Article Text

Abstract
Background: Since 2000, out-of-hours primary medical care services in the UK have undergone major changes in the organisation and delivery of services in response to recommendations by the Carson Review and more recently, through the new General Medical Services Contract (GMS2). People calling their general practice in the evening or at weekends are redirected to the out-of-hours service which may offer telephone advice, a home visit or a visit to a treatment centre. Little is known about users’ experiences under the new arrangements.
Aim: To explore users’ experiences of out-of-hours primary medical care.
Design of study: A qualitative study employing focus groups and telephone interviews.
Setting: Three out-of-hours primary medical care service providers in England.
Methods: Focus groups and telephone interviews were conducted with 27 recent users of out-of-hours services.
Results: Key areas of concern included the urgency with which cases are handled, and delays when waiting for a call back or home visit. Users felt that providers were reluctant to do home visits. The service was regarded as under-resourced and frequently misused. Many expressed anxiety about calling, feeling unsure about how appropriate their call was and many were uncertain about how the service operated.
Conclusions: Service users need clear information on how current out-of-hours services operate and how it should be used. Problems with triaging need to be addressed, users should be kept informed of any delays, and care needs to be taken to ensure that the new arrangements do not alienate older people or individuals with complex health needs.
Statistics from Altmetric.com
In the UK the delivery of out-of-hours primary medical care services has altered substantially over the past 20 years.12 In the early 1990s the predominant service model was that of general practitioner cooperatives, which were gradually replacing deputising services; only a few doctors provided on-call cover exclusively to patients on their lists. Cooperatives are composed of general practitioners from neighbouring practices who joined together to share the responsibility for being on-call, providing coverage for the locality through a rota system. Although this generic model was widespread, there was considerable variation in both the size and staffing offered by different cooperatives, and in the processes by which patients’ calls were taken, triage conducted and the management options available.2
By the end of the 1990s, out-of-hours primary care services in the UK had reached crisis point, in part due to ever increasing patient demand, combined with increasing general practitioners’ concerns about workload and the effect of providing out-of-hours care on their home life.13 A government review was commissioned,4 which delivered a critical verdict on the quality, safety and effectiveness of out-of-hours care. This review called for innovative ways in which to improve patient access to services through better integration of out-of-hours services based within primary care with other emergency services (for example, NHS Direct telephone service), and the implementation of care quality standards to monitor the performance of providers.5 From the general practice perspective, the tensions regarding delivering out-of-hours care culminated in contractual changes in the operation of primary care services. By October 2004, the new General Medical Services contract (GMS2)6 was implemented with far-reaching consequences. For the first time since the inception of the National Health Service (NHS), general practitioners were able to opt-out of the responsibility for commissioning and providing out-of-hours care, with this responsibility passing to the primary care trusts (PCTs); unsurprisingly, the vast majority of general practitioners opted out.
In many areas the existing general practitioner cooperatives were commissioned and the extent to which the services altered as a result of the GMS2 contract is debatable. Notwithstanding this, the new quality standards incentivised the merger of small neighbouring cooperatives due to economies of scale around implementing performance monitoring and clinical governance. Thus although the model was essentially still based on the “not-for-profit”, cooperative model the geographical area covered may have increased substantially. Similarly out-of-hours services were given the flexibility to employ other health professionals (eg, nurse specialists) to complement the clinical care provided by general practitioners, resulting in a more diverse workforce.2 Reviews of comparability of UK and international models of out-of-hours primary care have recently been published,12 with evidence of parallels with UK service models emerging in Denmark and the Netherlands.
