


Abstract
Background Hypertension is generally poorly controlled in primary care. One possible intervention for improving control is the harnessing of patient expertise through education and encouragement to challenge their care.
Aim To determine whether encouraging patients to manage their hypertension in an ‘expert’ manner, by providing them with information in a clear clinical guideline, coupled with an explicit exhortation to become involved in and to challenge their own care if appropriate, would improve their care.
Design of study Single blind randomised controlled trial of detailed guideline versus standard information.
Setting Single urban general practice over 1 year.
Method Patient-held guideline with written explicit exhortation to challenge care when appropriate. Two hundred and ninety-four of 536 eligible patients on the practice hypertension register were recruited, all of whom were randomised into one of two groups. Two hundred and thirty-six patients completed the study.
Results Primary outcome: average systolic blood pressure. Secondary outcomes: proportion of patients with blood pressure <150mmHg systolic and <90mmHg diastolic, average cholesterol, proportion of patients prescribed statins and aspirin according to guideline, hospital anxiety and depression score. No clinically, or statistically significant differences were found between intervention and control with respect to all parameters or in anxiety and depression levels. Statin and aspirin use improved throughout the course of the study in both groups. Statin use showed a trend (P = 0.02) in favour of control.
Conclusion In this study there was no clinically significant perceived benefit to patients as a result of providing them with a hypertension guideline. Patient guidelines are currently planned for many chronic illnesses. It is important to determine the utility of such interventions before scarce resources are applied to them.
INTRODUCTION
There is sound evidence that control of hypertension can significantly reduce the incidence of stroke and cardiac events.1 National guidelines for the identification and treatment of hypertension have been issued.2,3 However, there is evidence that most patients with hypertension who are identified do not have their hypertension adequately controlled,4,5 and that GPs often overestimate their adherence to guidelines.6
Without additional interventions to encourage change in medical practice, the effects of clinical guidelines are generally limited.7,8 A large number of additional interventions have been used to encourage the adoption of clinical guidelines including continuing medical education, dissemination of educational materials, educational outreach, local opinion leaders, audit and feedback, manual or computerised reminders, mass media campaigns and continuous quality improvement programmes.9 All have some effect, but none are overwhelmingly successful or effective in all circumstances.9,10 It is suggested that multiple interventions may be more effective than single ones.11,12
Clinicians have become increasingly aware of the impact of using patients' own expertise in the management of chronic illness and encouraging the ‘expert patient’ is UK government policy.13 In addition, there is increasing evidence that, in primary care, patients' expectations have a significant effect on the treatment they get from their doctor.14,15 Additionally, a variety of interventions aimed at improving adherence to antihypertensive medications have been evaluated with modest success, but patient education alone appeared unsuccessful.16
How this fits in
Patient-held guidelines are being increasingly employed to enhance patient care, however, there is little evidence for their effectiveness. This study shows that a patient-held guideline on hypertension, with an explicit exhortation to patients to challenge their care if it did not comply with the guideline, did not lower blood pressure. Reassuringly, however, the provision of such information did not increase anxiety.
One initiative, which has not been fully evaluated, is distribution of guidelines to patients although there is some evidence for their use in chronic illness.17,18 The purpose of our study was to evaluate the effect on the overall management and control of hypertension of encouraging patients to behave in an ‘expert’ manner by providing them with the necessary information in a clear clinical guideline, coupled with an explicit exhortation written in the guideline from their medical team to become involved in and to challenge their own care if appropriate. Because it was considered that providing such frank information including ten-year coronary heart disease risk might create anxiety, we included a measure of the psychological impact of the guideline.
We hypothesised that such an intervention would, after one year, lead to an increased number of patients with controlled (systolic/diastolic <150/90) blood pressure, lower average systolic blood pressure, lower cholesterol level, and achieve a greater adherence to national guidelines in the use of aspirin and statins with no concomitant change in anxiety and depression levels.
