprain. To estimate significance of the subgroup treatment effect modification we used a Wald test of the treatment by subgroup interaction term from a logistic regression model with excellent recovery (FAOS ≥450) as the outcome variable and baseline FAOS quarter, treatment arm, subgroup indicator, and the treatment by subgroup interaction term as predictors.
To evaluate effects of missing data, we performed a sensitivity analysis, graphically reporting the difference in the three month recovery rate between the two arms of the study over the entire possible range of missing values. We considered the plausibility of missing values being extreme enough to result in a 15% difference in rate of excellent recovery between the two arms of the study, which we deemed would be large enough to warrant routine referral to physiotherapy.48
All analyses were conducted with SAS (version 9.3, SAS Institute, Cary, NC, 2010).
Results
Between October 2009 and April 2013, we assessed 1969 patients with grade 1 or 2 ankle sprains for eligibility. Of these, 504 patients met our inclusion criteria, provided consent, and were randomised to the physiotherapy (n=254) or the usual care (n=250) arms of our study. One patient in the physiotherapy arm withdrew consent after randomisation and was excluded from the analysis. Figure 2⇓ shows the flow of patients through the study. Table 1⇓ shows relevant patient and injury related characteristics, with no significant differences identified between the two study arms.

Fig 2 Patient flow showing loss to follow-up, withdrawal, and missing data by study arm and outcome assessment period. Counts below randomisation are accumulative, with numbers in each box adding up to total number of patients allocated to given arm. Withdrawn=patients who actively refused to participate in further treatment or follow-up; lost to follow-up=patients who could not be contacted for current month assessment; missing FAOS=patients for whom FAOS at specified time point was not obtained
{kind=link}
Relevant characteristics of study cohort of patients with acute ankle sprain randomised to usual care with physiotherapy or usual care alone. Figures are numbers (percentage) of patients unless specified otherwise
Given the actual observed sample size and the rates of contamination and loss to follow-up, the power to detect a 15% improvement in our primary outcome was 78% for the intent to treat analyses and 82% for our per protocol analyses.
Table 2⇓ (intent to treat) and table 3⇓ (per protocol analysis) show comparisons of the study arms for the primary outcome, FAOS ≥450 at three months, and the secondary outcomes of excellent FAOS at one and six months. The per protocol analysis excluded 69 participants in the physiotherapy arm who did not attend at least one protocol physiotherapy session in the first three months, as well as 26 participants in the control arm who received physiotherapy during the first three months. Neither analysis identified strong, consistent, or significant differences in primary or secondary FAOS outcomes by study arm.
Results of intent to treat analysis for primary outcome of excellent recovery (total FAOS ≥450) in patients with acute ankle sprain randomised to usual care with physiotherapy or usual care alone
Results of per protocol* analysis for primary outcome of excellent recovery (total FAOS ≥450) in patients with acute ankle sprain randomised to usual care with physiotherapy or usual care alone
Figure 3⇓ (intent to treat analysis) and figure 4⇓ (per protocol analyses) show the change from baseline in total and domain specific continuous FAOS. Differences between groups in the mean change were not significant at any follow-up time point for any FAOS domain. Tables 4 and 5⇓ show the results of the subgroup analysis. Although these indicate a benefit for physiotherapy at three months in the subgroup of patients aged <30, with a borderline significant (P=0.05) interaction between treatment and age at the three month assessment, this trend was not present at other time points and would not remain significant after any reasonable adjustment for multiple testing. There was no significant treatment difference in any other subgroup. Figure 5⇓ characterises the missing data sensitivity analysis for the primary outcome of three month recovery (total FAOS ≥450). To reach a clinically important difference of 15% favouring the physiotherapy arm, we would have needed either of the following two conditions to be satisfied: at least 20/25 participants with a missing intervention in the physiotherapy arm to have excellent recovery and none of the 36 in the usual care arm achieving excellent recovery; or all 25 participants with a missing intervention in the physiotherapy arm and no more than five in the control arm achieving an excellent recovery. Based on the low rate of excellent recovery identified among the 88% of randomised participants with three month follow-up (tables 2 and 3⇓), these conditions are exceedingly unlikely to be achieved.

