Article Text

Abstract
Background Structured diabetes care can improve outcomes and reduce risk of complications, but improving care in a deprived, ethnically diverse area can prove challenging. This report evaluates a system change to enhance diabetes care delivery in a primary care setting.
Methods All 35 practices in one inner London Primary Care Trust were geographically grouped into eight networks of four to five practices, each supported by a network manager, clerical staff and an educational budget. A multidisciplinary team developed a ‘care package’ for type 2 diabetes management, with financial incentives based on network achievement of targets. Monthly electronic performance dashboards enabled networks to track and improve performance. Network multidisciplinary team meetings including the diabetic specialist team supported case management and education. Key measures for improvement included the number of diabetes care plans completed, proportion of patients attending for digital retinal screen and proportions of patients achieving a number of biomedical indices (blood pressure, cholesterol, glycated haemoglobin).
Results Between 2009 and 2012, completed care plans rose from 10% to 88%. The proportion of patients attending for digital retinal screen rose from 72% to 82.8%. The proportion of patients achieving a combination of blood pressure ≤140/80 mm Hg and cholesterol ≤4 mmol/L rose from 35.3% to 46.1%. Mean glycated haemoglobin dropped from 7.80% to 7.66% (62–60 mmol/mol).
Conclusions Investment of financial, organisational and education resources into primary care practice networks can achieve clinically important improvements in diabetes care in deprived, ethnically diverse communities. This success is predicated on collaborative working between practices, purposively designed high-quality information on network performance and engagement between primary and secondary care clinicians.
- General practice
- Patient-centred care
- Quality improvement
- Diabetes mellitus
Statistics from Altmetric.com
Background
Type 2 diabetes (T2D) is an important long-term condition, with high societal and economic costs due to cardiovascular and microvascular disease. In the UK in 2010, over 2.7 million people had the condition, predicted to rise to 4 million people by 2025.1 Around 10% of healthcare expenditure in the UK is directly related to diabetes and its attendant complications, and 15% of hospital inpatients have diabetes. Diagnosis of diabetes is associated with a life expectancy shortened by up to 10 years,1 and diabetic complications are multi-system, placing an increasing burden on cardiovascular, renal, ophthalmological, podiatric and vascular services.
It is known that multifactorial intervention, and structured personal care, can reduce complications in patients with T2D.2 ,3 The challenge is to translate evidence from clinical trials into real and equitable improvements in diabetes management in the face of a growing prevalence of the disease.
The problem
General practitioners in the inner London borough of Tower Hamlets serve a population of 260 000, of whom more than 50% are from ethnic minority groups of whom 30% are south Asian and 10% are black African Caribbean.4 There is a rapidly growing prevalence of T2D by virtue of the high proportion of at-risk ethnic populations and high rates of social deprivation.5
In 2008 10 424 people in the borough had T2D (7.1% age standardised to the European standard population),6 and of these, 90% were managed in primary care settings. In 2008 it was recognised that diabetes care in the borough was suboptimal. The Quality and Outcomes Framework (QOF) scores for diabetes were variable, with some among the lowest in the country. There was a very low uptake of diabetic retinal screening compared with the whole of London and England. This prompted us to undertake an additional analysis to examine whether there are differences in screening uptake by the three major ethnic groups in the locality. There were high rates of hospital admissions for diabetes-related complication and little evidence of systematic diabetes care along the lines suggested by the Diabetes National Service Framework.7 It was recognised that to prevent complications it was necessary to provide optimal primary care using evidence-based interventions, including diabetes education, and formal care plans as suggested by the Diabetes National Service Framework. However, it was uncertain what model of care would deliver the most improvement, although there is some evidence to suggest that health gain is greatest when the investment is in primary care.8
This project evaluates an example of system change involving the formation of networks of general practices tasked with collectively delivering an agreed care package for type 2 diabetes, with the aim of achieving a step change in improvement in clinically important indicators of diabetes management.
