


Abstract
Background GPs occupy a pivotal position in relation to providing services to opiate misusers in the UK, and this is now cited to support initiatives in other countries.
Aims To investigate GP involvement in the management of opiate misusers; and to examine the nature of this prescribing of methadone and other opioids.
Design GP data collected via self-completion postal questionnaire from a 10% random sample of the 30 000 GPs across England and Wales. Patient prescription data obtained on opiate misusers treated during the preceding 4 weeks.
Setting Primary healthcare practice in England and Wales in mid-2001.
Method A questionnaire was mailed to a random 10% sample of GPs stratified by number of partners in the practice, with three follow-up mailshots. Data on drugs prescribed by these practitioners were also studied, including drug prescribed, form, dose and dispensing arrangements.
Results The response rate was 66%. Opiate misusers had been seen by 51% of GPs in the preceding 4 weeks (mean of 4.1 such patients), of whom 50% had prescribed opiate-substitution drugs. This provided a study sample of 1482 opiate misusers to whom GPs were prescribing methadone (86.7%), dihydrocodeine (8.5%) or buprenorphine (4.4%). Of 1292 methadone prescriptions, mean daily dose was 36.9 mg — 47.9% being for 30 mg or less. Daily interval dispensing was stipulated by 44.6%, while 42.9% permitted weekly take-away supply.
Conclusions In 2001 nearly three times as many GPs were seeing opiate misusers than was the case in 1985. Half were prescribing substitute-opiate drugs such as methadone (to an estimated 30 000 patients). However, there are grounds for concern about the quality of this prescribing. Most doses were too low to constitute optimal methadone maintenance; widespread disregard of the availability of supervised or interval dispensing increases the risks of diversion to the blackmarket and deaths from methadone overdose. Increased quantity of care has been achieved. Increased quality is now required.
INTRODUCTION
GPs are at the heart of many of the recent developments of the NHS in the UK1-4 — not just strategically but also at the level of practical implementation. This has included the provision of care to opiate misusers — with strong endorsement from some GPs,5-12 but with others expressing concern or opposition.13-16 Official recommendations have typically included guidelines on the provision of methadone as part of the treatment of the opiate misuser;17,18 yet little is known about how attitudes and behaviour of GPs in England and Wales have changed since the previous national survey in 1985.19,20 A smaller survey in Scotland was reported in 1998.21 Furthermore, even less is known about which treatments are actually prescribed to opiate misusers by GPs; the daily doses they select; or the dispensing arrangements that they stipulate.
Internationally, considerable interest exists in the UK's encouragement of GPs to be involved in treating opiate misusers, as it is not generally practised in other countries. The favourable impression from the UK has encouraged other countries (including Canada, France and Australia and, more recently, the US) to introduce, or to consider the introduction of, their own variants of this ‘office-based practice’.22-29 However, the UK is ill-equipped to answer questions, apart from reference to a few local or regional reports.8-12;15;30-31
The previous substantial national (England and Wales) survey of GPs and their management of opiate misusers undertaken by Glanz et al19,20 found that 19% of responders had seen an opiate misuser during the previous 4 weeks, although the more recent study in Scotland21 found higher levels. However, GPs' prescribing practices were not significantly explored. This area was specifically included within the 2001 national survey of GPs, and these prescribing data are reported here, alongside a report on the attitudes and levels of activity of the random sample of GPs from across England and Wales.
METHOD
A random 10% sample of the approximately 30 000 GPs in England and Wales, stratified by number of GP partners in the practice, was obtained from a commercially available database. A questionnaire was developed utilising some items from the 1985 Glanz et al questionnaire, with expansion on selected areas. The domains covered by the questionnaire included: the GPs' current involvement in treatment provision; attitudes and beliefs about managing drug misuse; appropriateness of, and confidence in ability to provide, a range of services; and availability of local support. GPs were also asked to provide data on their recent contact with opiate misusers and anonymised data on prescriptions written in the 4-week period prior to completing the questionnaire.
In mid-2001 (and after pilot testing), the questionnaire was mailed to the 10% random sample (n = 3023 GPs), with three repeat mailshots at monthly intervals to non-responders. GPs were offered a £10 gift voucher on return of the completed questionnaire (voucher funding kindly supplemented by the Substance Misuse Advisory Service). In the final mailshot, a shortened version of the questionnaire was used to elicit a maximum response rate to certain key items (for which a £5 gift voucher was offered).
Over four mailshots, 1999 GPs responded (66% of the study sample). Data on opiate-substitution prescriptions given in the preceding 4-week period were also collected. For the first three mailshots, the questionnaire included a grid (similar to that previously used32,33) for entering details of relevant prescriptions for opiate misusers in the preceding 4 weeks – thereby obtaining data from 1680 GPs (that is, from mailshots one to three; 84% of the responder sample and 56% of the full study sample).