METHOD
Participants
We identified patients from the hypertension register of the participating health centre, a medium sized family practice containing 5500 patients in a relatively deprived part of Scotland. All patients on the register older than 18 years who had at least one systolic blood pressure recorded >150 mmHg were sent a description of the project and its aims and invited to take part in the study. We began recruitment in 2002. Non-responders were sent a reminder.
Randomisation
Randomisation and allocation was carried out remotely from the practice and independently using computerised random number generation. Where random number generation produced different interventions for two patients living at the same address, the female patient's intervention was changed to that of the male (n = 9). This was to minimise cross-contamination of control patients. (There were no instances of two hypertensive males or females at the same address).
Intervention
Those who agreed to take part were randomised into two groups. The first received, by post, a standard information booklet from the British Hypertension Society (BHS), the second the BHS booklet and additionally a detailed guideline (Supplementary Appendix 1) and record card derived from the Lothian Hypertension Guideline which gave general information about blood pressure, but also provided the patient with clear guidelines as to how their blood pressure should be managed by medical and nursing staff, and a clear exhortation to question their care if the guideline was not being adhered to. The guideline provided clear targets for blood pressure control, indicated the importance of calculating coronary heart disease risk where appropriate and the circumstances in which aspirin and statins should be used and cholesterol targets. The intervention was limited to the distribution of the guideline. Clinical staff members in the practice were fully informed of its content and were told to make use of it if patients took it with them to consultations. However, there was no follow-up mailing or telephone intervention to reinforce its use.
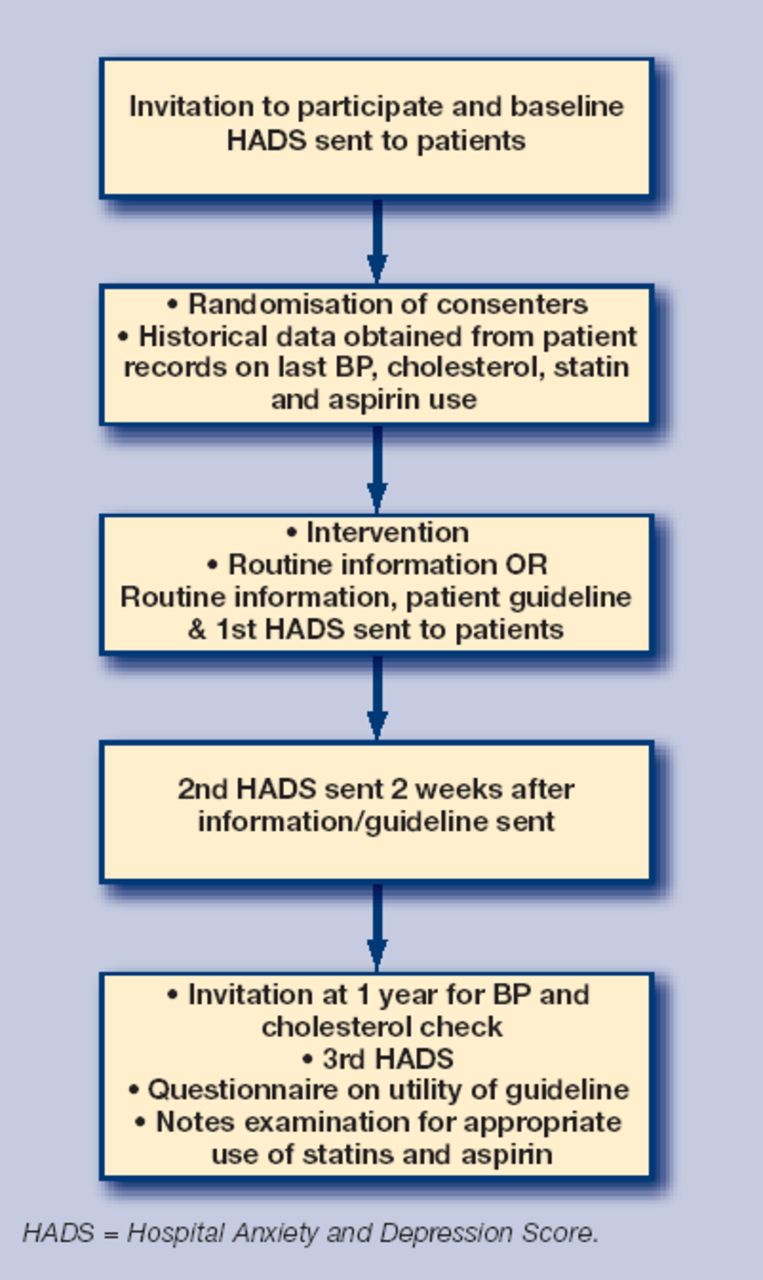
Study flow chart.
