


Abstract
Background Primary care services are often the main healthcare service for people with dementia; as such, good-quality care at this level is important.
Aim To measure the quality of care provided to people with dementia in general practice using routinely collected data, and to explore associated patient and practice factors.
Design and setting Observational, cross-sectional review of medical records from general practices (n = 52) in five primary care trusts.
Method A total of 994 people with dementia were identified from dementia registers. An unweighted quality-of-care score was constructed using information collected in the annual dementia review, together with pharmacological management of cognitive and non-cognitive symptoms. Multilevel modelling was carried out to identify factors associated with quality-of-care scores.
Results In total, 599 out of 745 (80%) patients with dementia had received an annual dementia review; however, a social care review or discussion with carers was evident in just 305 (51%) and 367 (61%) of those 599 cases, respectively. Despite high prevalence of vascular disease, over a quarter (n = 259, 26%) of all patients with dementia were prescribed antipsychotics; only 57% (n = 148) of these had undergone medication review in the previous 6 months. Those with vascular dementia who were registered with single-handed practices received poorer quality of care than those registered with practices that had more than one GP.
Conclusion Although the number of people with dementia with a record of an annual dementia review is high, the quality of these reviews is suboptimal. The quality score developed in this study could be used as one source of data to identify weaknesses in practice activity that need to be corrected, and so would be of value to commissioners and regulators, as well as practices themselves.
INTRODUCTION
Caring for people with dementia requires a holistic approach, including the management of cognitive symptoms, behavioural and psychological symptoms of dementia (BPSD), the provision of necessary social care, communication, and addressing carers’ needs.1 High-quality care, including regular monitoring and appropriate symptomatic treatment, is essential to maintain quality of life for individuals with dementia.2 For example, treatment of BPSD with antipsychotic medication is linked to a greater risk of stroke with associated negative outcomes for people with dementia;3,4 in spite of this, quality of care has been found to be suboptimal in several areas, including low detection rates for dementia,5 inappropriate management of BPSD,6,7 and under-recognition and diagnosis of depression.8
Primary care services are the first point of contact and main healthcare service for people with dementia.9-11 In 2006, the annual dementia review was first introduced as a quality indicator to the UK Quality and Outcomes Framework (QOF) pay-for-performance guidelines for general practice.12 This review, along with an indicator relating to a register of all people diagnosed with dementia in each practice, requires that there is a record of an annual dementia review from the previous 15 months for all patients on the dementia register. It covers an appropriate physical and mental health review for each patient, and coordination with secondary care services, if applicable, as well as the impact on any carer(s) and any carer’s needs for information. The evidence base for a dementia review in the QOF guidance includes evidence from the National Institute for Health and Clinical Excellence and Scottish Intercollegiate Guideline Network guidelines, the Audit Commission, and published papers.12 Two QOF indicators on depression were also included, in relation to case finding for depression, and severity where applicable, as part of an augmented focus of the dementia mental health review. To the authors’ knowledge, there have been no studies that have evaluated the quality of dementia care, as covered by the QOF dementia indicators, to date.
The aim was to measure the quality of care provided to people with dementia in general practices using routinely collected data, including the annual dementia review and the management of cognitive, behavioural, and psychological symptoms. The patient and practice factors associated with the overall quality of care were also explored.
How this fits in
Current guidelines require GPs to annually review people with dementia who are registered at their practice. This study is the first, to date, to evaluate the quality of this review, together with more specific care provided in the management of cognitive and non-cognitive symptoms. The quality-of-care score presented here could be utilised to identify weaknesses in practice activity that need to be corrected, and provide information to help expand quality indicators for dementia. Improvements in care should particularly target the care for people with vascular dementia and those with dementia who continue to be prescribed antipsychotic medication.
METHOD
Sample
Five primary care trusts (PCTs) in the Greater Manchester region took part in the study: Ashton, Leigh and Wigan; Bolton; Bury; Oldham; and Stockport. Each participating PCT provided a list of all general practices in their area together with the practice’s list size, population aged >65 years, patients on the dementia register, and the number of GPs working at the practice. Using these characteristics for stratification, this study aimed to include a stratified random sample of 53 practices from the five PCTs.