People calling their general practice in the evenings or at weekends are redirected to the out-of-hours primary medical service which may manage the call by offering telephone advice, a home visit, or a visit to a treatment centre, with medical care provided by a variety of health professionals. Telephone advice and visits to treatment centres are increasingly offered to patients instead of the traditional home visits. Some patients have reported difficulty getting to treatment centres,78 but many appreciate the opportunity of having a prompt face-to-face consultation out of hours.8 However, telephone consultations have been consistently associated with decreased satisfaction compared with home visiting9–12 with some service users expressing doubts about whether an accurate diagnosis is possible over the phone.713 Prior expectations are important, however, and can predict overall satisfaction with out-of-hours care independent of the service type or location of care14–16—for example, people who originally expected a home visit are more likely to be dissatisfied if given telephone advice.31013
As approximately 13% of the English population uses out-of-hours services each year,2 with users a substantive proportion from the more vulnerable members of society (eg, children younger than 5 years, older people or individuals with complex healthcare needs),317 it is important to understand users’ experiences of out-of-hours service provision. A recent report by the National Audit Office on the provision of out-of-hours services in England2 stated although providers are beginning to deliver a satisfactory standard of care, not all are meeting national quality requirements5 (particularly regarding speed of response). This report also concluded that although most patients have broadly good experiences of out-of-hours care, an estimated 1 in 5 have negative experiences, which may not be captured by PCTs, in part due to the use of unstandardised patient satisfaction questionnaires. It is critical to explore such experiences now, because of the extensive reorganisation of out-of-hours primary medical care services. This was the aim of the current qualitative study. The work formed the first phase of a larger study which aimed to develop an instrument suitable for the routine monitoring of patients’ experiences of out-of-hours primary medical care services5 and address the shortcomings of patient satisfaction tools currently used by providers.2
METHODS
Settings
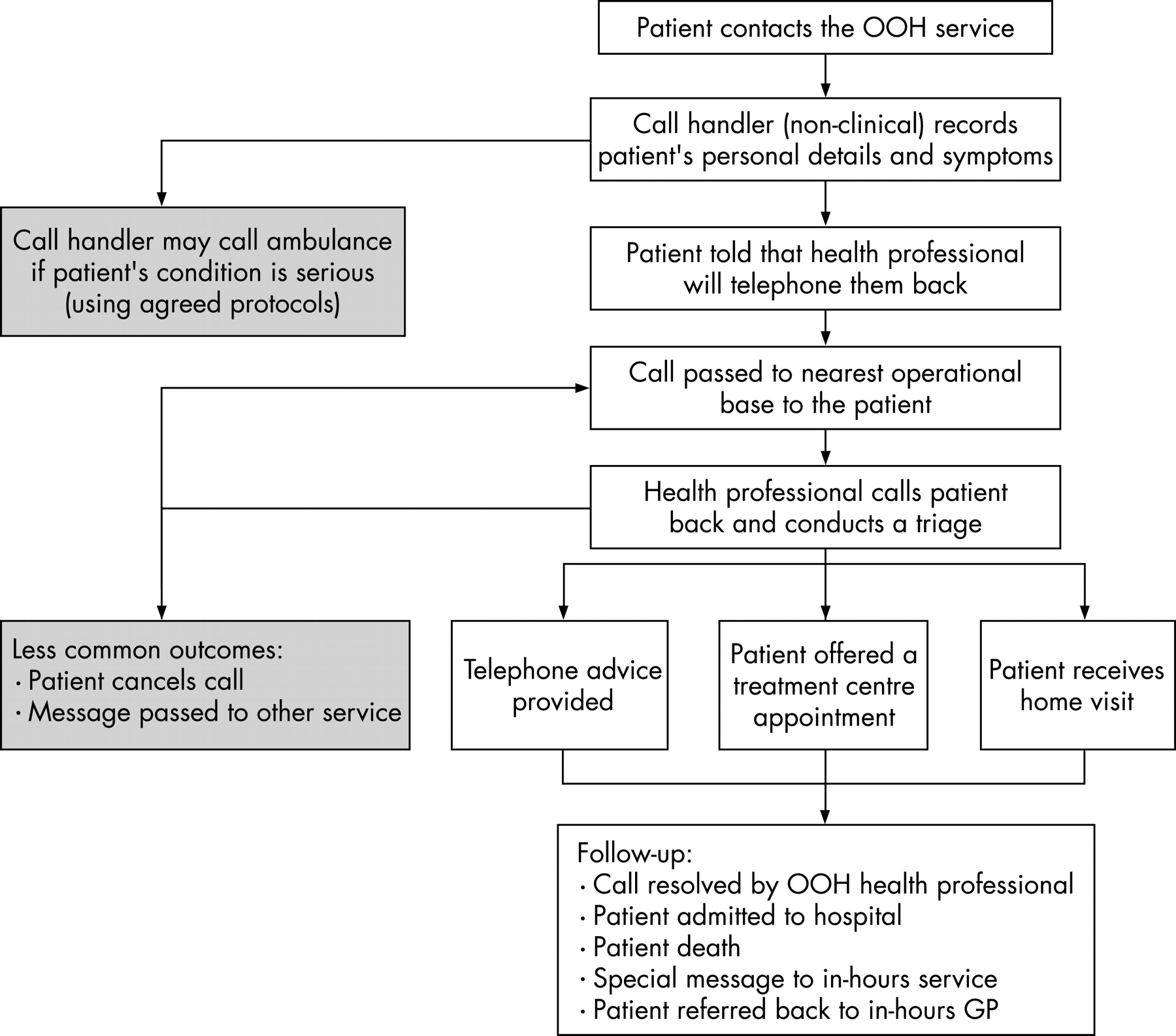
Three out-of-hours primary care services from different regions in England participated in this study. Two of the services (areas 1 and 3) provide care for an area equivalent to three PCTs (about 300 000 residents/area) whereas the third (area 2) covered eight PCTs (about 900 000 people). Areas 1 and 2 were mutual (not-for profit) organisations formed out of an amalgamation of existing general practice cooperatives which mapped onto each PCT area, whereas area 3 commissioned a private sector healthcare provider. All three services adopted a hub-and-spoke model. Administrative functions have been centralised (hub), whereas clinical services operate from existing local bases (spokes). The key feature of the model (fig 1) is the logging of patient details by a non-clinical call handler based in a centralised office who advises the patient that they will receive a telephone call shortly. The call handler then passes the details to a regional treatment centre for triage (at least one centre/PCT). All patients are telephoned back by a health professional, usually a general practitioner (much less often a nurse practitioner or paramedic) who then conducts a clinical triage. Based on the findings of the triage, a range of management options can be accessed, which in turn can result in a range of follow-up requirements.
