


Abstract
Background B-type natriuretic peptide (BNP) is a blood test which detects ventricular wall stretch and is being increasingly used in primary care on limited evidence.
Aim To assess the practical implications and potential clinical benefit of measuring BNP to identify and guide the treatment of undiagnosed or under-treated ventricular dysfunction in at-risk patients.
Design of study Screening study with single-arm intervention.
Setting A total of 1918 patients with diabetes mellitus or ischaemic heart disease aged ≥65 years registered with 12 general practices were invited; 76 patients with elevated BNP underwent BNP-guided treatment titration.
Method Eligible patients were invited to attend for a blood test at their own practice; those with a persistently elevated plasma BNP concentration (>43.3 pmol/l) after repeat measurement were offered initiation or up-titration of treatment guided by remeasurement of BNP with a target concentration of <36 pmol/l.
Results Seven-hundred and fifty-nine patients (40%) attended for screening; 76 (10% of 759) commenced treatment titration. Of these 76 patients, 64 (84%) were asymptomatic or had only mild breathlessness. Maximum titration effect was achieved by the second visit when 27 (36%) had achieved the BNP target concentration and the mean reduction was 10.8 pmol/l (P<0.001). The most effective therapeutic step was a switch in beta-blocker to carvedilol or bisoprolol (P<0.001).
Conclusion About 10% of patients with diabetes or cardiovascular disease on GP morbidity registers have a persistently raised plasma BNP concentration. Simple adjustment of their drug treatment may reduce their BNP and associated mortality risk, but further up-titration against BNP is only possible if the within-person biological variability of measurement can be reduced.
INTRODUCTION
Plasma B-type natriuretic peptide (BNP) is a measure of ventricular function — it is released into the bloodstream as the ventricular wall is stretched. Initially its diagnostic performance in detecting ventricular dysfunction was reported using echocardiography as the gold standard.1 It is now evident that BNP is in some ways a better diagnostic gold standard than echocardiography. It is a strong predictor of death from cardiac disease irrespective of whether an echocardiographic diagnosis of ventricular dysfunction or a clinical diagnosis of heart failure has been made. In patients with symptoms of heart failure, every 29 pmol/l (100 pg/ml) increase in BNP concentration is associated with a 35% increase in relative risk of death.2 In asymptomatic patients there are insufficient data to provide a similar estimate, but the relative risk of death is doubled (estimated hazard ratio 2.2) even above the low BNP cut-off of 5 pmol/l (18 pg/ml) applied in the MONICA (MONItoring of trends and determinants in Cardiovascular disease) study.3
How this fits in
Plasma B-type natriuretic peptide (BNP) is a measure of ventricular function which predicts risk of death from heart failure. Measurement of BNP is a cost-effective way to diagnose acute heart failure in a hospital setting and to guide its subsequent treatment. This study shows that it is also feasible to use the test in general practice to identify patients with raised BNP, and to reduce their mortality risk by simple adjustment of their drug treatment, whether or not they have overt symptoms of heart failure. However, using BNP to guide titration of subsequent treatment is not straightforward because of the within-person biological variability of a single measurement, which can be of similar size to the change achieved by adjusting treatment in patients who do not have acute symptomatic heart failure.
Echocardiography is still diagnostically important for investigating the cause and nature of ventricular dysfunction. However, evidence is accumulating that measuring BNP without undertaking echocardiography is clinically useful in a hospital setting in improving the diagnostic performance of non-specialist physicians,4–6 reflecting the fact that low plasma BNP concentrations rule out symptomatic heart failure.7 It has also been used successfully in hospital settings to monitor and titrate treatment.8–10 In the light of these reports, many NHS primary care trusts (PCTs) in the UK (110 out of 211 responders) now plan to support open access to BNP measurement in primary care.
This enthusiasm for BNP in primary care is understandable. Ventricular dysfunction is common among older patients in primary care,11,12 and access to echocardiography is often difficult. Measurement of blood BNP appears a simple and effective way to detect both systolic and diastolic dysfunction.13,14 Echocardiography remains important for identifying cardiac valve lesions in patients with elevated BNP concentrations, but it is about six times more expensive than a BNP assay, provision is usually hospital based and often limited, and a blood test is much easier and more convenient for the primary care patient. A good case can therefore be made for using plasma BNP as the diagnostic and monitoring test of choice in primary care.