Key measures for improvement
A number of care package clinical targets were chosen to assess the impact of the network intervention on diabetes care in the borough. The following indicators were financially incentivised:
-
The number of care plans completed in the previous 15 months, with a target of 90%.
-
Proportion of patients attending for digital retinal screen in the previous 15 months, with a target of 80%.
-
Proportion of patients achieving a total cholesterol of ≤4.0 mmol/L and blood pressure ≤140/80 mm Hg with a target of 50%.
-
Network population average glycated haemoglobin (HbA1c) in the previous 15 months, with a target of 7.5% (58 mmol/mol).
Process of gathering information
All local general practices use common data entry templates and the same web-enabled computer system for data recording. We used EMIS Web9 to collect demographic (age, sex, social deprivation and ethnicity) and routinely collected clinical data using the diabetes registers from all 36 general practices in the Tower Hamlets and similar data from two neighbouring primary care trusts (PCTs) to enable local comparison. Information on additional costs associated with network setup and care package funding came from Tower Hamlets PCT. The national QOF provided a further source of comparative data; this was obtained from the QOF online database and all comparisons between localities were made without any reported exceptions.10
Analysis and interpretation
We used Stata V.10 for all the data analyses.
The values of each target for Tower Hamlets were recorded over time and compared with surrounding localities, the whole of London and England.
Using the high levels of ethnicity recording (97%) in the population with diabetes, we undertook an analysis using bivariate statistics to examine differences in retinopathy screening uptake by ethnic group in the three inner east London PCTs (Tower Hamlets, Newham and City and Hackney).
We undertook a logistic regression analysis to determine whether the likelihood of receiving screening differed by ethnic group after adjustment for age, sex and social deprivation (measured using individual level Townsend scores based on the 2001 census).11
Strategy for change
In 2008 Tower Hamlets became a pilot site for integrated care, requiring financial investment and evidence of interagency care to develop new ways of working.12 Tower Hamlets PCT chose to invest in the development of general practice networks across the 36 GP practices. Eight locality-based networks were developed, each consisting of four to five geographically linked practices, to deliver a cluster of four care packages for chronic diseases, one of which was for primary care management of T2D. The activity and costings of the care packages were developed by a group of local hospital and community clinicians supported by project management from a management consultancy firm. The content of the care package was developed with reference to National Institute for Health and Clinical Excellence guidance and the nine key care processes itemised by Diabetes UK.13 ,14
A core component of the care package was the care planning process. This involves active patient recall for an initial appointment to collect biomedical indices (body mass index, BP, renal function, HbA1c, retinal screen, smoking status, foot health check). The patient receives the results to reflect on prior to the care planning review. This consultation involves a 30–45 min meeting with a doctor or nurse trained in motivational interviewing, in which goals for the coming year are tailored to the patient's needs and aspirations, with signposting to local services. Interim discussions through the year review elements of the care plan. The care plan can be seen as an end in itself, empowering individuals to understand their condition, identify treatment goals and use local services. It can also be viewed as a means to an end, in that the aggregated care plans of individuals can support the commissioning plans for a locality.15
A further investment was in the information technology (IT) capacity required to provide real-time tracking of the key performance indicators (KPIs) for each of the care packages. As part of the set-up costs, each of the eight networks was provided with funding for network managers and recall coordinators to work across all care packages, and all networks had initial organisational development training and support. The overall funding given to each network to deliver the diabetes care package was approximately £200 000 (depending on patient numbers and complexity); this was provided as 70% upfront to fund additional clinical capacity and 30% for achieving the care package targets as a network. Networks had autonomy on the use and distribution of funds to achieve the KPI targets. Most developed a diabetes team across the network to provide local leadership and build practice engagement and capacity. Specialist support from community-based diabetes specialist nurses and community consultant diabetologist sessions were commissioned by the PCT.