{kind=link}
Box 1: Sample exclusions
Age 12–16 inclusive
Person too unwell to participate (eg, end-stage terminal illness, recent hospital admission, nursing home resident)
Contact details omitted (eg, address given as a hospital ward or holiday park)
Contact was message handling (eg, details passed directly to another service)
Person flagged on system as aggressive or violent and requiring special procedures
Sampling
We invited 415 users of out-of-hours primary care services in three regions to attend focus group discussions about their experiences. To maximise sample heterogeneity the selected areas varied in terms of affluence, deprivation and ethnic diversity. Areas 1 and 2 in the south were a mixture of urban and rural populations and area 3 in the north was predominantly urban and ethnically diverse. In each area we sampled from a list of contacts to the out-of-hours service in the previous two weeks. Our sampling strategy aimed to include approximately equal numbers of (1) service users from each area; (2) parents of children aged 11 or younger and people in the age groups 17–49 and 50 plus and (3) individuals receiving different management options (telephone advice, treatment centre or home visit). Box 1 shows the exclusion criteria.
Box 2: Focus group topic guide
About the out-of-hours service and their contact with it
What did you know about the service before you contacted it?
How many times have you used the service before?
What did you want/hope for from the service (did you want a home visit or just telephone advice?)? How did this compare with what was offered?
How do different management options (ie, referred to treatment centre, received telephone advice or home visit) compare with each other?
Discuss ease of access to care
How easy was it to understand the information provided by your general practice about how to contact the out-of-hours service?
What types of information were you asked to provide by the person you initially spoke to on the phone and did you understand why it was needed?
What was the outcome of the assessment (eg, told immediately, had to wait for outcome)?
For those told to visit a treatment centre/emergency unit
How easy was it to get to/find the unit, what mode of transport did you use, and how long did it take?
How long did you wait to be seen at the treatment centre?
What did you think about the treatment centre (in terms of comfort and cleanliness)?
For those who received a home visit
How did you feel about being visited at home?
How long did you wait for the visit?
For those who received telephone advice
How did you feel about being given advice over the telephone as opposed to seeing a health professional in person?
How long did this person spend with you on the telephone?
Discuss the health professional who mainly dealt with their problem.
What kind of manner did the person who mainly dealt with your case have?
Did they seem concerned, dismissive, friendly, polite, abrupt, patient, considerate?
How well did they listen to you and take into consideration your personal situation in deciding treatment or advising you? How well did they explain things to you?
Do you have any comments about how the health professional who dealt with your problem could improve?
Discuss what happened after their consultation
How easy was it to get any necessary medicines?
Did the prescribed treatment make you feel better?