Fig 3 Intent to treat analysis of change in FAOS from baseline. Estimates are based on restricted maximum likelihood using all available FAOS scores from all patients
{kind=link}

Fig 4 Per protocol analyses of change in FAOS from baseline. Estimates are based on restricted maximum likelihood using all available FAOS scores from all patients
{kind=link}
Subgroup analyses by sex and age for intent to treat analysis of primary outcome of excellent recovery (total FAOS ≥450) in patients with acute ankle sprain randomised to usual care with physiotherapy or usual care alone
Subgroup analyses by injury characteristics for intent to treat analysis of primary outcome of excellent recovery (total FAOS ≥450) in patients with acute ankle sprain randomised to usual care with physiotherapy or usual care alone

Fig 5 Sensitivity analysis for missing FAOS data to assess “excellent” recovery at three months, plotting predicted proportion of recovery among 25 unknown participants in physiotherapy arm to predicted proportion among 36 unknown participants in control arm. Main axes (bottom and left) show percentages and secondary axes (top and right) show counts
{kind=link}
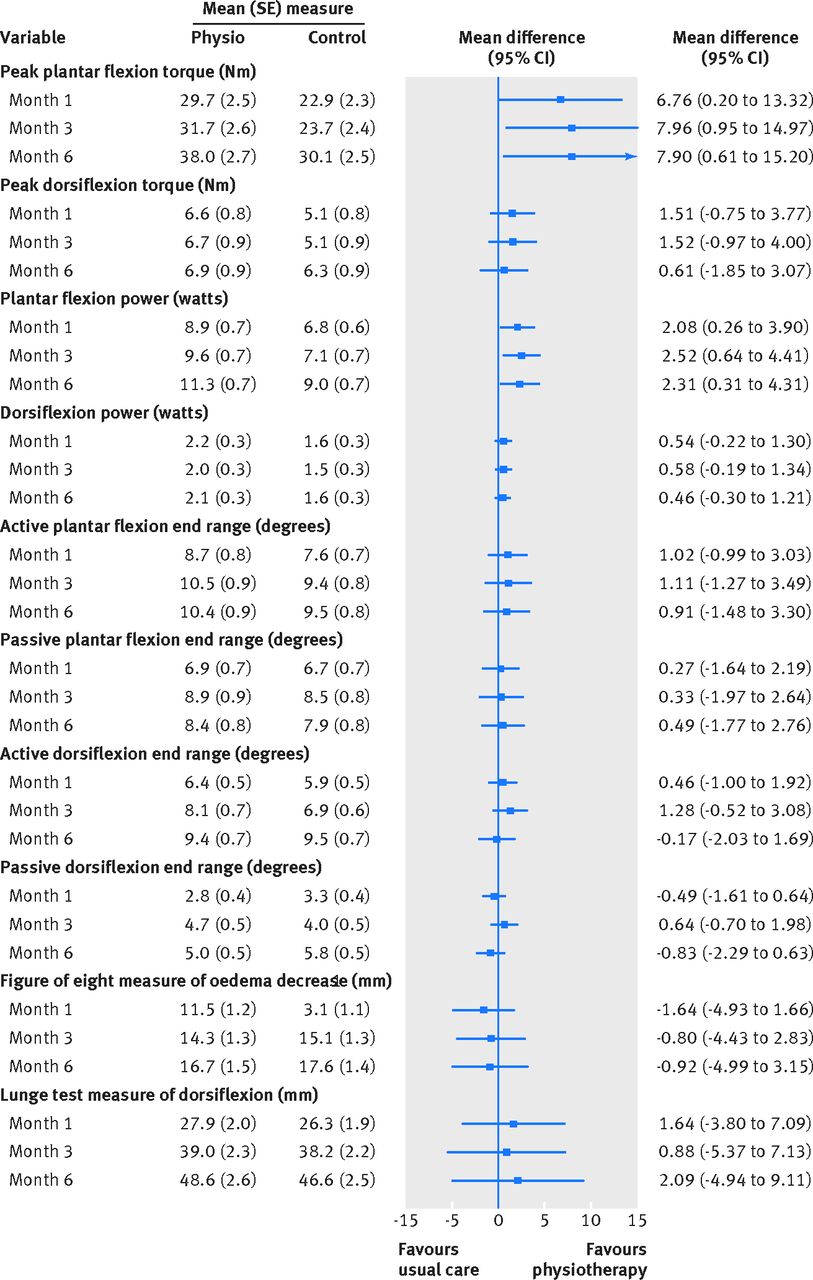
Figure 6⇓ (intent to treat analysis) and figure 7⇓ (per protocol analyses) show the assessment of change from baseline in clinical and biomechanical measures at the three time points. In the intent to treat analysis, there were no significant differences among the 10 variables measured. In the per protocol analysis, measures of peak plantar flexor torque (Nm) and plantar flexor power (watts) favoured the physiotherapy arm, with no other clinically important or significant differences identified by treatment arm.