Robust IT systems and good data quality formed an essential part of the strategy. All Tower Hamlets practices use the medical software EMIS and the locality has been an early adopter of EMIS Web. This allows centrally written searches to be used at the level of primary care networks and practices. Networks are able to run their own systematic call and recall programmes for annual reviews, and other interventions, using centrally designed searches. Defaulter lists can be produced regularly. The development of shared data entry templates encourages the standardisation of activity recording and data coding across the networks. Using credible data directly from practice systems to develop a monthly dashboard of KPIs, which is visible to practices, networks and the PCT commissioners, has been important for clinician engagement. It also enables networks to build reliance on the use of data to drive improvements in performance.
The network structure has enabled peer review of practice figures, alongside sharing ideas for hard to reach and treat groups. Networks were encouraged to develop a variety of approaches to support practices which struggle with performance. An element of healthy competition between networks has developed. See figure 1 for a summary of the network intervention.
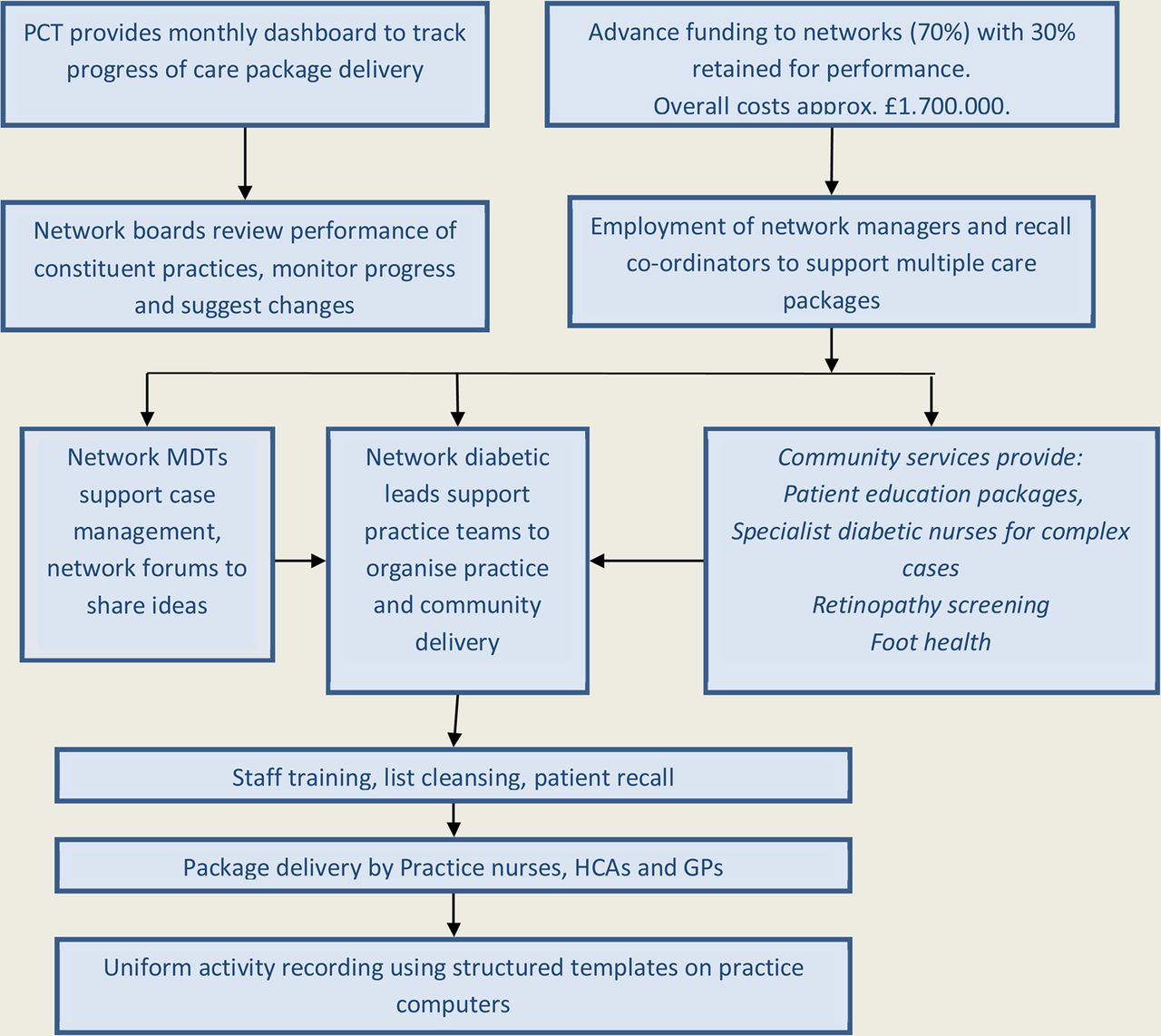
Summary of network intervention. GP, general practitioner; HCA, healthcare assistant; MDT, multidisciplinary team.