How easy was it to follow any instructions you were given about what to do if the patient’s condition became worse?
General rounding up topics
Do they have any comments about how the service could be improved?
What haven’t I asked that I need to have asked to be sure I got all the relevant information about your views on the out-of-hours service?
We anticipated a low uptake rate in each area as focus groups can be time consuming and/or inconvenient for some participants. Eligible individuals were sent an invitation and information sheet via the out-of-hours provider, with a reply slip to return to the research team indicating whether they would like to participate. The focus groups were offered at various times throughout the day as well as evenings, and located in local general practices and/or PCT offices. Out-of-pocket expenses were paid to individuals who attended the focus group. Telephone interviews were conducted with five people who indicated that they would like to participate but could not attend the focus groups. From this availability sample, individuals were selected as they had indicated a willingness to provide feedback on the service, and their socio-demographic characteristics matched our sampling groups.
Data collection
Six focus groups were conducted in total; three in area 1 (three participants in each group), two in area 2 (four participants in one group, three in the other) and one in area 3 (six participants). The focus groups were run by an experienced qualitative researcher (PP) and an assistant. They lasted 50–80 min and were audiotaped and transcribed verbatim, as were the telephone interviews, also conducted by PP. Box 2 summarises the topic guide used in the interview.
Data analysis
The focus group and telephone interview transcripts were coded and analysed by PP. Since the study was both exploratory in terms of users’ experiences and aimed to generate domains for a patient focused satisfaction questionnaire, a basic thematic analysis was undertaken.18 This involved coding the first transcript and then systematically testing, expanding and modifying the coding frame iteratively with subsequent transcripts. Once all the data were coded, the transcripts were re-read to ensure that the coding system was adequate and able to accommodate all the data. The coding frame was then refined by eliminating redundant codes. Independent coding by a second researcher (SR) confirmed that the coding frame was meaningful and comprehensive. Finally, codes were grouped into a small number of categories corresponding to overarching themes and the data systematically compared across the three geographical areas. Illustrative quotes were selected to exemplify key themes.
RESULTS
Sample
Out of 415 people contacted, 160 (38.5%) returned a reply slip. Of these 160 responders 27 people contributed data; 22 in focus groups and five in telephone interviews. The 115/138 who declined to participate in a focus group gave a reason for doing so (five of whom later participated in a telephone interview, table 1).
The characteristics of the focus group participants are summarised in table 2. Consistent with our sampling strategy we recruited approximately equal numbers of participants from the different geographical areas, age groups and final management options, although individuals from ethnic backgrounds other than Caucasian were under-represented. The age range was 31–80 years (average 55) with six being parents of children aged 11 or under. Between them, the sample had 41 contacts (13 home visits, 13 telephone advice and 15 treatment centre). Over a third of participants or their relatives worked, or had worked, in a health-related field. Telephone interviews targeted middle-aged service users (from areas 1, 2, 3) and a parent of a young child (area 1) as these groups had been under-represented in the focus group samples.
Focus group findings
The focus group findings related to eight key themes dealing with issues of both the quality and safety of accessing out-of-hours care:
deciding to call the service;
getting through to the service;
prioritising calls;
waiting;
location of consultation;
quality of clinical care;
access to medical history;
collecting medicines.
Deciding to call the service
This theme highlighted the feelings and worries people experienced prior to calling the out-of-hours service. The decision to make a call to the service was not always easy. In general people described waiting as long as possible before calling the service and only calling when symptoms deteriorated. The description below is typical:
“so when I wasn’t feeling very well on the Saturday I thought oh I’ll wait until Monday for my doctor, but then it came to Sunday I was getting worse and then the day I went, I phoned, was Bank Holiday and you’re thinking to yourself, I mean I felt lousy, and I’m thinking what do I do? Do I make a—it might be nothing so do I—what shall I do? Shall I try and wait until tomorrow, try and get a doctor’s appointment? But then it was getting worse and I, I had, I know it sounds daft if anyone does it, meningitis came into my mind.” (2, area 1)
As the above quote suggests, some people were unsure whether or not their condition was serious enough to merit the contact, or whether the service was only for seriously ill people. Many felt that there would always be someone who needed the doctor more than they did. People from all groups said they worried about calling the service, with more than half expressing some guilt about calling. There was also a fear of wasting the doctor’s time or “abusing the system”. A few people identified a possible generational difference around expectations for out-of-hours care. As one man put it:
“We are all of an age to remember the doctor as a revered figure in society that you didn’t bother unless it was really important. I think that’s at the back of all this. It’s the feeling that we’re not actually, we haven’t been consumers of the service for long enough. I’m sure young people would not be saying this, you know, if you’d got any teenagers here they would think it was their right to have a doctor visit.” (206p, area 3)
Concern was expressed among all groups that some people misused the service for minor complaints, but participants emphasised that their reasons for calling were serious and that they did not misuse the service in this way.