A sample of 71 practices was generated initially to cover potential refusals. Practices were sent invitations to take part and, if they refused, another practice with similar characteristics was chosen at random to participate. Participation was secured from 52 practices; the refusal rate was low (overall 27%, range for PCTs 20–33%), representing 21% (52/249) of all practices existing in the five PCTs at that time.
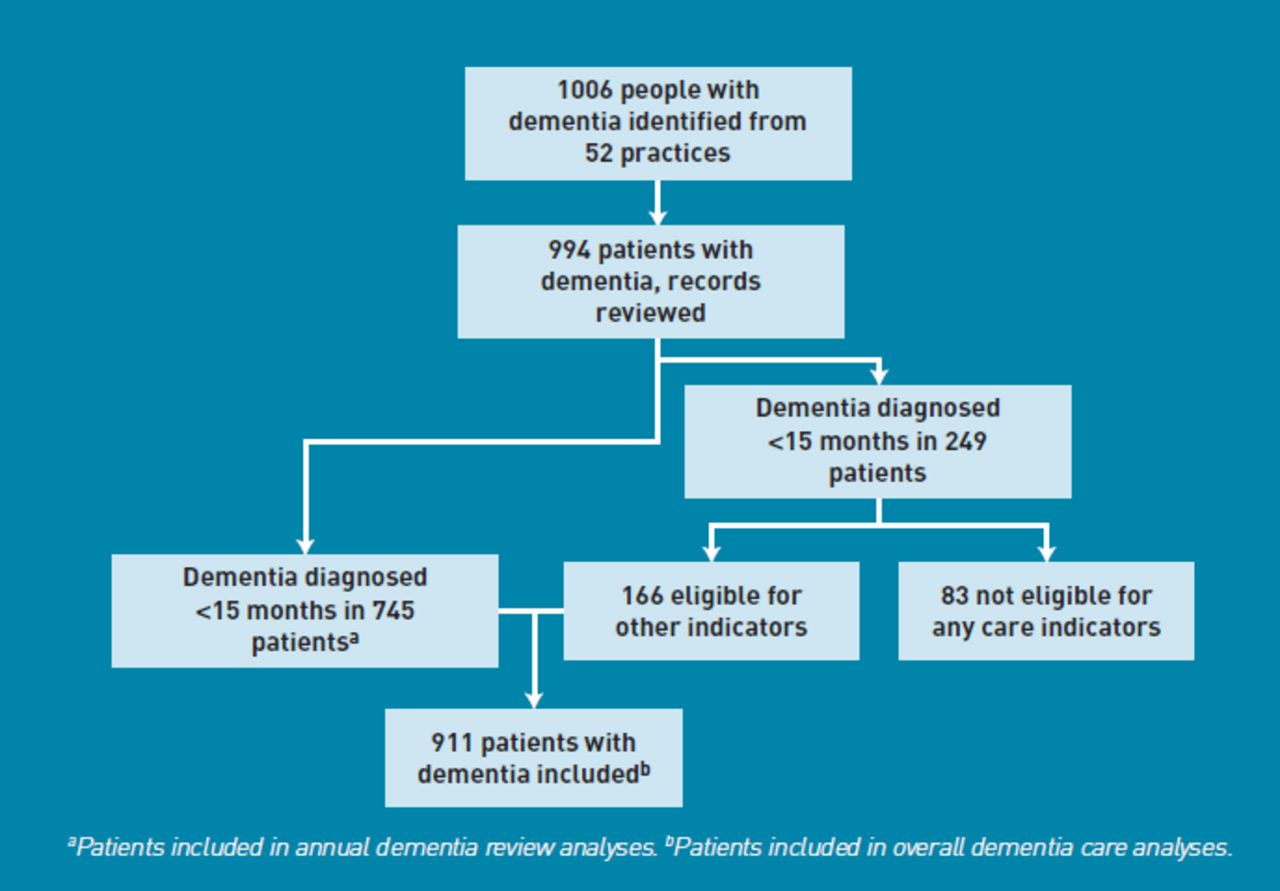
Patients with a dementia diagnosis were identified if they were listed on the dementia register at each practice. Information from 1006 patient records was collected in total. From this, 12 patients were excluded because they were deceased, or their dementia diagnosis was clearly disputed or revoked in their patient records; the final sample consisted of 994 patients with dementia.