Although this case has some merit, the evidence base to support it is still incomplete. A recent meta-analysis concluded that ‘the effect of the introduction of tests on clinical outcome or costs remains unclear’.15 The uncertainty stems from two main issues. Firstly, BNP shows as much variability as blood pressure, so that making a diagnostic or treatment decision on a single reading may be difficult in the non-acute situation.16 Secondly, the entry criterion for trials showing the benefit of angiotensin inhibition and beta-blockade in treating heart pump failure, whether symptomatic or not, has been ventricular dysfunction defined by echocardiography. Therefore, the effectiveness of treating ‘hyperBNPaemia’ without echocardiographic evidence of ventricular dysfunction is arguably unproven. This paper therefore reports the results of an observational study to assess the practical implications and potential clinical benefit of using plasma BNP to detect unrecognised or undertreated ventricular dysfunction in at-risk patients in general practice, and to guide their subsequent treatment.
METHOD
Identification and recruitment of subjects
Twelve primary care practices participated — four in Greater Birmingham and eight in or around Oxford. The practices were selected to represent a range of urban, semi-urban, and rural environments in the UK. All practices maintained electronic updated registers of patients with chronic disease, and each participating practice invited all patients aged ≥65 years registered with a diagnosis of either ischaemic heart disease or diabetes mellitus (which should include virtually all patients at risk of heart failure) to participate in the study. A total of 1918 patients were invited to participate between June 2004 and August 2005.
Initial screening for raised natriuretic peptide
A 4 ml sample of venous blood was drawn into a standard EDTA collection tube and transported to the laboratory the same day, usually within 4 hours. Samples were stored at 2–8°C before same-day centrifugation; storage of plasma after centrifugation was at −70°C. The initial screening assay was done in the local laboratory by measuring either BNP (607 patients) applying a cut-off of >43.3 pmol/l (150 pg/ml), or NTproBNP (152 patients) applying a cut-off of >26.2 pmol/l (220 pg/ml). Patients with natriuretic peptide concentrations above these cutoffs were invited to attend for further investigation, including two further blood tests for plasma BNP measurement (applying the quality control procedures described below), and a clinical examination.
Further investigation
The clinical examination was conducted by a GP or trained research nurse. Blood was taken for repeat measurement of BNP and for baseline measurement of serum creatinine and electrolytes on two separate visits. BNP assays were measured using the Bayer fully automated immunometric assay with chemiluminescent detection (Diagnostics Division, Bayer HealthCare, Newbury, Berkshire; now Siemens Medical Solutions, Frimley, Surrey). The inlaboratory coefficient of variation of the BNP assay has been estimated as <3.5%;17 the laboratory precision estimated from the quality control procedures was between 4.9% and 6%. Respiratory function was assessed by spirometry, and heart failure symptoms were recorded using the New York Heart Association (NYHA) classification.18 Echocardiography was conducted (by an echocardiography technician or GP with a special interest in cardiology) primarily to exclude serious valve lesions; systolic function was also assessed, employing Simpson's bi-planar method to estimate ejection fraction.19
Inclusion and exclusion criteria for titration phase
The inclusion criterion for treatment titration was a plasma BNP >43.3 pmol/l in two blood samples. GPs were advised to exclude patients on four grounds:
valve lesion requiring surgical intervention;
seriously impaired renal or respiratory function;
inability to understand and cooperate with titration of treatment; and
serious comorbidity (such as severe respiratory disease) making titration of treatment inappropriate.
Patients with poorly controlled atrial fibrillation were excluded only until rate control had been achieved; if the BNP remained above the 43.3 pmol/l threshold after rate control, they could be included.
Treatment titration
Patients were offered treatment titration at their general practice surgeries. The recommendation was for adjustment of therapy by the GP on the basis of the BNP result every 2 weeks for a maximum of four visits and then every 4 weeks once it fell within the target range of <36 pmol/l (125 pg/ml) on two successive occasions; or, if this was not achieved, for a maximum of 6 months. The GPs were given a simple titration plan based initially on the introduction and/or up-titration of angiotensin inhibitors then beta-blockers (according to tolerance) up to the British National Formulary maximum recommended daily dose, and finally the introduction of spironolactone if necessary (Appendices 1–5). No specific recommendation was made on which angiotensin-converting enzyme (ACE) inhibitor or angiotensin II receptor blocker (ARB) to prescribe, although GPs were advised to use either carvedilol or bisoprolol as the beta-blocker. Furosemide was suggested only for control of symptoms.