Getting through to the service
None of the groups reported any problems with getting through to the service. However, although the system was similar in all three areas (in so much as the first patient contact was with a non-clinical call handler required to take basic descriptive data following agreed protocols), some of the area 3 group expressed particular frustration at having to answer a routine set of questions first, despite saying how serious their condition was. One man rang on behalf of his wife who had postoperative wound dehiscence:
“Right, and my experience was getting someone on the end of it, no doubt flow chart driven, computer screen full of questions. And the first thing I said was, ‘My wife has just been discharged from hospital and her stomach is slit from top to bottom and she has an infection.’ Now what I would have expected is a modicum of clinical judgment being used, and at least skipping some of the process. Not a chance.” (206p, area 3)
The area 3 group felt that in such cases these questions should be omitted and the caller passed to someone with medical training immediately. Alternatively, as one man said, the call handler should obtain the details of the illness first:
“I’m talking about getting to the nitty gritty before you start worrying about whether she’s over forty or under fifty, or Catholic or Jewish or whatever. Get to the nitty gritty first and then ask the questions after.” (204, area 3)
In relation to this, two people in area 3 felt that call handlers should manage calls in a more personal way.
Prioritising calls
The question of how calls were prioritised was an important theme for all the groups. Most people were unsure how the service worked and what happened following the initial contact. Some wondered whether calls were simply responded to on a “first come, first served” basis. Several people, particularly those in area 1, strongly felt that their cases had not been dealt with sufficiently urgently. One man described his frustrations:
“I phoned on my mobile and said, ‘I think I should take him straight to (hospital) because I know the symptoms.’ I have lived with it long enough, for a very long time in fact, I knew all about asthma, and they didn’t phone me back until well after I got back home, by this time it was too late, he should have been in (hospital), he would have been recovering. Eventually they sent a doctor out, two hours later to the house and then he said to me, ‘Why didn’t you just take him straight to hospital’ and I said ‘I tried to tell your people that!’” (9, Area 1)
Another man felt that when there were delays in accessing care it was because the onus was on the patient to convey the urgency of the situation:
“I can appreciate when there are people that are not articulate [they] have difficulty explaining what their real medical condition is. The person at the other end doesn’t necessarily get the true feel of what’s going on and how urgent the call is. Erm, that’s what concerns me. Erm, that if it’s somebody who really has got a problem and doesn’t realise how serious that condition is, the information they give them isn’t good enough, erm, and it then takes an hour and a half when an ambulance ought to have been there.” (8, area 1)
Most of the people who felt their cases had not been dealt with sufficiently urgently questioned the skills and training of the call handlers. This was particularly true in areas 1 and 3:
“I’d like to know what clinic knowledge that receptionist or whoever it is has and what they do with what you tell them. I mean, you know, like you say, you give them the symptoms and this that and the other but do they then prioritise you? And if they do prioritise you as to how quickly the doctors would have phoned back, what knowledge are they basing that on?”(11, area 1)
The general feeling was that the first person the patient spoke to should be the person who triaged the calls, rather than an operator with no medical training. The most common suggestion was that experienced triage nurses should answer the telephone. As one man put it:
“Prioritise, like a triage nurse, that’s what you need isn’t it, like when you go to casualty you see a triage nurse and she assesses the severity doesn’t she? She can do the job in casualty and I think it’s that type of person that needs to do the job on the phone.” (228, area 3)
Some individuals suggested that call handlers should have high-level training and skills and that these should be reflected in higher status and remuneration.