RESULTS
Overall, a 66% response rate was achieved – a 56% (1682 out of 3023) response rate after the first three mailshots (providing information on the full questionnaire) and a further 10% (n = 317) to the fourth mailshot (shortened questionnaire). Four per cent (n = 111) replied stating that they refused to complete the questionnaire. Ninety-four per cent of responders were the original recipients of the questionnaire (1652 out of 1764, data missing on a further 235 cases) with the remainder being completed by one of the other GPs in the practice.
Characteristics and clinical practice of the GP cohort as a whole
Demographics
Responders had been qualified as a doctor for a mean of 20.8 years (standard deviation [SD] = 8.2, range 1–45 years, n = 1976), and working in general practice for a mean of 14.4 years (SD = 8.1, range 0.08–43 years, n = 1963). A third of responders (33.5%; 667 out of 1994) were female (data missing for 5) and the mean age of the sample was 44.8 years (SD = 8.6, range 27–69 years, n = 1384 (data missing, 615). The mean practice size was 8517 patients (SD = 4454, median = 8000; range 600–34 000, n = 1959). Over three quarters of responders (78.5%; 1431 out of 1823) worked full time. There was a mean of 4.3 full-time equivalent GPs at the practice (SD = 2.1; range 1–15; n = 1981; data missing, 18).
How this fits in
No national survey of GPs in England and Wales and their involvement in caring for opiate misusers has been published since the mid-1980s. Since that time, major changes have occurred in the size of the problem and in the proposed extent and nature of the primary care response. This paper provides more recent data on GP involvement. Nearly three times as many GPs were seeing opiate misusers in 2001 than in 1985, with half of these GPs prescribing methadone or other substitute drugs. However these prescriptions are mostly for doses significantly below levels recommended for maintenance treatment, and still permit a disturbingly large amount of weekly take-home doses.
Forty-one per cent of responders (822 out of 1990) categorised their practice as being in an ‘urban’ setting, 27.7% (552 out of 1990) in a ‘suburban’ setting, 16.7% (n = 333) in a ‘rural’ setting and 14.2% (n = 283) as ‘other’ (market town, inner city, mixed rural and urban, university campus) (data missing, 9).
Practice policies
In the first three mailshots, GPs were asked about practice policies (Table 1) (two GPs who had seen opiate misusers extensively in settings outside of general practice have been excluded from this section). Over half (59.1%) indicated that there was a practice policy to manage opiate misusers in formal shared-care arrangements. Three quarters (77.8%) did not limit the number of opiate misusers who were patients at the practice and the majority (88.0%) did not limit the hours during which they could be seen. However, one third of GPs (36.4%) said that care of opiate misusers was not part of the work of their practice.
Which of the following applies to your practice?a
Generalist or specialised generalist
The 1999 publication Drug Misuse and Dependence – Guidelines on Clinical Management defined three categories of doctor — the ‘generalist’, the ‘specialised generalist’ and the ‘specialist’.18 From the first three mailshots, 5% (80 out of 1632) considered themselves to be specialised generalists (mailshots one to three, n = 1682; data missing, 50). Of the GPs not working in single-handed practices, 10% (156 out of 1551; data missing, 8) reported that one of their colleagues was a ‘specialised generalist’. A total of 12% of practices (207 out of 1666; data missing 13) had a ‘specialised generalist’ (3 practices are represented twice in these first 3 mailshots).
In some localities, extra funding is made available to GPs who prescribe for opiate-dependent patients. Twenty-one per cent (330 out of 1587 who responded to mailshots one to three) were paid additional remuneration for prescribing methadone for this patient population.
Activity during the previous 4 weeks
Half of the GPs (50.6%; 1011 out of 1997) had seen at least one opiate-misusing patient during the previous 4 weeks (data missing on a further 2 cases). Two GPs were excluded from further analysis as they had seen 110 and 140 patients, respectively, in the previous 4 weeks, but not solely in a general practice setting (they also worked in a drug dependency unit or drug team clinic). A further four GPs were excluded because although they had seen at least one opiate misuser in the previous 4 weeks, they did not specify the total number they had seen. The remaining 1005 GPs had seen a total of 4099 opiate misusers during this time, giving a mean of 4.08 per GP (SD = 6.07, range 1–60).