Collection of study data and endpoints
Plasma BNP plus serum creatinine and electrolytes were remeasured at each titration visit; pulse, blood pressure, weight, and any clinical signs or symptoms of heart failure were also recorded. In one surgery, titration was based on use of a near-patient BNP test (done in parallel with the laboratory assay on which the results reported here are based). In other surgeries, blood was taken by a nurse before the consultation so the result was available at the consultation, or adjustment of treatment was left to a subsequent visit or confirmed by telephone after the consultation when the blood result was known. Practitioners were advised to monitor serum creatinine, serum potassium, and blood pressure at each visit, and to stop titration if serum creatinine exceeded 200 μmol/l (or 30% above baseline), serum potassium exceeded 5.5 mmol/l, or they were concerned (on the basis of clinical measurement or history) about the risk of hypotensive events such as faints or falls.
Main outcome and statistical analysis
The agreed main study endpoint for the titration phase was the difference between the blood BNP concentration at entry (mean of the two assays immediately prior to treatment titration) and at study exit (mean of the last two assays done during the 6-month follow-up period). This difference was estimated on the basis of intention to titrate. Statistical analysis was undertaken with the software programmes SPSS (version 14) and STATA (version 8). The comparison of the dichotomous outcomes (for example, differences in the proportion of patients taking treatment) was made by Fisher's exact test; comparison of continuous variables (for example, mean BNP concentrations) was made by a paired t-test. The analysis of the effect of titration of ACE inhibitors and beta-blockers is based on detailed analysis of the first four visits for 61 patients at which treatment adjustments to dosage of these drugs were made. A mixed-effects multiple regression analysis using the patient as an identifier was conducted to assess the effect of adding or adjusting an ACE inhibitor or beta-blocker on the change in BNP concentration at the next visit.
RESULTS
Initial screening
The uptake and outcome of the initial screening is shown in Figure 1. A total of 1918 eligible patients were identified from the diabetes mellitus and ischaemic heart disease registers of the participating practices and invited to attend for venesection. Initial uptake was 40% (95% confidence interval [CI] = 37% to 42%) overall, but higher in Oxfordshire (477/966, 49%) than in Birmingham (282/952, 30%). About one in five patients tested (147/759, 19%) had a raised natriuretic peptide (BNP or NTpro-BNP) on the first test, but 40% (53/132 retested × 2) did not have a persistently raised BNP >43.3 pmol/l on further investigation. Of the 79 patients in whom BNP remained elevated, 76 entered treatment titration. One patient was withdrawn because of mitral stenosis recognised on echo assessment, one because of comorbidity, and the third because of known intolerance to a drug in the titration regime.

Outcome of initial invitation to BNP screening of the 1918 patients on the diabetes and ischaemic heart disease morbidity registers.
Baseline characteristics of patients titrated
The mean age of the 76 patients offered treatment titration was 77 years (range 66–92 years), and the mean entry BNP (the mean of the confirmatory screening sample and the pretreatment sample) was 62.4 pmol/l (range 37.5–144.1 pmol/l). Most patients were either asymptomatic (23, 30%) or had only mild symptoms of heart failure (41, 54%); the remaining 12 patients had more marked symptoms, with a NYHA score of 3. Most patients (49, 65%) were assessed as having neither global nor regional ventricular systolic dysfunction on echocardiography, with only 11 (14%) having an ejection fraction <40%. Table 1 shows that more than one-third of patients (40%) were already receiving the recommended treatment for ventricular dysfunction of both an angiotensin inhibitor and beta-blocker; few (13%) were receiving neither.
Medication prescribed at the beginning and end of BNP-guided treatment titration (n = 76).