Data collection
For each patient, information was collected by trained staff from electronic and paper records that were held by the general practice; this was done using a pro forma tool, designed in collaboration with a steering group of representatives from primary care and old age psychiatry. The process was piloted on patients in one general practice to resolve any ambiguities, and included patient demographics (age, sex, and living situation), dementia subtype, current medication use, and comorbid medical conditions.
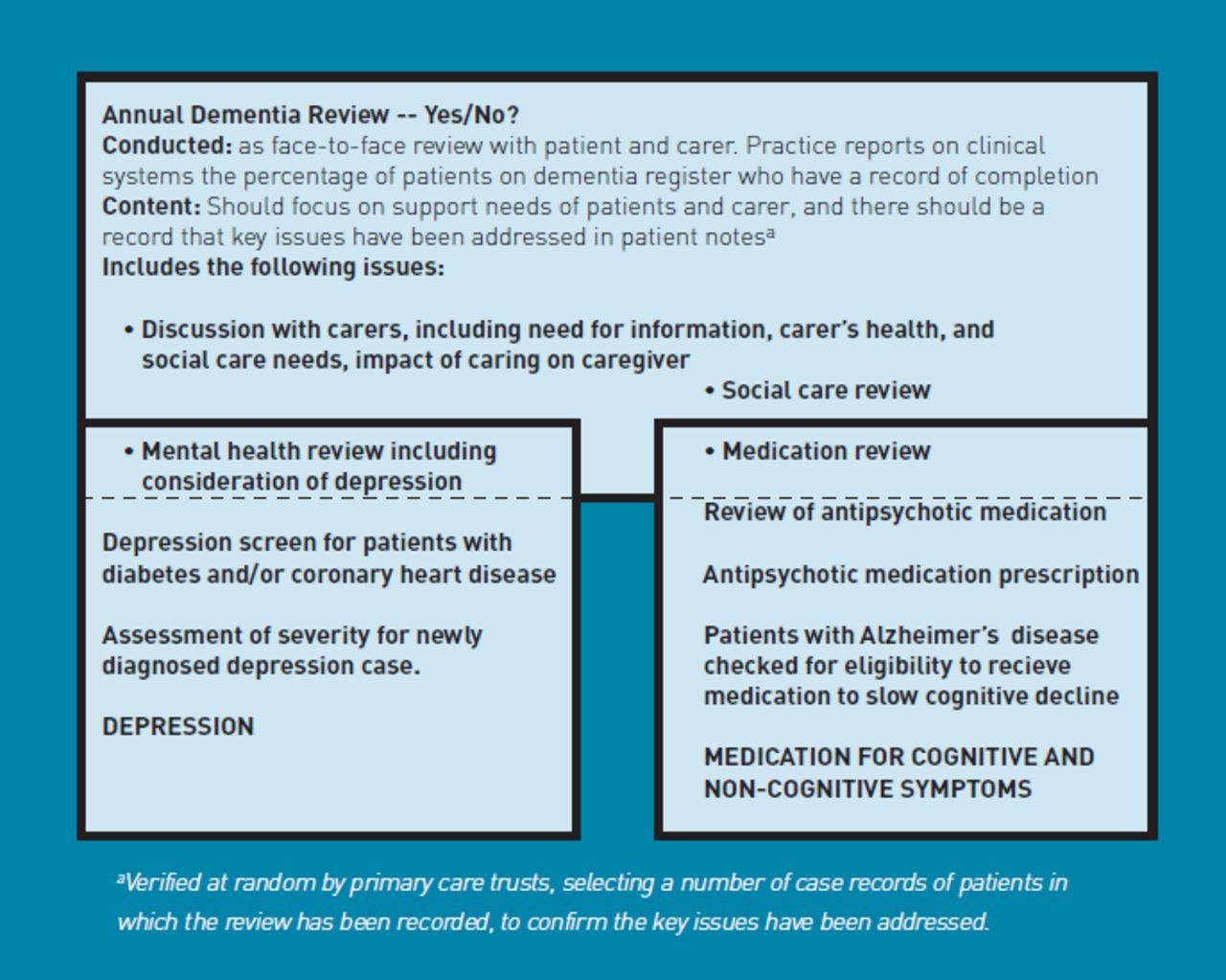
Information used to determine adherence to the dementia quality indicator in the UK pay-for-performance QOF 2008/2009 guidelines for primary care, which specifies that people with dementia have a record of dementia review from the previous 15 months, was obtained. If present, details were extracted for each of the four components of the annual review contents, as described in QOF guidelines, covering discussion with carers, medication, mental health, and social care reviews (Figure 1). Additional mental-health review data were also extracted in terms of adherence to two QOF indicators for depression:

Overlap between annual dementia review and other quality indicators.