Fig 6 Intent to treat analysis of change in clinical and biomechanical measures from baseline. All estimates reported as increase from baseline, with exception of figure of eight measure of oedema, which is reported as decrease from baseline, so that greater increase is consistently favourable. Estimates based on restricted maximum likelihood using all available measures from all randomised participants
{kind=link}

Fig 7 Per protocol analyses of change in clinical and biomechanical measures from baseline. All estimates reported as increase from baseline, with exception of figure of eight measure of oedema, which is reported as decrease from baseline, so that greater increase is consistently favourable. Estimates based on restricted maximum likelihood using all available measures from all randomised participants
{kind=link}
In the six month follow-up period, 19/254 (7.5%) participants in the physiotherapy arm and 21/250 (8.4%) in the usual care arm reported a re-injury of the same ankle, with no significant difference between the two trial arms (P=0.71).
Discussion
Principal findings
With the participation of 503 patients, our trial is the largest randomised controlled trial to have evaluated the therapeutic benefits of supervised physiotherapy in the treatment of acute ankle sprains. Based on our outcomes, we conclude that among patients aged 16-79 presenting to an emergency department with a simple grade 1 or 2 ankle sprain within 72 hours of their injury, the addition of early supervised physiotherapy to usual care does not lead to clinically important improvements in functional recovery up to six months after injury, compared with usual care alone. The absence of a therapeutic benefit of supervised exercise was confirmed for our primary outcome of excellent functional recovery as assessed by the FAOS at three months, as well as for the FAOS (using both excellent recovery and continuous scores) and objective clinical and biomechanical measures at one, three, and six months after injury. Our finding is clinically important as the recommendation of physiotherapy for the management of acute ankle sprains comes with substantial economic costs.
Strengths of the trial
Our trial conformed to the CONSORT guidelines.49 Our main findings are unlikely to be explained by imbalances in confounding factors, both known and unknown, between the trial arms. Baseline group comparisons essentially showed equivalence on such factors, suggesting that the approach to randomisation and its administration were effective. Although participants were volunteers, the study population was large and heterogeneous, and, because of the use and effectiveness of randomisation, it is unlikely that any forces of selection resulted in bias in the observed effect estimates. A participation rate of 88% at the three month primary endpoint and 80% at six months was maintained. Subgroup analyses suggested a benefit of physiotherapy at three months in younger patients (aged <30). The direction of effect was not consistent, however, and favoured the usual care group at one and six months. There were no significant differences between study arms in subgroup analyses by sex, cause of injury (such as sports related or not), and grade of injury (grade 1 or 2) at one, three, and six months after injury.
We also conducted a sensitivity analysis, as recommended by Thabane and colleagues,50 to verify the robustness of our findings. Consideration of missing data from loss to follow-up, by re-estimating the treatment effect of the primary outcome over the entire possible range of missing values, did not change our findings. We identified contamination, from non-compliance with the trial protocol in terms of not receiving assigned (27.3%) physiotherapy or by independently seeking physiotherapy when not assigned (10.4%) and conducted separate intent to treat and per protocol analyses. Both analyses failed to show clinically important effects associated with the physiotherapy intervention, and the observed trends reversed from three months to six months.
Another potential source of bias is the effect of “social desirability,” where patients assigned to an active intervention are more prone to self report favourable outcomes during clinical interviews.51 Such bias would be expected to favour the physiotherapy intervention. There were, however, no clinically important differences or consistent trends in outcomes over time for both the self reported FAOS and the clinical and biomechanical measures of ankle function. Blinding was implemented when possible among the attending therapists, laboratory personnel, and interviewers.
The FAOS is one outcome measurement available to determine patient assessed foot and ankle function.24 We do recognise that although the FAOS has been refined and validated in various contexts,31 52 53 the nature and extent of non-differential misclassification of the primary study outcome remains unknown. Therefore, any misclassification of outcomes in our trial is most likely to be non-differential in nature. Also, our criterion of a score ≥450 denoting excellent recovery was based on studies that used similar self report questionnaires for lower extremities—namely, the lower extremity function score (LEFS)54 and the knee injury and osteoarthritis outcome score (KOOS).48 The evaluation of the FAOS as a continuous variable, as we did in our secondary analyses, allows for a more statistically efficient analysis of this outcome. The use of a cut off to dichotomise recovery as “excellent” or “not excellent,” however, provides a more clinically interpretable outcome.55 It is likely that patient assessed measures of excellent recovery will be influenced by the characteristics of the clinical population under study,25 and, therefore, a range of cut offs might be appropriate. Identification of those characteristics that modify patients’ assessment of recovery requires further research, though the stringent criterion adopted in our study provides confidence that patients classified as recovered were appropriately categorised as recovered.13 56 57
Comparison with other studies
Our results contradict those of Hultman and colleagues,24 who conducted a randomised controlled trial to evaluate the effectiveness of providing four physiotherapy visits in addition to usual emergency department care on recovery of ankle function measured at six weeks and at three months after injury. The physiotherapy visits were held within 14 days of attendance. As in our study, the physiotherapy regimen was standardised and based on functional exercises, using the FAOS as the primary outcome. Hultman and colleagues reported a therapeutic benefit of physiotherapy in addition to information provided in the department. Their trial was relatively small, with 33 patients in the intervention group and 32 in the control group. Their protocol instructed patients to exercise to a pain level of 5 out of 10 on a visual analogue scale, according to Thomée’s model57 of pain control, whereas our patients were instructed to exercise as tolerated. The role of training to a higher level of pain, and the reinforcement of this during physiotherapy, could warrant further evaluation.