Changes in medication made during titration
The mean number of visits made by each patient for assessment and titration of treatment was 8.6 (standard deviation [SD] 2.9) and median 9 (interquartile range [IQR] 7–11). The minimum of visits was five. Table 1 shows that the proportion of patients receiving optimal treatment (that is, both an angiotensin inhibitor and a beta-blocker) increased from 40% to 74%, and the proportion receiving neither treatment fell from 13% to 5%. The most common adjustments made during the first three visits were the introduction or up-titration of angiotensin inhibitors (81 titrations), the introduction or up-titration of a beta-blocker (33 titrations), or a change in beta-blocker (27 switches, in 26 cases a switch to carvedilol or bisoprolol). The decision to switch beta-blockers was region specific: 24 of the 27 switches were in Oxford practices. Introduction of spironolactone was infrequent (five events).
Effect of titration on BNP
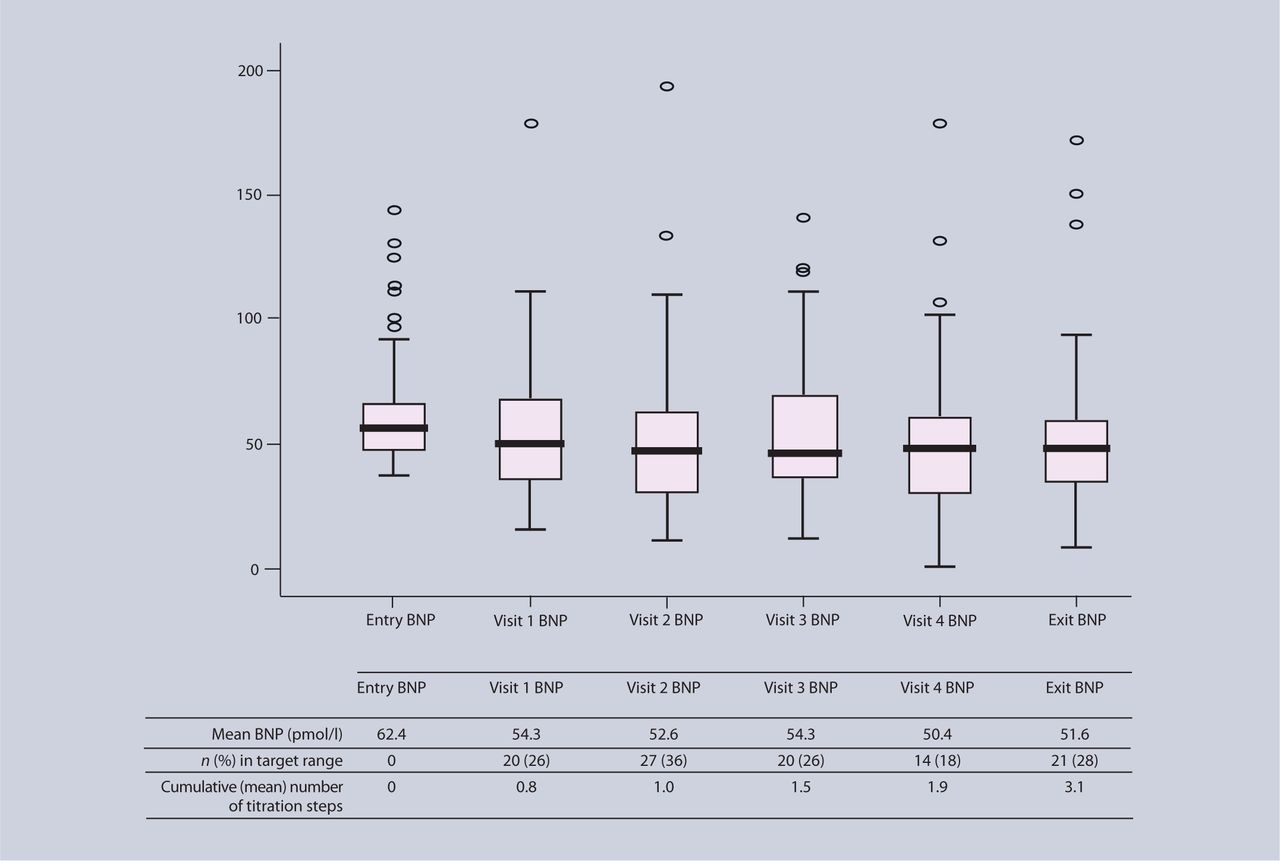