Waiting
This theme focused on the anxieties people experienced while waiting for health professionals to call them back or make a home visit. People in all groups reported that the period of waiting for their call to be returned was demanding, often spent enduring painful or worrying symptoms. A minority of participants, mainly the parents of small children, said they had been called back quickly. However, one woman identified a lack of guidance on what to do until the doctor called back, which in her case was an hour and a half later:
“but when you phone somebody you would like to think that they’d got a bit of knowledge that they can say, ‘Oh well, if he isn’t sort of like safe, get to hospital—[11: “It’s reassuring”]—“Or ‘Don’t move him and I’ll get a doctor to phone you back straight away’, or ‘I do think it would be quicker or better if you got an ambulance’, but there isn’t any steering. You have to wait [for the doctor to call back] and if you have to wait a long time …” (1, area 1)
Some people felt that they should be informed if there was going to be a long wait for their call to be returned, as one man said:
“There I think the call centre ought to respond and go back to the patient and say, look, we have spoken to the doctor, he is very busy at the moment. Sorry about the delay but he will phone you in X amount of time. But in other people’s cases it would probably set their mind at rest. At least they’re going to respond because after, it had been in the middle of the night, an hour and a half later, blooming heck! Has the doctor forgotten me?” (8, area 1)
Waiting for a home visit was described as an anxious time, during which a few people wondered whether to carry on waiting or to attend the accident and emergency department. One elderly woman who lived on her own said:
“I think that’s the frightening part, of not knowing whether they’re going to turn up in 10 minutes or an hour, or 2 hours, because an hour when you are very ill is a long time to wait.” (101, area 2)
Many people seemed understanding of even lengthy delays, attributing these to emergencies, inadequate staffing levels or excessive use of the service. However, a few people worried that they had been forgotten and felt they should have been called to say that the doctor was on their way:
“they could ring you back up and say …, you told me you are not serious, so you will just have to put up with the discomfort for another half an hour, but we will still come round and see you. A call like that would be right, OK, I can deal with this, I can lie down, shut my eyes, keep still and don’t move, that’s the best thing isn’t it?” (228, area 3)
In the absence of such a phone call, some rang the service back to see what was happening (these people expressed surprise at having to provide basic contact information again). In general, when people had to wait a long time for a health professional they deduced either that the areas covered must be vast, or that there were too few health professionals available to provide the service. In this regard they were curious to know how many doctors provided care and what sort of hours they worked.
Location of consultation
The location of the consultation—that is, on the telephone, at home or in a treatment centre, raised different issues. Most of the individuals who received telephone advice reported that it was very reassuring and exactly what they needed, as the mother of a 2-year-old baby with croup illustrates:
“I was pretty sure what it was and pretty sure what to do. But at 1 o’clock in the morning I needed someone else to tell me that I was right basically, so I phoned up, and they were fantastic. Within I think 2 or 3 minutes of putting the phone down the doctor rung me back and gave the advice and said, ‘If she’s no better in half an hour call back’” (142, area 2)
Similarly, most people were satisfied with the care provided at treatment centres and expressed relief that they were able to access medical care out of hours.
“I was so grateful for that service, somewhere I could go on a Bank Holiday Monday and get treatment into my body right away.” (2, area 1).
Some concern was expressed about getting to treatment centres, however; those who did not drive had to rely on neighbours or relatives to take them, or to pay for a taxi. With regard to home visits, most participants perceived that out-of-hours services were reluctant to undertake home visits, with numerous examples being provided:
“the first thing that they want to know is can you get to them. Save them coming out to you, and you know if your answer is in any way that you can, then you go. They won’t come and see you.” (134, area 2)
“They were trying, yes, both phone calls I had they were both trying to get you to their surgery first and not worry about you, the priority was to try and shift you to them, rather than them coming to you.” (228, area 3)
“I was a bit dismayed about her [doctor] attitude, you know, I told her I wasn’t very well and it seemed as if she was, you know, trying to get me to come up to the hospital to avoid somebody coming out to see me.” (3, area 1)
However, two people in area 2 reported that despite volunteering to go to a treatment centre the doctor had insisted on visiting them at home. Some individuals reported feeling guilty about asking for a home visit, believing that this placed excessive strain on scarce resources.