The guideline during development and prior to distribution was reviewed by patients and by professionals and found to be simple to understand and to address the important aspects of blood pressure management.
Outcomes
The primary outcome was the proportion of patients whose blood pressures were ‘controlled’ defined as systolic blood pressure <150 mmHg and diastolic <90 mmHg. Secondary outcomes included; average systolic blood pressure, average cholesterol, proportion of patients prescribed statins and aspirin according to guideline, hospital anxiety and depression score at 2 weeks and 1 year.
Data collection
Baseline data collection
All these baseline data were derived from patient records except for the Hospital Anxiety and Depression Score (HADS) that were obtained at the time of first contact with the patient. We decided to use historical data on the practice computer system rather than measure all participants' parameters at baseline as we thought that doing so, with its consequent impact on management, would greatly blur any possible effect of the intervention.
Measurement of anxiety and depression
With the invitation to take part, patients were asked to complete a baseline HADS questionnaire. We chose this as it is a well validated scale19 with good test/retest reliability and is suitable for patients who may have cardiovascular problems. Patients were subsequently asked to complete the HADS questionnaire by post, at 2 weeks and 1 year after the intervention.
Measurement of blood pressure at 1 year
Patients in the trial were invited after 1 year to attend for blood pressure measurement. The nurses measuring blood pressure were blind to the patients' trial allocation. It was the intention to measure all patients using an electronic sphygmomanometer (OMRON HEM-97) twice, with patients seated and an average taken. However, a small subset (n = 33 [14%], 15 in control and 18 in intervention groups) had a single measurement of blood pressure using a mercury sphygmomanometer.
Blinding
At the time of taking the blood pressure the nurses were blind to the status of the patients. However, in a very small number of cases (n = 3) patients revealed which group they were in by presenting the nurse with the record card which comprised part of the patient-held guideline.
Measurement of cholesterol at 1 year
Any patient who had not had a cholesterol estimation performed in the preceding 6 weeks had blood taken for this. Cholesterol was measured by the local hospital laboratory.
Use of statins and aspirins at 1 year
The research nurse, blind to patient randomisation, examined participants prescribing records for evidence of aspirin and statin use. Appropriate aspirin and statin use was determined by 10-year CHD risk estimation (calculated using the Joint British Societies Cardiac Risk Assessor Program based on equations devised by Anderson et al20 <15% no treatment; ≥15% but <30% aspirin if not contraindicated; ≥30% aspirin and statin if not contraindicated using presenting blood pressure).
Patient perception of the intervention and control
Patients were sent a questionnaire shortly after the end of the trial asking them their views on how well they thought the practice had looked after their blood pressure, how much they felt involved in the management of the blood pressure, and how useful they found the written material they had been sent.
Recruitment
Recruitment started in spring 2002 over a 2-week period. Along with the invitation to take part, patients were sent a baseline HADS questionnaire. Patients who agreed to take part were sent either the intervention and control information or control information alone. Two weeks later they were sent the second HADS questionnaire. Follow up for BP and cholesterol measurement took place over a 6-week period 1 year later.