GPs who responded to the first three mailshots provided more complete data on the prescriptions they had given to a total of 3508 different patients who had been seen, for problems associated with misuse of heroin in the previous 4 weeks, by 859 GPs (mailshot 1–3). Seventy-three per cent of patients (2534 out of 3458, data from 850 GPs) were male. Fewer than 1% (14 out of 3340) of patients were <16 years; 46.8% (n = 1563) were 16–24 years; 46.5% (n = 1552) were 25–40 years; and 6.3% (n = 211) were >40 years (data from 845 GPs). The proportion of patients new to the GP with regard to their opiate-misuse problem was 14.9% (519 out of 3477, data from 850 GPs).
GPs who had not seen any opiate misusers in the previous 4 weeks were asked to give reasons for this (mailshots one to four). They were able to provide more than one reason, hence the percentages total more than 100. A total of 986 GPs had not seen any opiate misusers. For 41% (n = 402) of GPs, none had attended; for 23.6% (n = 231) no opiate misusers were registered with the practice; for 20.0% (n = 196) opiate misusers were seen by another GP in the practice; for 22.3% (218 out of 979) they were unwilling to treat opiate misusers; and for 15.3% (n = 150) miscellaneous ‘other’ reasons were given.
Prescribing substitution therapies
Half (50.2%; 506 out of 1007) of the GPs who had seen at least one opiate misuser had prescribed opiate substitutes. Of the 506 GPs who had prescribed, 483 provided information on the number of patients to whom they had prescribed. Fuller data on drugs prescribed are reported later in this paper.
Comparison of GPs who had, or had not, attended or prescribed to an opiate misuser
Table 2 shows data comparing GPs who saw at least one opiate user in the previous 4 weeks with those who did not. GPs who had seen at least one opiate misuser were more likely to be male and had worked slightly less time in general practice. They were more likely to work in a practice that limited the number of opiate misusers who were patients at the practice, and to work in a locality where remuneration was provided for prescribing to opiate misusers.
Comparison of GPs who saw at least one opiate misuser with those who saw none in the previous 4 weeks.
Comparison of prescribing or not, among those who saw at least one opiate misuser
The sample for the following analysis comprises the 1007 GPs who had seen at least one opiate misuser in their GP practice in the previous 4 weeks and compares the 506 who prescribed substitution therapies with the 500 who did not (data missing for one case). GPs who prescribed to opiate misusers were significantly more likely to be male, to describe themselves as ‘specialised generalists’, to work in practices where there were other ‘specialised generalists’, and to work in practices with smaller patient numbers. They also tended to work in practices that limited the number of opiate users who were patients and the number of hours during which these patients could be seen, and in localities where funding was provided for this type of work (Table 3).
Comparison of prescribing or not, among those who saw at least one opiate misuser.
Substitute-opiate drugs prescribed to opiate addicts: dose and dispensing arrangements
Fuller prescribing data were obtained from GPs who responded to the first three mailshots: 430 GPs had prescribed opioids to patients over the preceding 4-week period, and 418 provided more detailed information. One GP had prescribed to 110 patients and has been excluded as this work was not conducted solely in general practice. One further GP did not provide valid prescription data, resulting in a final valid sample of 416 doctors who, between them, provided data on the prescriptions for substitute opiates given to 1482 opiate misusers in the preceding 4-week period (1491 opiate prescriptions: 9 patients received 2 different opiate preparations). Thirty-nine per cent (n = 161) of these GPs had prescribed to only one such patient; 41% (n = 170) had prescribed to 2–4 patients; a further 16% (n = 68) to 5–10 patients; and the remaining 3% (n = 17) to >10 such patients.
Data on the 1491 treatments from these 416 GPs comprise the data set that is the basis of the analyses and report in the next section. When different from these sample sizes, the new denominator is indicated. These analyses are presented in two main sub-sections. Firstly data are presented on features of all of these prescribing treatments. Thereafter, in view of the dominance of methadone, this receives a separate more in-depth analysis. Finally, a brief sub-section reports on less frequently prescribed opioids.
Analysis of the full sample of 1491 opiate-substitution treatments
The 1491 treatments are dominated by methadone, which comprised 86.7% (n = 1292) of the substitute-opiate treatment prescribed by these GPs over this 4-week period. The next most commonly prescribed opioid was dihydrocodeine (8.5%; n = 126), followed by buprenorphine (4.4%; n = 65). Other opioid drugs comprised less than 1%.
Two-thirds (64.6%, 932 out of 1443; data missing for 48 cases) of these opioid prescriptions had been issued in the context of a local ‘shared-care’ arrangement.6-12 However, while it was similarly common for both methadone and buprenorphine prescribing to be within such shared-care arrangements (68.6%, 859 out of 1253; data missing for 39 cases and 62.5%, 40 out of 64; data missing for one case, respectively), this was not the case with dihydrocodeine prescribing, of which only 26.7% (32 out of 120; missing data for six cases) was within shared-care arrangements.