Quality of clinical care
Most participants expressed satisfaction with the quality of clinical care they received. Most people in areas 1 and 3 were impressed with the out-of-hours health professional they encountered, praising their manner, the treatment and the thoroughness of the consultation. Particular appreciation was expressed for those who did not rush, who explained things clearly, who were confident, professional and caring, and who did not make them feel guilty for using the service:
“The doctor was smashing and very thorough and again he didn’t rush at all. He’d brought stuff for testing urine and he’d brought antibiotics that he was carrying and he was very, very pleasant, wasn’t he? Very nice man, so we enjoyed his visit really and he also didn’t give any impression of, you know, you shouldn’t be calling us out” (206, area 3)
Occasional concerns were expressed about the health professional’s manner, or their ability with the English language, but these were rare. More varied experiences were reported in area 2, and one individual stated that her doctor’s response to a major family crisis was very unsympathetic, contrasting with another’s account of an excellent package of care provided over a bank holiday.
Access to medical history
Several people felt that the out-of-hours service should have access to the general practice records, citing this as especially important for people with chronic conditions. One woman argued for this on account of her rare medical condition:
“I think the only worrying thing from my point of view about the service is they haven’t got access to your GP records, so if you’ve got something like—I had to have three [doctors] out over a weekend because two of them would not give me the drug in the route I have to have it … I ended up spending 20 minutes explaining and debating why this particular drug only works in one particular manner.” (18, area 1)
Uncertainty existed, with some individuals believing that the out-of-hours service already accessed their medical records. One man, who had to repeatedly contact the service, could not understand why the out-of-hours service did not know all about his case because “it’s obviously all computerised” (134, area 2). It was usually within the context of familiarity with the patient’s medical history that nostalgic comments were made about family doctors under previous out-of-hours arrangements.
Collecting medicines
The collection of prescribed medicines raises issues about the availability of transport and resources in the out-of-hours period. For most interviewees, collecting medicines required access to a car, or money for public transport. One woman explained:
“But then say you’ve got children, say your children are poorly so then you get this list [of pharmacies], they give you this list which is fine, that’s brilliant and they show you a list then you’ve got no car so then you may have to try and get another taxi to somewhere else. What if you haven’t got any money on you, you’re talking Bank Holiday Monday. You go to the cash point, its empty. So what do you, unless you’ve got decent neighbours that maybe you can call on?” (2, area 1)
One person reported that he was told his wife should fetch his medication in a taxi even though she was disabled. Another said his wife had to drive a considerable distance one night in a storm to fetch his medication. He suggested that the out-of-hours service should have a motorcycle courier who could deliver medication. As might be expected, the problem of collecting medicines was particularly acute for individuals in rural areas.
DISCUSSION
Summary of findings
Study participants were concerned about the urgency with which their cases were handled and the amount of time they had to wait for a call back or home visit. There was a widespread perception that providers were reluctant to do home visits. Many people expressed anxiety about calling the service and were uncertain whether their call was appropriate or not. This seemed to be partly because they were unsure about the severity of their symptoms and the urgency of the situation, but also because they almost universally perceived that the service was poorly resourced and misused and they did not want to be accused of “abusing” it. Once people had negotiated their way through the initial call-handling process and had finally accessed medical care, they were generally complimentary about the health professionals’ skills and the quality of care received.
Context of the literature
These findings support those of previous qualitative studies in this area, which also found that the decision to call the out-of-hours service is complex1920 and that home visits and swift access to medical care after initial contact are highly valued.781320 Similarly, the sorts of issues raised are in agreement with the domains identified by McKinley and colleagues’ qualitative work conducted a decade ago.21 Foster and colleagues’ findings particularly resonated with ours, in terms of their participants’ emphasis on the importance of continuity of care and their reluctance to “make demands” on the service.7 However, our study revealed the extent of confusion surrounding the newly emerging models of out-of-hours service. The finding that callers were not sure when it is appropriate to contact the service and remained unclear about the processes by which their call was managed, yet remained highly satisfied with the quality of medical care provided is somewhat paradoxical. However, it is consistent with the survey work commissioned by the National Audit Office2 which found that only 1 in 5 service users were dissatisfied with some aspect of the quality of medical care received.