Sample size
Based on existing baseline data from the patient records we calculated that a study that recruited 300 patients would have had 80% power to detect as significant at the 5% level differences between groups of 15% of patients achieving blood pressure <150/90 and in mean blood pressure of more than 5 mmHg.
Statistical analysis
Analysis was by intention to treat. Treatment groups were compared by two-sample t-tests for quantitative outcomes and χ2 tests with Yates' correction for categorised outcomes. Confidence limits for differences in percentages were calculated using the Wilson method. Changes in measurements from baseline to end of study were tested by paired t or McNemar tests as appropriate.
RESULTS
Figure 2 shows the flow diagram of how the recruitment and randomisation proceeded. Of eligible patients, 294 of 536 were recruited, all of whom were randomised. Two hundred and sixty-one presented for final blood pressure estimation, 238 provided a final HADS score and 244 provided a final cholesterol level.

{kind=link}
{kind=link}
Participant flow chart.
Baseline data
The data collected at baseline (Table 1) shows that there was no significant difference between the characteristics of control and intervention groups at baseline.
Comparison of randomised groups at baseline.
Endpoints
At the end of the trial there was no clinically or statistically significant difference between the intervention and control groups with regard to any of the parameters except a trend for the use of statins (P = 0.02 in favour of control group). Table 2 shows the differences between the groups with regard to the different parameters.
Comparison of randomised groups at end of study.
Change of HADS throughout the study
There was a trend towards a small, but clinically significant, drop in the average anxiety component from 7.75 to 7.24 (P = 0.02) and a statistically significant drop in the depression component from 5.87 to 4.9 (P = 0.001) of the HADS between the start of the study and 2 weeks after intervention in the intervention group with a corresponding trend in the depression component of the control group of 6.0 to 5.46 (P = 0.06). There was, however, no statistically significant difference between the control and intervention group in the change in either HADS scores either at 2 weeks or the end of the study.
Changes in average cholesterol, numbers treated with statins and aspirin during the course of the study
There was a significant reduction in both control and intervention groups in terms of average cholesterol (mmol/l) over the year (5.48 to 5.02, P = 0.001 and 5.42 to 5.04, P = 0.002 respectively) although the difference between the two groups was insignificant. More patients were treated with statins over the course of the year in both groups, but significantly more in the control group (P = 0.01, see Table 2).
There was a small but statistically significant increase (P = 0.008) in the numbers treated with aspirin over the year but no difference between intervention and control groups.
Patient perceptions of the effect of the intervention
At the end of the study patients were sent a questionnaire asking them their views on how well they thought the practice had managed their blood pressure over the year (very well; quite well; not so well; not at all well), how much the staff had involved them in managing their blood pressure (yes, a lot; yes, a little; not at all) and how useful they had found the information they had been sent (very; quite; not so useful; not at all useful). There was no difference between the groups in their perception of how well their blood pressure had been managed, or in the usefulness of the literature. Those in the intervention group who replied were numerically more likely to say they had been involved ‘a lot’ in their blood pressure management, but this failed to reach statistical significance (65/78 (83%) versus 57/81 (70%), difference = 13%; 95% confidence interval = 0 to 26).
DISCUSSION
Summary of main findings
The results of this study suggest that the use of this particular patient-held guideline did not improve clinical outcomes in respect of the management of hypertension when compared with standard information. Interestingly, there was a trend toward a small, but clinically significant reduction of anxiety and depression scores following the distribution of both the guideline and control documentation, a phenomenon suggested by previous research.21 This provides some further reassurance that presenting patients with detailed cardiovascular risk information does not appear to cause distress. One parameter, the appropriate use of statins based on cardiovascular risk, was possibly better managed in the control group. It is hard to know why this may be so, although it was a secondary end-point and may be artefactual given the multiple parameters being tested.