The first wave of three networks started the care package in October 2009, with the remaining five networks starting in April 2010. The effective, full implementation date is deemed to be April 2010.
Effects of the intervention
Care planning for people with diabetes involving a collaborative consultation based on shared decision making and support for self-management was a core component of the care package and built on the experience in Tower Hamlets as a pilot site for the Year of Care in Diabetes.16
The proportion of patients with a care plan completed in the previous 15 months rose sharply from 10% in the first quarter of 2009 to 88% in the first quarter of 2012. No regional or national comparisons are available for this component of the care package.
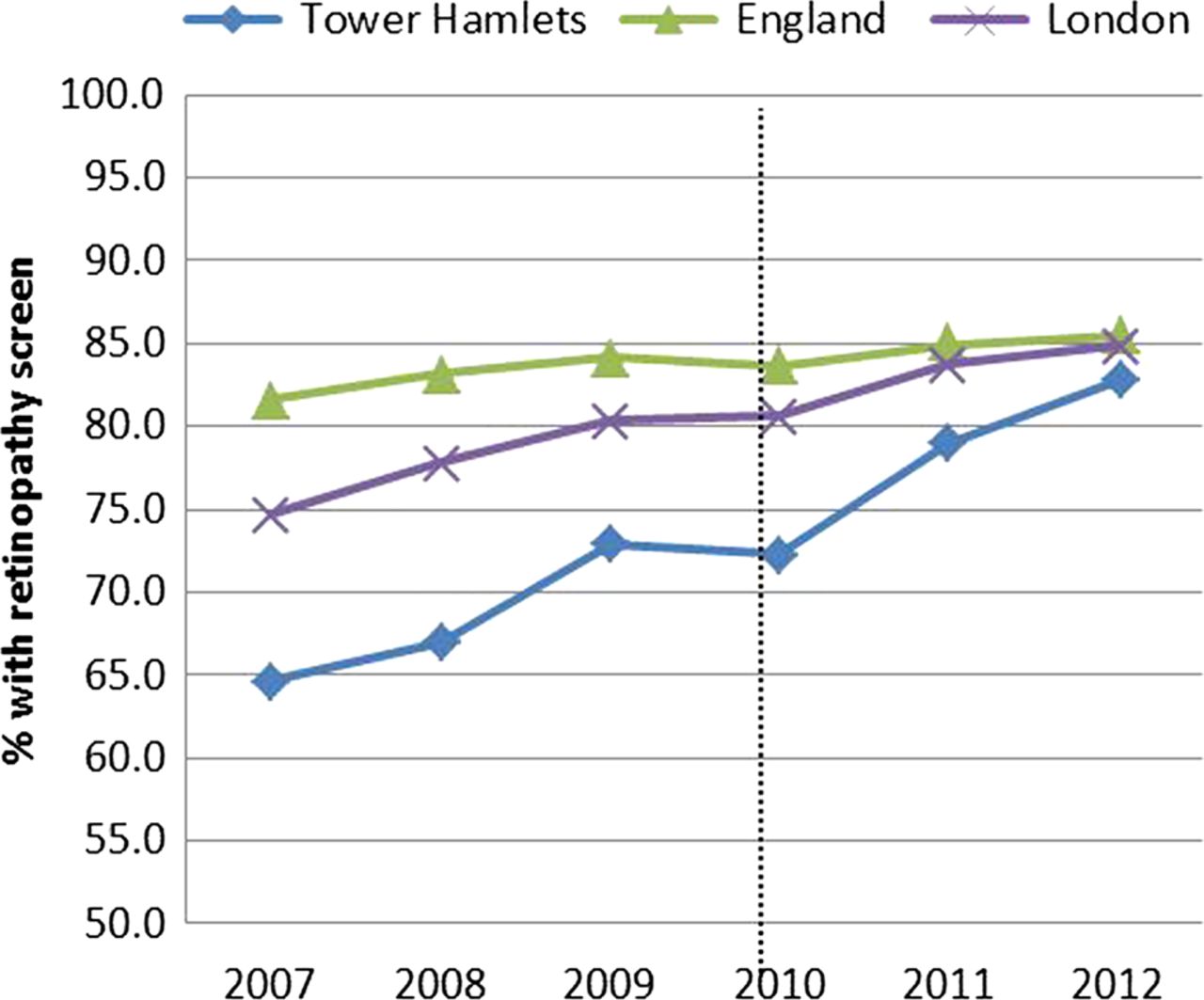