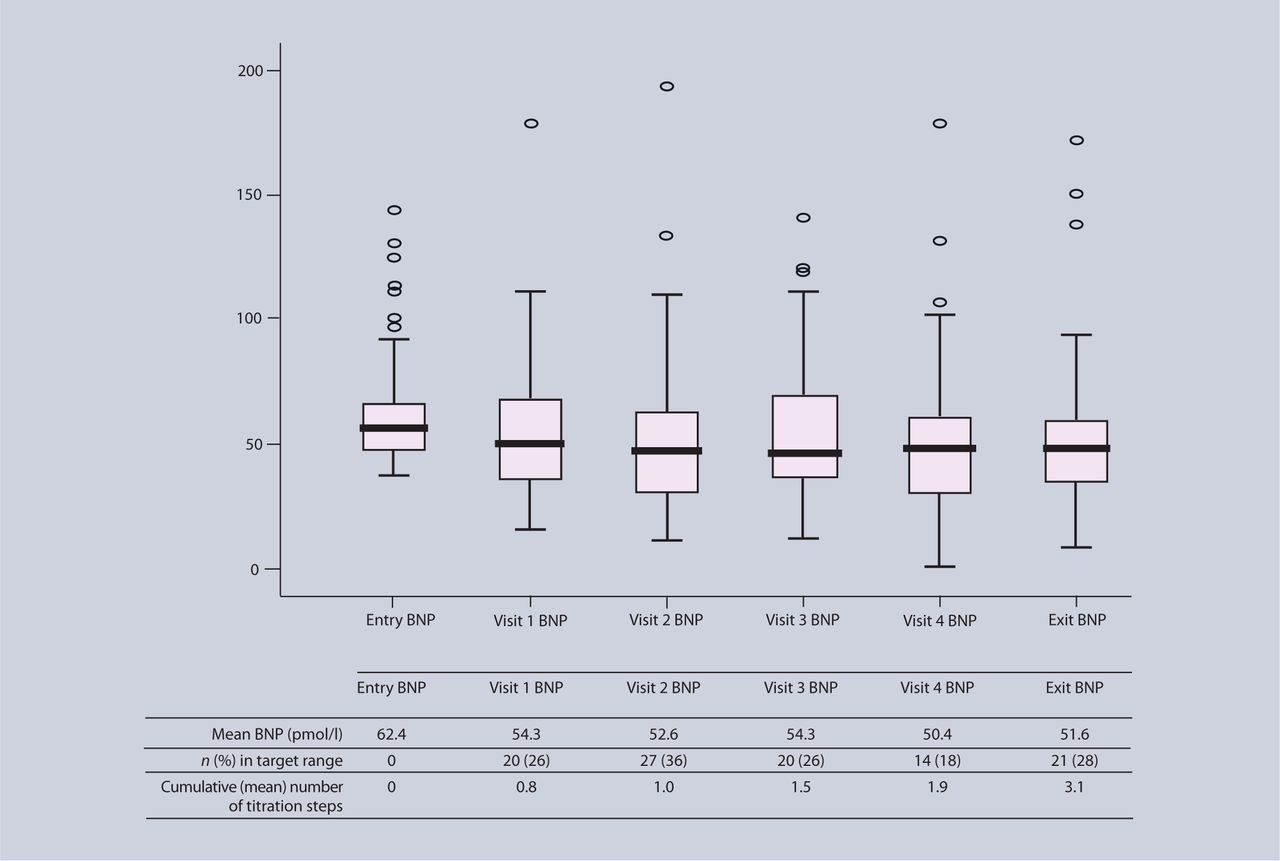
The effect of titration on the BNP concentration is shown in Figure 2. Twenty-one patients (28%) were within the BNP target range (<36 pmol/l) at exit. The mean BNP reduction achieved was 10.8 pmol/l (17%, P<0.001). Most of the reduction achieved was the result of initial modification of treatment rather than continuing titration — the BNP concentration at visit 2 was 52.6 pmol/l, and at exit 51.6 pmol/l.
{kind=link}
{kind=link}
Blood BNP concentrations (pmol/l) at entry (mean of two pre-titration samples), at exit (mean of last two samples), and at first four intermediate titration visits. Data below x axis show mean BNP concentrations and proportion of patients within target range of <36 pmol/l, and mean number of titration steps completed. Line within box is median value; the box represents the interquartile range (50% central range); the whiskers represent 2.5% and 97.5% values (95% central range); circles are extreme values.