Study limitations
Participation in a focus group takes time and effort. The uptake rate for the focus groups was poor, with most non-participants saying they were too busy, or too unwell to take part. Because most peoples’ contact with the out-of-hours service is probably unremarkable, it could be that the sample was biased towards those with more extreme experiences. However, it seems more likely that our sample was biased in terms of those with an interest in health service issues, since a third of participants or their relatives worked, or had worked, in a health-related field. Although we achieved our aim of obtaining participants who varied in terms of age, geographical area and type of management options received in this relatively small study, we were unable to recruit participants from ethnically diverse backgrounds. Similarly, on pragmatic grounds, our research method excluded individuals who were too unwell to attend a focus group (for example, nursing home residents) or socially marginalised groups (eg, individuals living in temporary accommodation and who are likely to move often). Approaching recent users of out-of-hours services via a general practitioner with whom the patient has a personal relationship may facilitate recruitment to focus groups. Similarly, providing face-to-face interviews may be necessary for socially marginalised groups who might find participation in focus groups too difficult.
Our sample were all recruited through out-of-hours services adopting a broadly similar model of service organisation, which is one of several different models currently available in the UK.12 Our findings around the difficulty in accessing out-of-hours care, and particular the frustrations expressed about the “script-like” call handling may, in part, be because all our services employed non-clinical call handlers as a first point of contact. The degree to which these experiences are common to patients using other models of service, such as the National Exemplar sites,22 where the first point of contact had clinical training (eg, nurse or emergency care practitioner) is worthy of further exploration.
Implications for policy, practice and research
The eight themes emerging from focus groups related to both the quality (location and quality of consultation) and safety (getting through, prioritising calls, waiting, accessing medication information, collecting medicines) of accessing out-of-hours care. Lack of confidence about calling might make it difficult for users to assert the urgency of their situation, possibly one of the reasons why some people felt their cases had not been dealt with quickly enough. Although publicity to allay the public’s fears about “misusing the system” and information about when it is appropriate to use the service might be beneficial, given the limited resources available, services may wish to focus activity on improving the information given to service users. Because people did not understand how the triage system worked, they questioned the qualifications of the call handler (rather than the doctor with whom responsibility lies) when they felt their cases had not been dealt with sufficiently urgently. Some suggested that call handlers needed more training, whereas others felt they should be replaced by triage nurses so that appropriate advice could be given immediately, ensuring patient safety. One study found that a nurse-led out-of-hours service halved the number of cases dealt with by general practitioners, reduced home visits and treatment centre attendance and allowed callers faster access to information and advice.23 Call handlers could also reduce anxiety and improve the quality of service if they uniformly advised people on the likely waiting period before being called back and kept people informed about any delays in responding or visiting. A brief explanation for the script-like questioning process during the initial call would be valued. If this is not explained, it risks being experienced as insensitive, especially by first time callers.
A common perception was that home visits were discouraged by the out-of-hours service. Foster et al suggest that home visits are particularly appreciated by older people and that the new model of out-of-hours care may not suit them.7 Older people may therefore under-use the service, despite their higher morbidity and likelihood of living alone. We suggest care should be taken that the new system does not alienate older people and that efforts are directed towards meeting their needs.
Further work, using different sampling and recruitment methods, is needed to target the experiences of users from ethnically diverse backgrounds and socially marginalised groups. Snowballing sampling techniques, in which individuals from hard to reach groups are identified through direct approaches from health professionals or community teams working closely with individuals from these groups may encourage participation.24 If participation is secured, measures such as the provision of translated research materials or the availability of interpreters will also be necessary to support data collection through focus groups or face-to-face interviews. Previous research with Vietnamese community groups in London19 found that participants’ knowledge about out-of-hours services was limited and that there were communication problems with call answering services and health professionals, which may have compromised aspects of both patient safety and of the quality of care provided. The utility of providers sending out (English language) questionnaires to capture the views of individuals from these groups, as a method for satisfying the national quality requirements,5 must also be critically examined as these groups may also experience difficulties in either receiving or completing questionnaires.
SUMMARY
This study explored the concerns, expectations and experiences of users of out-of-hours healthcare services. The findings were used to inform the development of a survey instrument,25 suitable for the routine collection of data regarding users’ experiences of care, in line with current national quality requirements.
Acknowledgments
We very grateful to all the people who participated in the focus groups, as well as to A Tester, E Bell and H Barker for their help with running the focus groups and/or transcribing the audiotapes.
REFERENCES
Footnotes
Ethical approval: The study was approved by North and East Devon Research Ethics Committee. Ref no: REC 05/Q2102/1.
Funding: The study was funded by the Department of Health.
Competing interests: None.
- Abbreviation:
- PCT
- primary care trust