The majority of these substitute-opiate prescriptions were for the drug in oral liquid form (83.4%; n = 1230); 15.3% (n = 225) for the drug in tablet form; and 1.3% (n = 19) for the drug in the form of injectable ampoules (data missing for 17 cases). However, this distribution was not maintained across the different substances prescribed. For example, only 37 out of the 225 prescriptions for tablets were for methadone, while all 19 of the prescriptions for opiates in ampoule form were for methadone.
Almost half of these prescriptions (47.2%; 668 out of 1415) were for a single weekly, fortnightly, or monthly pick-up from the dispensing pharmacy, with only 41.1% (582 out of 1415) being for daily pick-up (special prescription pads are issued to GPs for this specific purpose). For this analysis, we have considered prescriptions to be dispensed on 5, 6 or 7 days per week as being for daily pick-up, as with earlier reports.32,33 (Pick-up data are missing for a further 72 cases, plus four cases of one-off prescriptions that have been excluded from the analysis). The pick-up arrangements are examined in more detail in the next section, which restricts itself to the methadone prescriptions. The mean daily dose for each of the three more commonly prescribed opioids are displayed in Table 4.
Opioid drugs prescribed to opiate misusers by GPs in England and Wales, 2001.
Analysis of the 1292 methadone substitution treatments
Methadone was the drug prescribed in 1292 (86.7%) of the treatments. Information about the form of the drug was provided for 1286 (99.5%) of these methadone prescriptions.
Dose of methadone
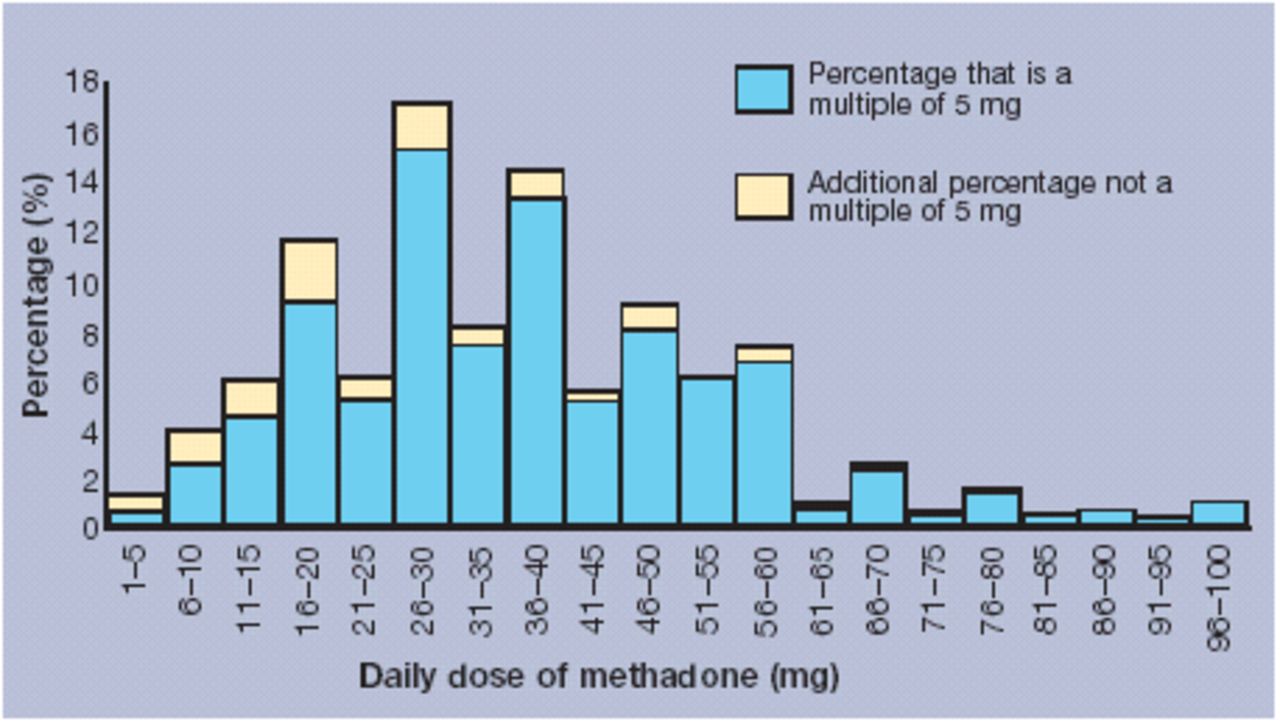
The mean daily dose of methadone in these prescriptions was 36.9 mg (range 1–305 mg; mode = 30 mg; SD = 21.2). The two most commonly prescribed daily doses were 30 mg and 40 mg of methadone daily. Indeed, these two doses made up 29.4% of all methadone prescriptions (15.7% and 13.7%, respectively), with the daily doses of 20 mg and 50 mg comprising a further 17.7% (9.2% and 8.5% respectively). Thus, these four doses made up nearly half of all daily doses. Nearly half of all methadone prescriptions (48.1%) were for a daily dose of ≤30 mg, with nearly three quarters (70.6%) being for a daily dose of ≤40 mg. A small number (3.4%) of prescriptions were for a daily dose of ≥80 mg, with 1% being for a daily dose of ≥100 mg. The distribution of daily doses of methadone is displayed in Figure 2.