Patients with diabetes and/or coronary heart disease, for whom a case finding for depression had been undertaken using two standard screening questions in the previous 15 months; and
Patients with a new diagnosis of depression (preceding 1 April until 31 March from 2007–2008), with an assessment of severity at outset of treatment. In accordance with national guidance,13,14 for those being prescribed antipsychotic medication at the time of the study, the date of initiation, the reason for it, and evidence of medication reviews were recorded, along with the consideration of cognitive-enhancing medication (cholinesterase inhibitors or memantine) in those diagnosed with Alzheimer’s disease.
Quality of annual dementia review and overall dementia care
For those patients diagnosed with dementia >15 months previously (n = 745), the quality of their annual dementia review was measured by whether or not it and its four components had been completed. The quality rating ranged from 0 points (no evidence of annual review) to five points (annual review was done and included all four components) for each patient. The quality of care was examined in further depth by assessing specific care processes, such as use of medications to slow cognitive decline in Alzheimer’s disease;13 reasons for, and review of, prescribing antipsychotic medications;15 and screening and treatment for depression.12
Figure 1 illustrates the areas of overlap between measures in the annual dementia review and specific care processes. All indicators for dementia review and specific care processes were summed for each patient. The overall quality of care was equal to the number of relevant measures for which care was provided, divided by the number of measures for which the patient was eligible. Patients differed in the applicable number of measures; two examples of this variation are presented in Table 1.
Computation examples of denominator for quality-of-care score
The score represents the proportion of indicators adhered to for each patient, with 0% indicating poor care and 100% indicating best-recorded care. This approach has been used in similar studies of overall quality of care for other major chronic diseases16 and gives each patient equal weight, regardless of how many indicators apply.16,17
Statistical analysis
All descriptive statistics were performed using SPSS for windows (version 16.0). For accuracy purposes, patients who had been diagnosed with dementia in the previous 15 months (n = 249) were excluded from the analysis of annual dementia review. For overall care, patients who were eligible for at least one of the other care processes were included, even if they were not eligible for dementia review (Figure 2).

{kind=link}
{kind=link}
Sample in analyses to assess quality of care in dementia.
Multilevel ordinal regression and multilevel linear regression were used to investigate the factors associated with quality of dementia review and overall quality of dementia care, respectively. Multilevel analysis is a method for dealing with a lack of independence within clusters; for instance, here there were three levels: patient, practice, and PCT.18,19 Initially, univariate associations of patient- and practice-level independent variables that may affect quality of care were explored. Patient-level variables included:
age;
sex;
dementia duration;
living situation (in nursing/care home versus community);
comorbid physical conditions;
medications; and
dementia subtype of Alzheimer’s disease including mixed dementia, vascular dementia, and other dementia.
Practice-level variables were:
whether the practice was run by one GP (single-handed) versus several (multi-handed);
socioeconomic deprivation of practice location, as measured by the Index of Multiple Deprivation 2007;20 and
size of population aged ≥65 years.
Multivariate models, adjusting for age, sex, and all other independent variables were then analysed. A normalising transformation could not be applied to the non-normally distributed dependent variable used in these analyses. Although regression analysis has been found to be reasonably robust to some degree of non-normality,21 sensitivity of the main analyses were assessed for overall care by using a multilevel ordinal logistic model. No differences in significance were identified between the main and sensitivity analyses; as such, results are reported from the main analysis. All multilevel modelling analyses were performed using Stata (version 11.0).