Overall throughout the year there was a significant increase in the use of statins, aspirin and the proportion of patients whose cholesterol was controlled in both groups. We were unable to draw rigorous conclusions as to how much blood pressure control had changed, as baseline blood pressure was based on historical records. However, there appeared to be little change over the year.
Strengths and weaknesses of the study
This was a pragmatic trial carried out in a normal UK health care setting of an intervention which would be inexpensive to apply. We deliberately chose to distribute the guideline in a way that we felt it would probably be distributed in normal clinical settings. However, it may be that more intensive interventions, for example followed up by clinician reminders or combined with home monitoring would have been more effective, as educational interventions alone have not been shown in other studies to be effective.16 Equally it might be argued that there was a ceiling effect and that blood pressure control in this group would have been hard to improve. However, following recent changes in the payment system for UK GPs where blood pressure control is specifically rewarded, the frequency of controlled blood pressure in the participating practice has greatly exceeded that sought in the trial.
There was a gratifying uptake of the study from patients who were largely representative of the practice. The practice, however, is derived from patients of lower socioeconomic groups some of whom had literacy problems and this may have had implications for the effectiveness of the guideline and generalisability of the results. The study was initially designed so that the patients would be randomised into groups and then be exposed to the guidelines before being given information and consenting to be part of the study. However, the local research ethics committee asked that all patients be consented at the start of the study. The detailed nature of the study information sheets prompted many patients to contact the surgery prior to randomisation to have their blood pressure and blood checked and to ask about preventative drug therapy. This may have reduced the subsequent effect of the guideline. Also, in common with many practices in the UK, improved computer software became available during the course of the year. The new software had features which automatically calculated 10-year coronary risk and could prompt doctors to check blood pressure and warn if patients with ischaemic heart disease were not appropriately treated with statin or aspirin. Additionally the guideline may have influenced doctors' management of hypertension generally and not just for those randomised to the intervention group.
As a result of a misunderstanding of the protocol by one nurse all patients did not, as had been intended, have their blood pressure taken electronically. This almost certainly led to a less rigorous measurement for this small group. However, this problem applied equally to patients in both groups and to less than 15% of the participants in total and removal of these patients from the analysis did not alter the results.
Comparison with other existing literature
Patient-held guidelines have been successfully used in asthma,18 but a New Zealand ‘self-empowerment and educational device for people with diabetes’ was found to be ineffective,22 although there is evidence for more intensive interventions in this field.23 We found no other trials of patient-held guidelines in hypertension.
Encouraging the ‘expert patient’ is UK government policy,13 detailed patient guidelines have been distributed in other countries24 and there have been discussions in the UK about providing patient guidelines based on SIGN (Scottish Intercollegiate Guidelines Network) for a variety of conditions. Before this happens, however, it is important that our study is replicated on a larger scale and with differing types of practice to see if the findings in this study are typical.
Ideally, future research in blood pressure or other sorts of patient-held guidelines should be in the form of a cluster randomised controlled trial in a variety of practices drawn from differing socioeconomic groups. Such a trial would be enhanced by a design where control consent is obtained after randomisation and one which included a health economics component. In the current UK climate, where maximisation of blood pressure control is heavily incentivised by financial reward, it is unlikely that patient guidelines would have a measurable effect.
Supplementary Material
Acknowledgments
We are grateful to the patients, doctors and nurses of Ashgrove HC who took part in the trial and to Aziz Sheikh for help with drafting the paper. Brian McKinstry is a career fellow funded by the Chief Scientist Office of the Scottish Executive.
Notes
Supplementary information
Additional information accompanies this article at http://www.rcgp.org.uk/bjgp-suppinfo
Funding body
Chief Scientist Office of the Scottish Executive (OOB/3/19/F25)
Ethics committee
Lothian Research Ethics Committee (LREC/2001/1/21)
Competing interests
The authors have stated that there are none
- Received October 2, 2005.
- Revision received January 27, 2006.
- Accepted May 2, 2006.
- © British Journal of General Practice, 2006.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