Limitations of the trial
The limitations of our trial need to be acknowledged in the interpretation and application of our findings to practice. Our extensive protocol might have introduced bias in the characteristics of participants in our study group. While we were successful in enrolling 504 patients, this represents a recruitment rate of one in three patients who met our clinical criteria of eligibility. We suspect that our time intensive appointments for outcome assessment might have contributed to the refusal of 232 eligible patients to participate. Another 129 eligible patients declined to participate because of travel distance, a consequence of our urgent care centres serving a large geographical region. As such, our sample might not be generalisable to all those who experience grade 1 and 2 ankle injuries. Our high retention at the three month primary end point (88%) and at six months (80%) supports a high level of commitment among our study participants.
Conclusions and implications for practice
Our trial provides level I evidence that supervised physiotherapy, as described, does not provide clinically important benefit in the management of simple ankle sprains in a general population of patients seeking care in an acute care setting. Our comparator of usual care was the provision of written recommendations for initial rest, cryotherapy, compression, and limb elevation, with graduated mobility being encouraged as tolerated. These recommendations stem from basic principles of physiotherapy, which, to our knowledge, are commonly provided in emergency departments. This format of usual care is associated with minimal cost and is unlikely to ever be assessed against no care. We do note that 43% of participants in the physiotherapy arm and 38% in the control arm had not reached excellent recovery by six months; this being lower than anticipated. This suggests that while there was not a clinically important effect with the standardised physiotherapy regimen provided to our participants, there is potential for the investigation of alternative interventions that would reduce morbidity in patients with these injuries.
What is already known on this topic
-
Ankle sprains are one of the most common and burdensome musculoskeletal injuries and are associated with a high rate of visits to an emergency department
-
Although most ankle sprains are simple grade 1 or grade 2 ligament sprains, the clinical standards for the acute management of these injuries are not well defined
-
Current evidence regarding the role of supervised physiotherapy in the acute management of these injuries is limited
What this study adds
-
In the acute management of patients with grade 1 and 2 ankle sprains presenting to an emergency department within 72 hours of injury, a standard intervention of early supervised physiotherapy plus usual care does not lead to clinically important improvements in functional recovery up to six months after injury compared with usual care alone
-
As 43% of participants in the physiotherapy arm and 38% in the control arm did not reach excellent recovery by six months, there is potential for the investigation of alternative interventions that would reduce morbidity associated with these injuries
Footnotes
-
We thank D Emerton, who coordinated data collection, X Sun, who assisted with data analysis, S Dostaler, who assisted with trial development and registration, and I Bielska for maintaining literature reviews. We also thank all participants for their time and commitment to our study and participants involved in the pilot phase of our trial, who provided feedback on our methods and procedures.
-
Contributors: RJB and AGD were responsible for data integrity and analyses for the study. All authors contributed to the study concept and design. RJB and BB were responsible for data acquisition. AGD, RJB, BB, and WP were responsible for the statistical analysis and interpretation. RJB, AGD, LP, BB, and WP drafted the manuscript. All authors contributed to the critical revision of the manuscript for intellectual content. Study supervision was provided by RJB and BB. RJB is guarantor.
-
Funding: The study was funded by the Canadian Institutes of Health Research (MCT-94833). The sponsors had no role in the design, conduct, and analysis or involvement in the preparation or submission of the manuscript for publication
-
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
-
Ethical approval: This study was approved by Queen’s University Health Sciences Research Ethics Board (file No 6004187) and informed consent was given by all patients.
-
Data sharing: The investigators will share data (with associated coding library) used in developing the results presented in this manuscript on request (from AGD, daya@kgh.kari.net). Anonymised record level data would be made available on request to investigators who have submitted a publicly available proposal for analysis and who have received ethical clearance from their host institution.
-
Transparency: The lead author affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/.