The proportion of patients attending for digital retinal screening in the previous 15 months improved from 72% in the first quarter of 2009 to 82.8% in the first quarter of 2012.
Comparison with QOF data from London and England demonstrate that rates in Tower Hamlets show a step change catch up between 2009 and 2012; see figure 2.
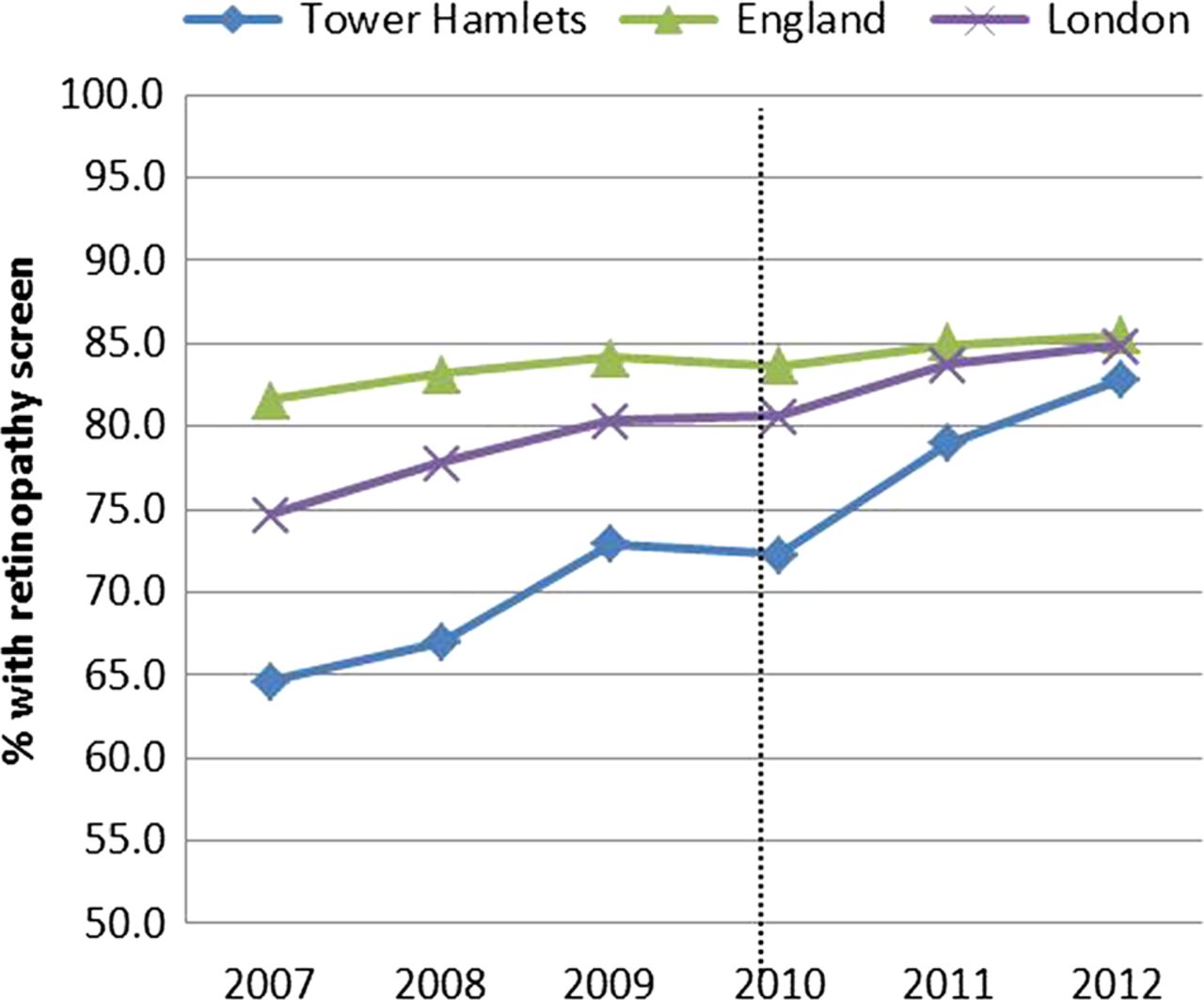
Percentage of people with diabetes with annual retinopathy screening completed. Tower Hamlets rates compared with London and England (Quality and Outcomes Framework (QOF) data, no exception reporting). Data from QOF (http://www.gpcontract.co.uk).
The care package joint target for cholesterol and blood pressure management was for 50% of patients to have a cholesterol value of ≤4.0 mmol/l combined with a blood pressure of ≤140/80 mm Hg. The rate of achievement for this target rose from 35.3% to 46.1% over the observation period.
Regional and national comparisons from QOF data use separate targets for cholesterol (≤5.0) and blood pressure of ≤145/85 mm Hg (≤150/90 for QOF 2012). Figures 3 and 4 illustrate the improved performance of Tower Hamlets pre and post the start of the intervention in late 2009 in comparison to regional and national figures. In 2012, Tower Hamlets ranked top among all PCTs in England for cholesterol and blood pressure control.8

Proportion of people with diabetes with cholesterol ≤5 mmol/L. Tower Hamlets rates compared with London and England (Quality and Outcomes Framework (QOF) data, no exception reporting). Data from QOF (http://www.gpcontract.co.uk).

Proportion of people with diabetes with blood pressure ≤145/85 mm Hg. Tower Hamlets rates compared with London and England (Quality and Outcomes Framework (QOF) data, no exception reporting). Data from QOF (http://www.gpcontract.co.uk).