The stepwise approach to the mixed-effects regression provided a final model that included both switching to bisoprolol or carvedilol, and introducing or up-titrating the angiotensin inhibitor as significantly associated with reduction in BNP. Switching to bisporolol or carvedilol, in most cases from atenolol, was the most significant titration step in the regression model (β coefficient 20.0, P = 0.001), with the introduction or up-titration of an angiotensin inhibitor having less effect (β coefficient 9.8, P = 0.037). The effect of up-titration of beta-blockers was not statistically significant.
There was a substantial difference in the reduction in BNP achieved by practices clustered around Oxford compared to those around Birmingham. The mean fall in BNP in the Oxford practices was 17 pmol/l compared to 0 pmol/l in the Birmingham practices (P<0.001). This contradicted the prior hypothesis that Oxfordshire practices would perform less well because of higher pretreatment prescribing rates of angiotensin inhibitors and beta-blockers. The multiple regression analysis suggests that the explanation lies in drug titration practice, particularly switching of beta-blockers, as the effect of region (Oxford or Birmingham) on BNP was not significant after adjustment for the titration steps.
Difficulties and adverse effects of treatment titration
Three-quarters of patients starting the titration (57/76, 75.0%) completed it as recommended (that is, until within the BNP target range of <36 pmol/l or 6 months had elapsed), although few complied strictly with the planned 2–4-weekly visit timetable for treatment adjustment. Figure 2 shows that clinicians did not adjust medication at every visit as anticipated by the titration schedule — by the fourth visit the mean number of titration steps made was only 1.9, and by exit 3.1. In eight patients, no change was made in medication at all. In a further 11 patients, titration was interrupted because of new episodes of illness (six patients), or patient unwillingness to continue (five patients). One patient recorded a confirmed potassium concentration >5.5 mmol/l, which required withdrawal of spironolactone. Two patients recorded a creatinine above 200 μmol/l, but only in one case related to uptitration of an ACE inhibitor. Titration was stopped in two patients because of suspected hypotensive episodes; in one episode a patient fell while dismounting their bicycle and fractured a femur; the admitting clinician mentioned hypotension in the discharge summary as a possible precipitating cause.
DISCUSSION
Summary of main findings
The results of this study show that about 10% of patients with diabetes or cardiovascular disease on general practice morbidity registers have a persistently raised plasma BNP concentration. Simple adjustment of their drug treatment has the potential to reduce their BNP concentration and associated mortality risk significantly. Although only one-quarter of the patients treated (28%) had a plasma concentration within the target range after treatment titration, the mean reduction achieved is associated with a 13% fall in relative mortality.2 The estimated workload for the average practice of 6000 patients in setting up an annual BNP monitoring programme for at-risk patients would not be unmanageable; each month it might involve sending invitations to about 10 patients, taking blood from five patients, following up one patient, and adjusting treatment for one patient every 2 months. However, up-titration of treatment against BNP concentration was particularly difficult and time consuming, both because of the elderly patient group and the intra-person variability of the BNP concentration, and it appears to achieve little additional reduction in BNP concentration.
Strengths and limitations of the study
The strength of the study is that it reports the experience of managing older patients, most with significant comorbidity, in real-life NHS general practices. Treatment titration in particular was not straightforward. To some extent this reflects an understandable reluctance of older patients to modify their medication or risk symptoms of hypotension (one patient did indeed fall and break his hip during up-titration of an angiotensin inhibitor, possibly due to hypotension). Clinicians themselves reported that up-titration of treatment was particularly difficult because of the substantial within-person variation in BNP concentrations. This presumably reflects changing ventricular load in response to day-to-day changes in fluid intake, salt intake, and exercise. However, the pragmatic nature of the study, which revealed the difficulty of treatment titration in clinical practice is also its main weakness. The failure to fully implement the titration means that it is impossible to know whether the failure of most patients to reach target despite treatment adjustment reflects irreversibility of the underlying condition, or suboptimal treatment titration (for example, very few patients were prescribed spironolactone). It should also be stressed that despite its scale and logistic difficulty, this was an observational pilot study to estimate effect size, and not a randomised trial. The estimate of effect must remain uncertain until a randomised trial has been conducted.