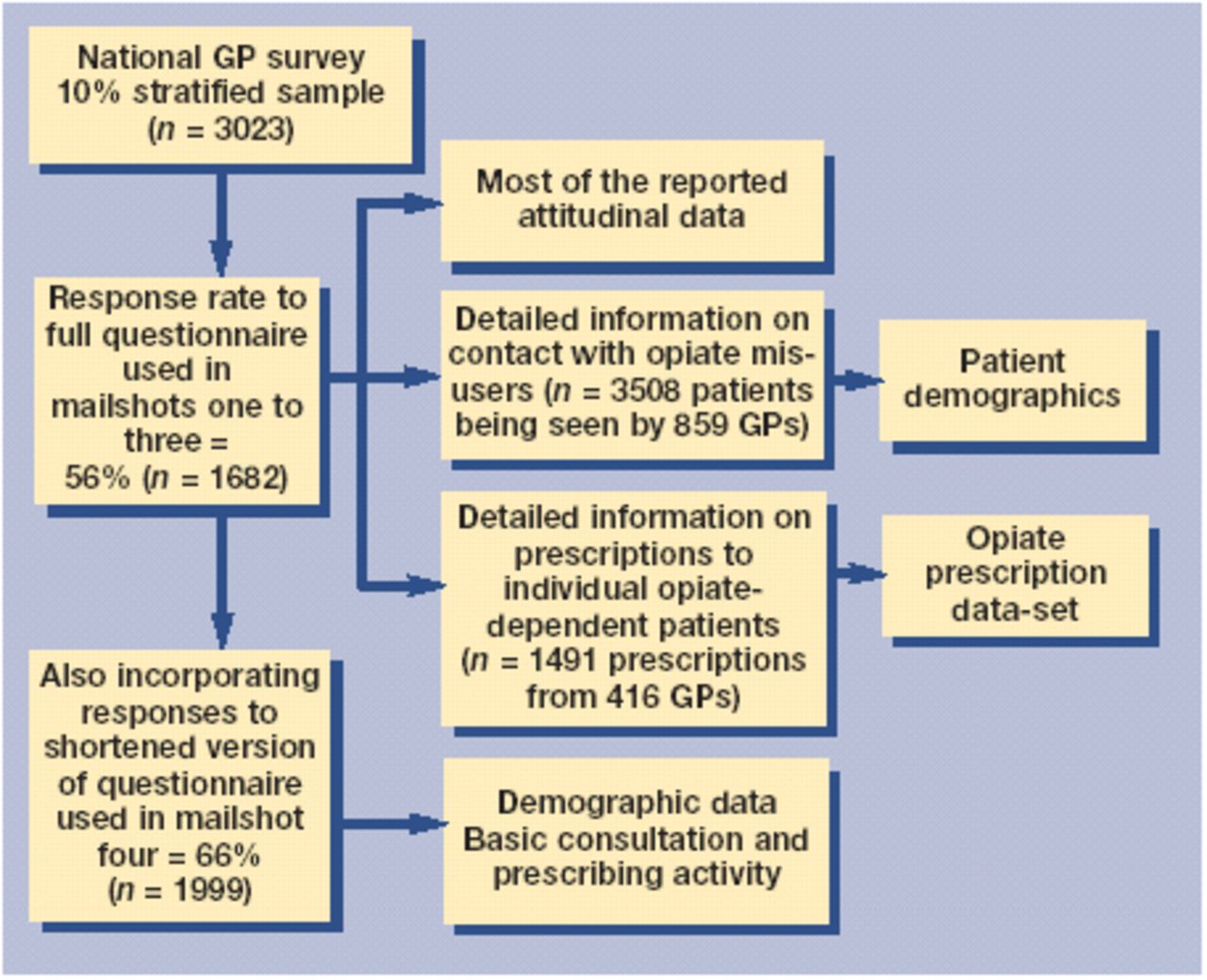
National GP survey: samples and subsamples.