RESULTS
Demographics
The demographic characteristics of all patients (male 32%, mean [SD] age 81.6 [8.7] years] and general practices (n = 52, mean [SD] list size 7461 [1416]) are shown in Table 2. The median years’ duration of dementia (that is, since diagnosis) was 2.8 (interquartile range [IQR] 1.3–4.9), and the majority (51%) of the sample lived in the community. A total of 883 (89%) patients had at least one comorbid (physical) condition (data not shown) and 565 (57%) had multimorbidity (≥2 comorbidities). The most prevalent comorbid vascular-related disease was hypertension (44%), followed by coronary heart disease (20%), stroke/transient ischaemic attack (TIA) (17%), and diabetes mellitus (14%). A total of 745 patients were diagnosed ≥15 months prior to the study and were eligible for inclusion in the analyses to assess quality of care.
Characteristics of patients with dementia and general practices included in the study
Quality of dementia care
Table 3 shows that, in 599 (80%) patients, there was a record of an annual dementia review being completed; however, less than two-thirds of patients had a record of discussion with carers and just over a half had their social care reviewed.
Indicators of quality of care provided to patients with dementia
Eligibility checking for cholinesterase inhibitors or memantine for patients with Alzheimer’s disease was relatively high (86%). Although 259 (26%) of all 994 patients were prescribed antipsychotic medication at the time of the study, the presence of hallucinations and/or delusions was the reason for prescription in only 69 (27%) of these. The median duration of antipsychotic prescription was 23 months (IQR 8–42) and, of those prescribed antipsychotics for >15 months (n = 129), half (n = 66; 51%) had their medication reviewed in the previous 6 months, and 99 (77%) in the previous 15 months.
The proportion of patients meeting the quality indicators for depression screening and assessment were low — 55% and 11% respectively.
Predictors of quality of dementia review and overall care
Table 4 shows the univariate and multivariate predictors for dementia review and overall care quality. Patient characteristics that were significantly associated with better quality of dementia review in univariate analyses included living in the community compared with living in a care home, and having a diagnosis of Alzheimer’s disease compared with vascular and other dementia. The only predictive practice-level characteristic was having more than one GP. In the multivariate model, multi-handed practices and patients with Alzheimer’s disease, compared with those with vascular dementia, remained predictors of better quality of dementia review.
Multilevel regression analysis results showing univariate and multivariate predictors of quality of annual dementia review and overall care
The characteristics univariately associated with better overall care were the same as those for dementia review, but also included shorter duration of dementia. Patients with Alzheimer’s disease, compared with all other dementia subtypes, and multi-handed practices, remained factors significantly associated with better quality of care in the multivariate model.
DISCUSSION
Summary
The findings of the current study show that although, according to their medical records, the majority of people with dementia had a received their annual dementia review, the quality of that review varied and, for many, did not include social care review and discussion with carers. Inappropriate prescription and monitoring of antipsychotic medication was also apparent, despite the high prevalence of vascular comorbidity in the sample. People with Alzheimer’s disease and those in multi-handed practices received better quality of care, while those with vascular dementia and those in single-handed practices received a poorer quality of care.
Strengths and limitations
To the authors’ knowledge, this is the first study to date that has evaluated the annual dementia review, as specified by the QOF in primary care. The data used in this study were collected before the national dementia strategy was published in 2009, and, hence, before most PCTs started to implement dementia education. As such, the multilevel methodology of this study could be used to compare the performance of the new GP consortia and to capture the potential effects of PCTs’ educational interventions. As the practices in this study were also selected through a random stratified sampling process, there was a broad representation of practice characteristics; these are, therefore, likely to be reflective of general practices in other areas in the UK.
There are, however, several limitations that deserve comment. Information on all measures of care for patients with dementia were derived from medical records, which may not necessarily represent the actual care received. Although incomplete medical records may underestimate care quality, documented care can be, in itself, a measure of quality;22 the findings may highlight areas in which documentation needs improvement.
Care for somatic comorbidities (for example, hypertension) which have been found to be equally well controlled in patients both with, and without, dementia were not included in the study.23 Quality indicators — even bundled indicators that emphasise the importance of individual specific review — cannot reflect or assess the complexities of primary health care and the uniqueness of individual patients24,25 but, rather, involve making and assessing generalisations about individual patients. The quality of a dementia review will also depend on the continuity of care, interpersonal care, and trust between health professional, patient and, where appropriate, carer. QOF indicators, by their definition, can only ever address isolated and measurable aspects of this wider complexity.