Comparison with existing literature
The only previous studies estimating the effect of treatment titration against BNP concentrations have been carried out in a hospital setting.8–10 They differ from this study in enrolling symptomatic patients with more severe heart failure, who have substantially higher BNP concentrations at entry. This means that the problem of intra-person variability is much less because the signal-to-noise ratio of the BNP assay is much greater. Unfortunately, this high intra-individual variation and hence low signal-to-noise ratio in the range of BNP concentrations recorded in a general practice population (most with well-controlled symptoms) appears to be common to all natriuretic peptide assays including NTpro-BNP.20 Even in stable hospital outpatients, the reference change value is reported as 43%.21 However, it may be possible to reduce the within-person variability by focusing on the conditions under which the measurement is made.20
The cut-off points for entry to the study were guided by data from the ECHOES (EChocardiographic Heart Of England Screening) study, but were essentially arbitrary and chosen to identify patients in the top quintile of risk.13 The meta-analysis by Doust concluded that the risk of death and cardiovascular events seems to rise even with relatively small rises in BNP well below recommended concentrations for diagnosing echocardiographic ventricular dysfunction in a community setting.2 However, the target of 36 pmol/l was the concentration in the ECHOES study that achieved a sensitivity and negative predictive value of 100% in diagnosing symptomatic heart failure.22
Implications for future research and clinical practice
The present findings have three important clinical implications for a primary care community keen to embrace BNP. Firstly, clinical decisions should not be based on the results of a single assay unless the within-person biological variability of measurement can be reduced. Secondly, a substantial proportion of patients at known risk of heart failure have unrecognised or undertreated ventricular dysfunction which could be monitored and detected by BNP. Thirdly, simple adjustment of their drug treatment, including switching of beta-blockers, has the potential to reduce the BNP and associated mortality risk in up to half the patients so identified. However, this was an uncontrolled study and the results make a formal pragmatic trial to confirm cost-effectiveness more, rather than less, necessary.
Acknowledgments
The authors would like to acknowledge and thank the NHS patients and colleagues who participated in this study. The two University Departments involved in this study are members of the NIHR School for Primary Care Research. With thanks to the study's participants: C A'Court, Broadshires Health Centre, Carterton, Oxfordshire; S Blake, White House Surgery, Chipping Norton, Oxfordshire; D Ebbes and I Southwood, Didcot Health Centre, Didcot, Oxfordshire; P Glasziou, 19 Beaumont St, Oxford; P Grimwade, Windrush Health Centre, Witney, Oxfordshire; A Hussain, Pearl Medical Centre, Ward End, Birmingham; P Jhittay, 273 Kingsbury Rd, Erdington, Birmingham; R Lehman, Hightown Surgery, Banbury, Oxfordshire; D Mant, South Oxford Health Centre, Oxford; R Pankhania, Harlequin surgery, Shard End, Birmingham; J Shribman, Bugbrooke Medical Practice, Bugbrooke, Northamptonshire; F Sohail, Swan Medical centre, South Yardley, Birmingham; T James (Oxford), S Barber (Birmingham); H Becher, J Dwight, D Ebbes, P Grimwade (Oxford); R Davis, A Stein (Birmingham).
Appendices
Recommended titration schedule.
ACE inhibitor equivalence tables for dosing.
Angiotensin II receptor blocker equivalence tables for dosing.
Beta-blocker equivalence tables for dosing.
Notes on dosing.
Notes
Funding body
The study was funded by the UK Medical Research Council (reference is G0300457). NHS service support costs were provided through the Thames Valley Primary Care NHS Trusts Research Partnership. Bayer HealthCare provided the materials for the BNP assay and their technical advice at no cost
Ethical approval
Ethical approval was given by the Central Oxford Research Ethics Committee (REC-C 04/Q1606/60)
Competing interests
Christopher Price is a past employee of Bayer HealthCare. FD Richard Hobbs and David Mant were funded by Bayer HealthCare to present the results of this study at the 2006 World Cardiology Conference. The authors are not aware of other competing interests
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received August 28, 2007.
- Revision received September 4, 2007.
- Accepted January 23, 2008.
- © British Journal of General Practice, 2008.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