Methadone prescriptions: distribution of daily dose prescribed by GPs in England and Wales, 2001. Eighty-eight per cent were for a multiple of 5 mg. (Three prescriptions for daily doses >100 mg not displayed: 170, 255 and 305 mg.)
A saw-tooth effect can be seen in the daily dose bands, with daily doses that are a multiple of 10 (20 mg, 30 mg, 40 mg, etc) being much more likely to be selected than intervening doses (25 mg, 35 mg, etc). Furthermore, the effect is even more pronounced with the raw data (although too detailed to display graphically or in a table), as 88% of all methadone prescriptions were for a specific daily dose that was a multiple of 5 mg.
Form of methadone
The majority (n = 1230; 95.6%) of methadone prescriptions were for the oral liquid form of methadone (such as methadone 1mg/ml), with only 37 (2.9%) prescriptions being for methadone tablets, and only 19 (1.5%) for injectable methadone ampoules.
Interval dispensing arrangements for methadone
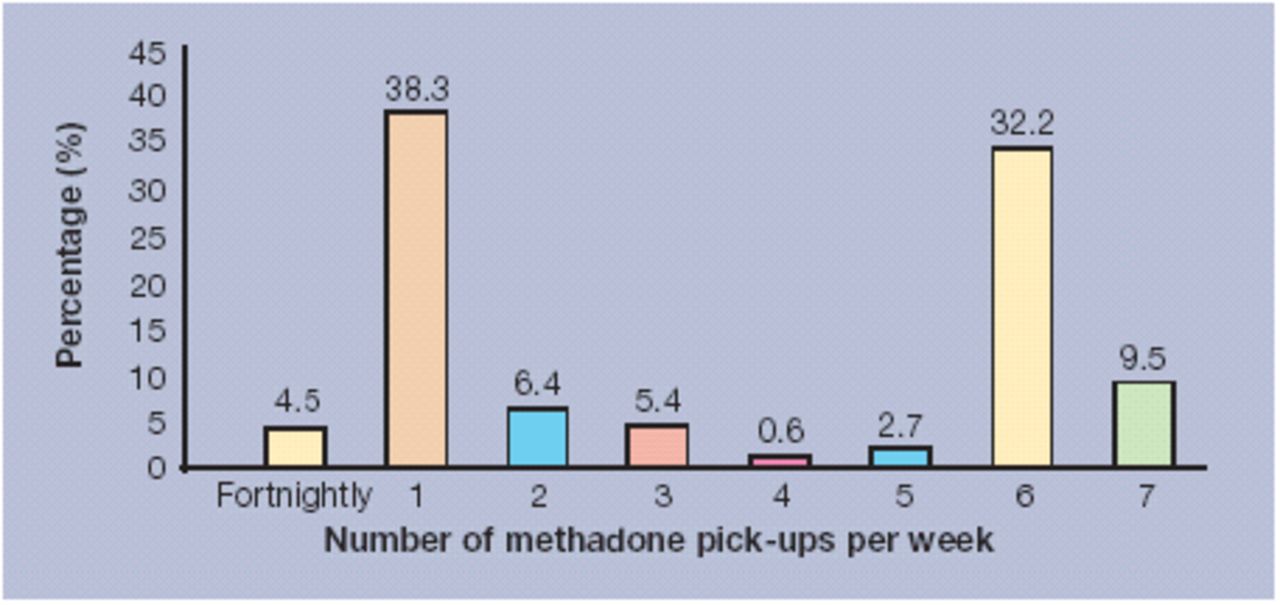
Figure 3 shows the frequency of use for different possible pick-up arrangements. A value of 1 on the x-axis represents a single collection per week, while the value 6 on the x-axis indicates a commonly used arrangement in the UK of ‘dispense daily and on Saturday for Sunday’.
{kind=link}
{kind=link}
{kind=link}
Methadone prescriptions: distribution of dispensing arrangements (seven pick-ups per week = daily collection, etc). (Two prescriptions for a single monthly pick-up, and three for pick-up twice a day are not shown.)
Two dispensing frequencies (weekly and six times per week) between them accounted for nearly three-quarters of all methadone prescriptions, 38% of the methadone prescriptions being for a weekly pick-up, and 32% being for pick-up on 6 days per week.