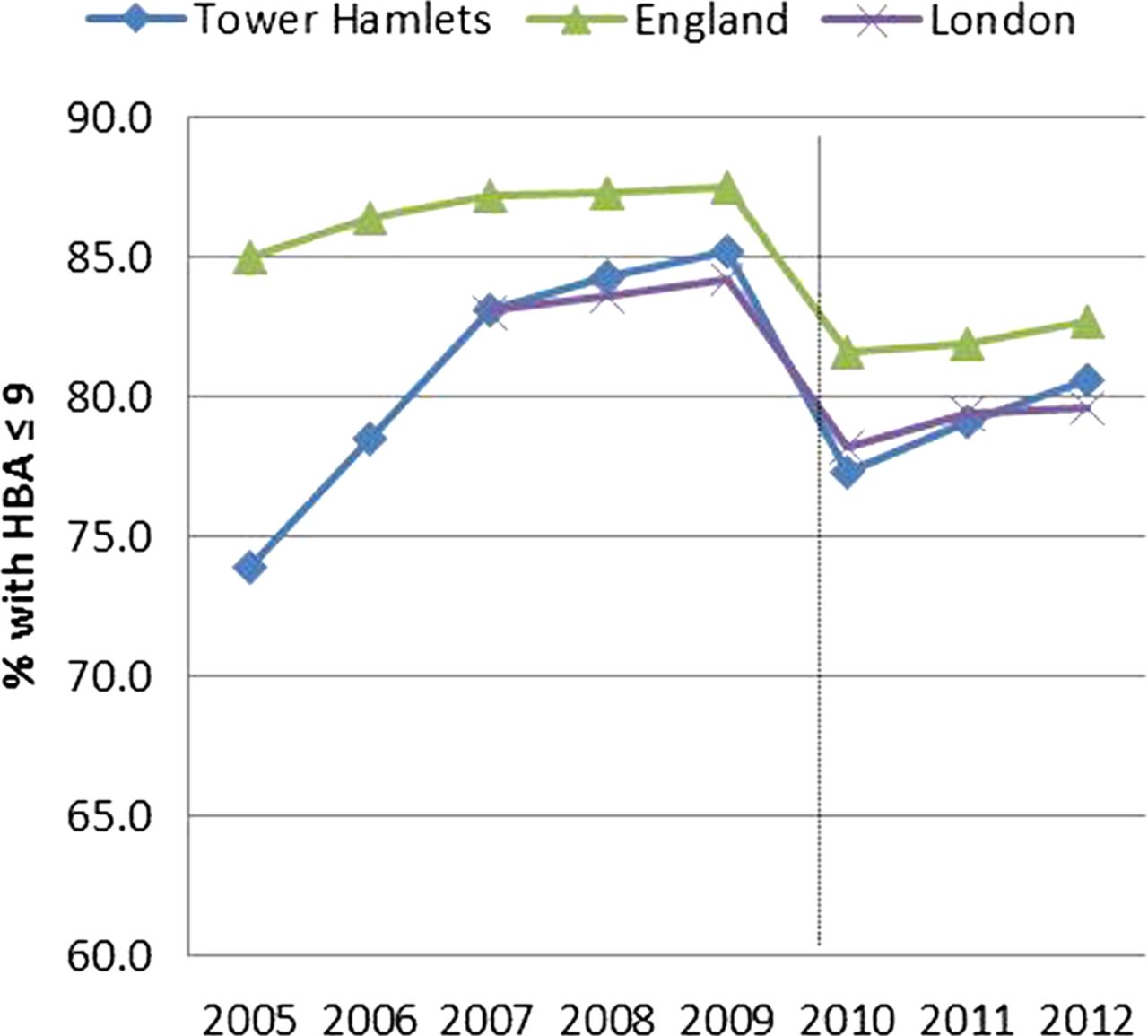
The average HbA1c value of all patients with T2D in Tower Hamlets fell from 7.80% (62 mmol/mol) to 7.66% (60 mmol/mol) between 2009 and 2012. This did not meet the care package target of 7.5% (58 mmol/mol).
There are no regional or national data relating directly to this target, so we have used comparison with the QOF target of achieving an HbA1c ≤9% (72 mmol/mol). Figure 5 illustrates that Tower Hamlets, along with other London PCTs, lag behind England on performance in achieving this target in large part because of high values in London's large south Asian and black African/Caribbean groups.18

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of people with diabetes with haemoglobin (HbA1c) ≤9% (75 mmol/mol). Tower Hamlets rates compared with London and England (Quality and Outcomes Framework (QOF) data, no exception reporting). Data from QOF (http://www.gpcontract.co.uk). DCCT laboratory harmonisation occurred in 2009, with adjustment of values.