In addition, although equal weighting of quality indicators is a conventional statistical approach that has been used in similar studies,16,17 it may not accurately reflect differences in their clinical significance. It was not possible to assess whether patients were also under the care of a secondary care professional and reviewed in more detail by them, rather than their GP. If this is the case, this study’s findings may indicate that communication and coordination between these services needs improvement. However, responsibility for continued prescribing of medications, such as antipsychotics, and, hence, medication reviewing is a responsibility that lies with the GP. Finally, adequate and timely dementia care requires recognition by GPs, which, particularly for those with mild dementia, is only met in approximately half of cases.26
Comparison with existing literature
In contrast with the management of cognitive symptoms in people with Alzheimer’s disease, the provision of care received for non-cognitive symptoms was poor. This is consistent with ongoing evidence of suboptimal management of BPSD,7 including high antipsychotic prescription and misuse.27,28 A recent study of 315 general practices in Scotland also found increased and prolonged use of psychotropic medications in people with dementia compared with the general population of older people.29
Differences between dementia subtypes may facilitate or hinder attendance to appointments with GPs or other health professionals, which may help to explain the poorer care received by those with vascular dementia; for instance, some studies have shown those with vascular dementia to be more functionally impaired and to experience more difficulties in activities of daily living than those with Alzheimer’s disease.30,31 As well as slowing the progression of symptoms, the prescription of cognitive-enhancing medication to those with Alzheimer’s disease provides the need to review, by either primary or secondary care services, in accordance with the guidance,13 and may provide an opportunity to address other care needs. Also, in terms of research that has been undertaken, vascular dementia falls behind that for Alzheimer’s disease and other common conditions affecting the brain; as such, little is known regarding its prevention or treatment.32 As those with vascular dementia cannot be prescribed cognitive-enhancing medication13 and there is no other such treatment currently available, they may be less likely to be followed up and less likely to receive higher levels of care.
Practices that were run by more than one GP were associated with better quality of care compared with those run by one GP. Although there is no definitive evidence that suggests one practice type is superior, lack of time for consultation has been identified as a barrier that prevents GPs from doing as much as they would like in caring for patients with dementia and their families.33,34 This is, perhaps, even more of an issue for practices run by one GP, as opposed to those run by several GPs where workload may be shared, such as through delegating a special interest GP responsible for dementia patient management or dementia clinics.35
Implications for practice
As well as identifying potential weaknesses in practice activity that need to be corrected, the quality-of-care score developed in this study may be valuable to commissioners and regulators to use as a quality marker and in performance management. In addition, it includes information that could be used to expand the QOF dementia domain in the future. For example, adding more specific indicators covering management of medication, as well as mental health and social care, for patients with dementia may allow for improved assessment of quality. This would also be useful in light of the commitment to reduce antipsychotic use in people with dementia by two-thirds by November 2011.36
This study’s findings indicate that research leading to improved care for people with vascular dementia should be made a priority. This supports the goals set out by the 2007 Alzheimer’s Society workshop on research priorities for vascular dementia, including research programmes to find new therapeutic interventions.32 While such research is taking place, quality indicators that specifically target people with vascular dementia may help to ensure that symptoms of dementia and their effect on the management of comorbid vascular diseases are monitored regularly. Addressing the deficiencies in dementia care is important to maintaining the quality of life for all people with dementia, not just those with vascular dementia; this is particularly the case given that disease-modifying strategies are not yet available.
Acknowledgments
Thanks to Vonda Hamilton and Michelle Griffiths (Manchester PCT); Robert Hallworth (Stockport PCT); Reehana Khan (Oldham PCT); Angela Christopher, Michelle Garret, and Sharon Mott (Ashton, Wigan and Leigh PCT); Paul Campbell and Lesley Gray (Bury PCT); and Christine Atkinson (Bolton PCT) for their help in data collection.
Notes
Funding
This work was funded by the Greater Manchester primary care trusts.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received May 31, 2011.
- Revision received July 11, 2011.
- Accepted September 15, 2011.
- © British Journal of General Practice 2012
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