Given the uneven distribution and differing significance of different numbers of dispensings per week, these have been grouped as ‘daily’ (to include five, six and seven dispensings per week), ‘several times per week’ (to include two, three or four dispensings per week) and ‘weekly’ (to include the small number of fortnightly and monthly dispensings along with weekly dispensing) to enable statistical analysis as undertaken in earlier studies.32,33
Of these prescriptions, 44.6% were for ‘daily’ dispensing (550 out of 1232), while 12.4% (n = 153) were for ‘several times per week’ and 42.9% (n = 529) for ‘weekly’ dispensing. Mean daily doses of methadone were 37.8 mg for ‘daily’ dispensed methadone prescriptions, 42.4 mg for ‘several times per week’ prescriptions, and 34.8 mg for ‘weekly’ pick-up prescriptions.
Different dispensing arrangements were generally stipulated with prescriptions for methadone tablets and ampoules. Sixty-two per cent (21 out of 34) prescriptions for methadone tablets were for ‘weekly’ pick-up, and only 21% (n = 7) for ‘daily’ pick-up (data missing for a further 3 cases). For methadone ampoules, 72% (13 out of 18) of prescriptions were for ‘weekly’ pick-up and only 22% (n = 4) for ‘daily’ (data missing for one further case).
Dihydrocodeine and buprenorphine
Marked differences were noted in the dispensing arrangements for dihydrocodeine, although the special regulations (that enable the prescribing GP to instruct daily dispensing of opioids) do not apply to dihydrocodeine: 89.8% (n = 106) of the 118 dihydrocodeine prescriptions were for ‘weekly’ dispensing, 4.2% (n = 5) were ‘several times per week’, and 5.9% (n = 7) were for ‘daily’ dispensing (data missing for a further seven dihydrocodeine prescriptions, and a further one-off prescription).
In contrast, the dispensing arrangements for buprenorphine were similar to methadone, with 49.1% (n = 27) of the 55 buprenorphine prescriptions being for ‘weekly’ dispensing, 12.7% (n = 7) being ‘several times per week’, and 38.2% (n = 21) being for ‘daily’ dispensing (data missing for a further 10 cases).
DISCUSSION
Summary of main findings
The first important observation is that GPs in England and Wales are substantially involved in managing opiate misusers. Half of all GPs who responded had seen an opiate misuser in the preceding 4 weeks, and half of these GPs (25% of the total sample) had prescribed opiate-substitution therapies. Over two-thirds of patients were prescribed opiate substitutes. The extent of this involvement is markedly greater than in earlier years.
Some crude estimates can be made of the total number of opiate misusers receiving substitute-opiate drugs from GPs in England and Wales at any single point in time. If the findings from our random sample are assumed to be generalisable to the national GP population (approximately 30 000), then this points to a figure of approximately 62 000 opiate misusers being seen by GPs over this 4-week period in 2001. Alternatively, if we presume that our findings are not generalisable to the non-responder population in the survey, but instead assume that none of this non-responder sample attended or treated any opiate misusers, then this would give a lower (but still substantial) figure of approximately 41 000 opiate misusers being seen by GPs across England and Wales over this 4-week period in 2001. The true figure will lie somewhere between these estimates. We can also estimate the national extent of prescribing by GPs to opiate-dependent patients by extrapolating from the responses of these GPs: and thus it would indicate that somewhere in the order of 30 000 patients were receiving methadone (mostly oral syrup/linctus methadone), 2000 receiving dihydrocodeine, and 1000 receiving buprenorphine.
Comparison with existing literature
Compared to the 1985 study (that employed similar methodology), we have found evidence of a much higher level of activity — half (51%) having attended an opiate misuser within the last 4 weeks (compared to 19% in 1985), who had seen a mean of 4.1 opiate misusers during this time (compared to a mean of 2.0 in 1985), and of whom half (50%) had prescribed an opioid drug as part of the treatment response (compared to about a third (31%) in 1985). (The Glanz data from 1985 are not directly comparable for this last variable as Glanz did not specifically ask about the actual drugs prescribed and did not specify the time period to which the question applied.) Substantially more work is now being carried out by GPs with patients being seen by nearly three times as many GPs — a far cry from the mid-1980s when few GPs were involved and fewer still were willing to prescribe.
In the 1985 study, Glanz found that 35% of these patients were new to the doctor.19,20 The fall in the proportion of new patients seen by GPs in 2001 compared to 1985 (down from 35% to 15%) warrants further consideration. An explanation may be that an increase in the overall availability of treatment places since 1985 has reduced the need for opiate misusers to access primary care. It is also possible that while GPs are managing more patients, they may also be retaining them for longer, leaving no room for new patients. The smaller proportion of new patients in the 2001 study should prompt questions about whether there may now be a capacity problem developing with regard to patients trying to access treatment in primary care.