Differences in retinal screening uptake by ethnic group
We undertook a logistic regression analysis to determine whether the likelihood of receiving screening differed by ethnic group after adjustment for age, sex and social deprivation (measured using individual level Townsend scores based on the 2001 census).
Table 1 shows that when age, gender and social deprivation are taken into account, the white population in comparison to the reference South Asian group is significantly less likely to complete retinal screening.
Odds of completing retinal screening in east London, by ethnicity
Lessons learnt and next steps
We have found that significant clinical improvements in diabetes care can be made by a combination of financial and organisational investment into networks of general practices, using incentive payments alongside educational facilitation with specialist input. We are able to demonstrate that this is associated with a step change improvement in blood pressure, cholesterol and retinal screening rates in comparison to England and London.
The targets for the care package were designed to challenge performance by the networks. Although HbA1c has not fallen to the planned target it may well be that the cultural and behavioural shift required to achieve this will take a longer time to be seen.
Similarly during the observation period the challenging care package targets for combined cholesterol and BP values were not met in full, and in 2012 these targets were separated to allow more consistent comparison with national QOF indices. Indeed for cholesterol management and blood pressure control, Tower Hamlets PCT achieved among the best results in England, despite serving a mobile, multiethnic population ranked as the third most socially deprived local authority area in England.
It is encouraging to find that the South Asian ethnic group, which forms the bulk of the diabetic population, achieved higher rates of retinal screening than white population groups in east London. However, these rates still lag behind rates for London overall and need further sustained attention to improve. Understanding ethnic differences in uptake will support the development of targeted local interventions to improve rates.
Integrated care programmes aim to improve clinical outcomes and patient experience by developing a range of organisational and clinical integration across primary, community and hospital settings.18 ,19 Programmes also aim to shift care from expensive acute hospitals to cheaper primary and community service settings for those conditions best managed out of hospital.13 Programme organisational structure can take a variety of forms and there is little consensus on which structures best achieve and sustain the desired changes.20–22
In common with other integrated care diabetic programmes23 we found that a key factor for success has been the engagement of clinicians in the planning, implementation and governance of the process, and in contributing to educational support through multidisciplinary team (MDT) meetings. However, the unique contribution in this initiative has been the financial investment in a practice network structure and organisation, alongside investment in an IT backbone to support the development of real-time information on clinical performance which has high face validity for clinicians and commissioners. Devolving resource and responsibility to groups of local providers enabled the practices to find collective local solutions to deal systematically with the complexities and fragmentation of existing care pathways.24
The decision to fund networks rather than individual practices encouraged a process of peer scrutiny and collective management of the financial resource. Network boards reviewed practice performance against targets and the clinical leads worked with practice teams to support delivery.25 The introduction of a bi-monthly community diabetic MDT meeting, led by a consultant in diabetes, provided ongoing educational support to all primary care clinicians, with discussion time set aside for analysis of KPIs, discussion of recent advances in treatment and individual discussion of difficult cases. The consultant also provided rapid access to advice by email or telephone. These elements provided an alternative source of clinical support to reduce the need for outpatient referral.
Moving forward, there is a process of review of the care packages on a yearly basis. Targets are reviewed and stretched if necessary or dropped in favour of other targets. We hope to develop greater input from patients to determine whether they consider the process of diabetes care has been enhanced as a result of care packages.
References
Footnotes
-
Contributors SH, JR and TC had the original idea for the paper. RM provided the analysis and presentation of the data. TC,SH, JR wrote the first and final drafts. SH is guarantor.
-
Funding Tower Hamlets PCT.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.