Strengths and limitations of this study
Study limitations need to be recognised. A sample size of 10% was chosen for this study, double that of the previous 1985 study,19,20 and a sampling and stratification process designed to eliminate bias due to multiple response from the same practice and to span single-handed through to large practices was used. However, caution should be exerted when extrapolating numbers of GPs and numbers of patients to the whole population. The response rate also needs to be considered, as studies of this nature have previously indicated that responders are more likely to be those who are interested or active in the field of study,35 and thus there is the risk of overestimate of the actual level of activity. Caution is also required in view of the reliance on self-report from GPs, which may result in bias due to error in recall or reporting. In an attempt to reduce any such bias or uncertainty, enquiry focused on activity in the previous 4 weeks, and GPs were encouraged to check recall through patient medical records. The issue of ‘social desirability’ in the responses is less likely to be a major issue as responses reported here are factual, and not attitudinal.
Implications for future policy and practice
The extent of GP activity is encouraging, but some areas of concern must also be recorded. We found widespread prescribing of methadone at low dose — certainly low in comparison to the international literature. The mean daily dose of methadone prescribed by GPs was 36.9 mg, with the modal value being 30 mg daily, and with nearly 50% of methadone prescriptions being for a daily dose of 30 mg or less. This is low dose (for opiate-dependence treatment) and is not in keeping with international evidence of greater benefit from higher-dose oral methadone maintenance.36-38 Various possible explanations for these low doses can be put forward: for some patients, the doses may originally have been higher but they may now be on a reducing path; the greater willingness of GPs to treat opiate misusers may have encouraged a larger number of opiate-dependent patients to seek treatment, perhaps with lighter dependence-problems. However, if these doses are meant to be methadone maintenance treatment, then they indicate a disturbingly widespread reliance on low-dose maintenance treatment, which has been found to be significantly less effective than high-dose maintenance.36 It is also possible that GPs are exercising increased caution about opioid prescribing following the growing concern about diversion of prescribed supplies of methadone and their contribution to overdose deaths among young people.39-42 However, even if such pressures may be understandable, the provision of suboptimal treatment is not defensible.
A second area of potential concern is the extensive provision of take-home supplies of methadone. Nearly half (42.9%) of all methadone prescriptions were being issued as a single dispensing of at least a week's supply, despite the existence of special regulations that permit GPs in the UK to instruct the dispensing pharmacist to supply the methadone in smaller installments (such as on a daily basis for a prescription covering a fortnight). In recent years, the Department of Health17,18 has guided that there should be more extensive supervision of methadone consumption (as already occurs in some cities such as Glasgow),5,43 or at least daily dispensing of each installment. Unless a more stable population is being managed by GPs (about which we have no data), the evidence from the current survey indicates that this guidance (about daily dispensing) has gone largely unheeded.
The UK government has strongly embraced the management of drug misusers in primary care with the development of shared care models,7-12,16 as a pragmatic solution to an ever-increasing demand for services. However, despite this move, demand continues to outstrip availability of services in many areas. Doubts and worries persist,14,15,30 and this study provides us with both encouraging and disappointing news. On the positive side, the majority of GPs were willing to be involved in providing care to drug misusers, with evidence of a considerable degree of further untapped willingness. But on the negative side, 36% still stated that caring for opiate misusers was not part of the work of their practice, and, of those who had not seen any opiate misusers in the previous 4 weeks, 22% were not willing to treat opiate misusers. It seems that two different conclusions can be reached. Firstly, that with appropriate support and funding, some of the remaining ‘dormant’ GPs might be stimulated into involvement. Secondly, despite more than a decade of active promotion of the vital contribution of the GP, there remains a substantial minority who remain opposed to such involvement. Enthusiasm for advancement on the positive front must be accompanied by serious attention to deficiencies in comprehensive coverage, if prompt access to appropriate health care at time of need is accepted as the proper objective.
The involvement of GPs in the management of opiate addiction (office-based practice) is being considered and implemented by several other countries, including Australia, France, Germany, and the US.22-29 We have charted the substantially increased contribution of GPs, and this is to be encouraged in the changing NHS.1-4 However, it will be crucial for this to be accompanied by specific attention to the training needs of these GPs34 and to the dissemination of guidance to promote the best (and avoid the worst) of clinical practice in the management of the opiate misuse.
Acknowledgments
We thank all GPs who completed the questionnaires
Notes
Funding body
Research grant awarded by the charity Action on Addiction, and subsequent supplementary funding from Department of Health
Ethics committee
South London and Maudsley NHS Trust Ethics Committee
Competing interests
None
- Received August 13, 2004.
- Revision received December 1, 2004.
- Accepted April 9, 2005.
- © British Journal of General Practice, 2005.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

