Article Text

Abstract
Background: Housing is an important environmental influence on population health, and there is growing evidence of health effects from indoor environment characteristics such as low indoor temperatures. However, there is relatively little research, and thus little firm guidance, on the cost-effectiveness of public policies to retrospectively improve the standards of houses. The purpose of this study was to value the health, energy and environmental benefits of retrofitting insulation, through assessing a number of forms of possible benefit: a reduced number of visits to GPs, hospitalisations, days off school, days off work, energy savings and CO2 savings.
Methods: All these metrics are used in a cluster randomised trial—the “Housing, Insulation and Health Study”—of retrofitting insulation in 1350 houses, in which at least one person had symptoms of respiratory disease, in predominantly low-income communities in New Zealand.
Results: Valuing the health gains, and energy and CO2 emissions savings, suggests that total benefits in “present value” (discounted) terms are one and a half to two times the magnitude of the cost of retrofitting insulation.
Conclusion: This study points to the need to consider as wide a range of benefits as possible, including health and environmental benefits, when assessing the value for money of an intervention to improve housing quality. From an environmental, energy and health perspective, the value for money of improving housing quality by retrofitting insulation is compelling.
Statistics from Altmetric.com
Housing is a key environmental influence on population health.1 People in developed countries such as the USA, Canada and New Zealand spend about 90% of their lives indoors and most of this time is spent at home.2 3 Improving housing is a preventive health strategy with social benefits: exposure to substandard housing is not evenly distributed across populations.1 Recent studies have provided increasing evidence on the specific health risks and costs of a cold, damp and mouldy indoor environment.4 There are health risks associated with low indoor temperatures during winter and high temperatures in summer.5 6 Cold housing, below the World Health Organization recommended minimum of 18°C,7 has been associated with avoidable excess winter mortality.8 9 Increasing periods of high temperatures associated with climate change have been linked to extreme indoor temperatures, and higher mortality, in the USA and Europe.10 11
There is little solid research on the value for money of improving housing quality.12 Methodological questions can be raised about the benefits that some studies13 ascribe to residential energy efficiency measures. What studies there are tend to either present the analysis of housing improvements in terms of a benefit–cost ratio, where benefits over the lifetime of an investment are discounted back to the present and compared with costs,14 or present results in terms of a net present value (NPV) estimate of “discounted benefits less costs”, as reported for residential “weatherisation” programmes in the USA.15 These measures are useful for both house owners (public or private) and policy advisers estimating how much to invest in public assistance for housing improvements. The challenge is to reliably estimate the range of benefits, such as health benefits of damp and mould reduction or injury prevention, energy savings and benefits accruing beyond the household in question, such as improved outdoor air quality, noise reduction or CO2 emission savings.
While many countries including the UK and New Zealand are setting higher standards for new housing,16 17 most of the existing housing stock was not built to these standards. There is little guidance on the relative benefits and costs of retrospectively improving the standards of these houses. Some studies have modelled the effectiveness of retrofitting insulation. A US survey of retrofitting of multiunit housing18 found highly variable payback periods for various retrofits, including insulation; a British study of private rental housing found retrofitting insulation effective in terms of modelled reductions in fuel use.19 Another study undertook a payback analysis based on simulating the energy-saving effect of insulation retrofitting of a single house.20 Although the first of these studies touched on comfort, none reported health improvements.
One study examined energy measures in low-cost housing in South Africa,21 and concluded that health benefits, along with employment gains and reduced local household expenditure, justified modelled energy efficiency measures. Another study22 identified significant health benefits, based on extrapolating ambient air pollutant emission savings from energy use simulations. A Swiss study noted that co-benefits, such as improved living comfort, good indoor air quality and better noise protection may yield gains of the same order of magnitude as energy-related benefits.23 An Irish study modelled the returns on domestic energy conservation opportunities, concluding that a home retrofitting programme would result in a 3:1 benefit–cost ratio, including energy savings, health benefits and reduction in avoidable mortality.6 None of these studies, however, used direct empirical evidence on health outcomes. Only two empirical studies are known that report health benefits from insulation. One is a study in Cornwall (UK), for which the positive results were weakened by methodological limitations,24 and benefit/cost data were not supplied. The other,15 on US weatherisation programmes, reports a wide range of estimates of the benefit of illness avoided.
Potentially, health benefits of installing insulation can accrue in a number of ways, such as a reduced number of visits to GPs, hospitalisations, and days off school or work. These benefits can accrue simply through the general effect of greater warmth and dryness on respiratory health, or through specific mechanisms such as reduced allergens and mould in the house. Households may also make energy expenditure savings, since a given temperature in the home may be reached with less heating, or they may take the benefits from insulation in greater comfort, rather than making energy expenditure savings. In New Zealand, the current context is one of residential energy use being projected to grow rapidly in coming decades25(p 108), from a base of low per-household current energy use.26
Partly because New Zealand has a temperate climate, about a third of all dwellings still have no insulation (insulation has been required in new houses since 1978); nevertheless, low indoor temperatures are common. Around 3% of people use no heating,27 and winter evening temperatures in the living room (often the only room in the house consistently heated) average just below 18°C.28
OBJECTIVES
The Housing, Insulation and Health Study was a cluster randomised trial of retrofitting insulation in predominantly low-income communities. The study was specifically designed as a practical community-level intervention to assess whether installing insulation in houses has any impact on the occupants” health or the energy they use. Aims, methods, main results and ethical approvals have been reported elsewhere.29 30
To estimate as full a range as possible of benefits and costs, objective data were collected wherever practical on aspects of health and wellbeing, and environmental factors such as energy and emissions which contribute to wider wellbeing. This paper reports on the benefit–cost ratio and net present value of the retrofit intervention, on the expectation that a better picture of these values may assist in the formulation of improved housing, health and environmental policy. This study is the only prospective study of its type of which we are aware.
METHODS
As this paper provides an economic analysis of the main results of a randomised trial of the retrofitting of housing insulation, the main trial method is first described in brief only. This is followed by a summary of the methods used to place values on the costs and benefits of the intervention, and the method used to bring these together, using the discounted present value technique.
Households in which at least one person had symptoms of respiratory disease were recruited from seven predominantly low-income communities in New Zealand. Many of these areas are growing and most are not suffering depopulation—a consideration in estimating the expected lifetime of dwelling insulation. The 1350 households (4407 people) were randomised within communities to receive retrofitted insulation during or after the study. There was an 85% household retention rate and a 75% individual retention rate. Houses, which were all built before 1978 (when insulation became mandatory), were insulated by installing a standard insulation package. The indoor temperature and relative humidity, mould growth and energy consumption of the houses in the study were measured, as well as changes in the health and wellbeing of the occupants and their healthcare utilisation.
Measures at baseline (2001) and follow-up (2002) included self-reported measures of health, comfort and wellbeing and primary care (GP) visits, and days off school and work; and independent measures of temperature, relative humidity, mould (speciation and mass), endotoxin, β-glucans, house dust mite allergens, GP and hospital visits. At baseline only, there was an independent assessment of house condition. While full records over the 2 years of the study were collected for energy consumption (including self-reported bottled gas, wood and coal use), energy savings estimates reported here were based only on metered data, that is electricity and gas usage. All measurements referred to the three coldest winter months in the southern hemisphere (June, July and August).
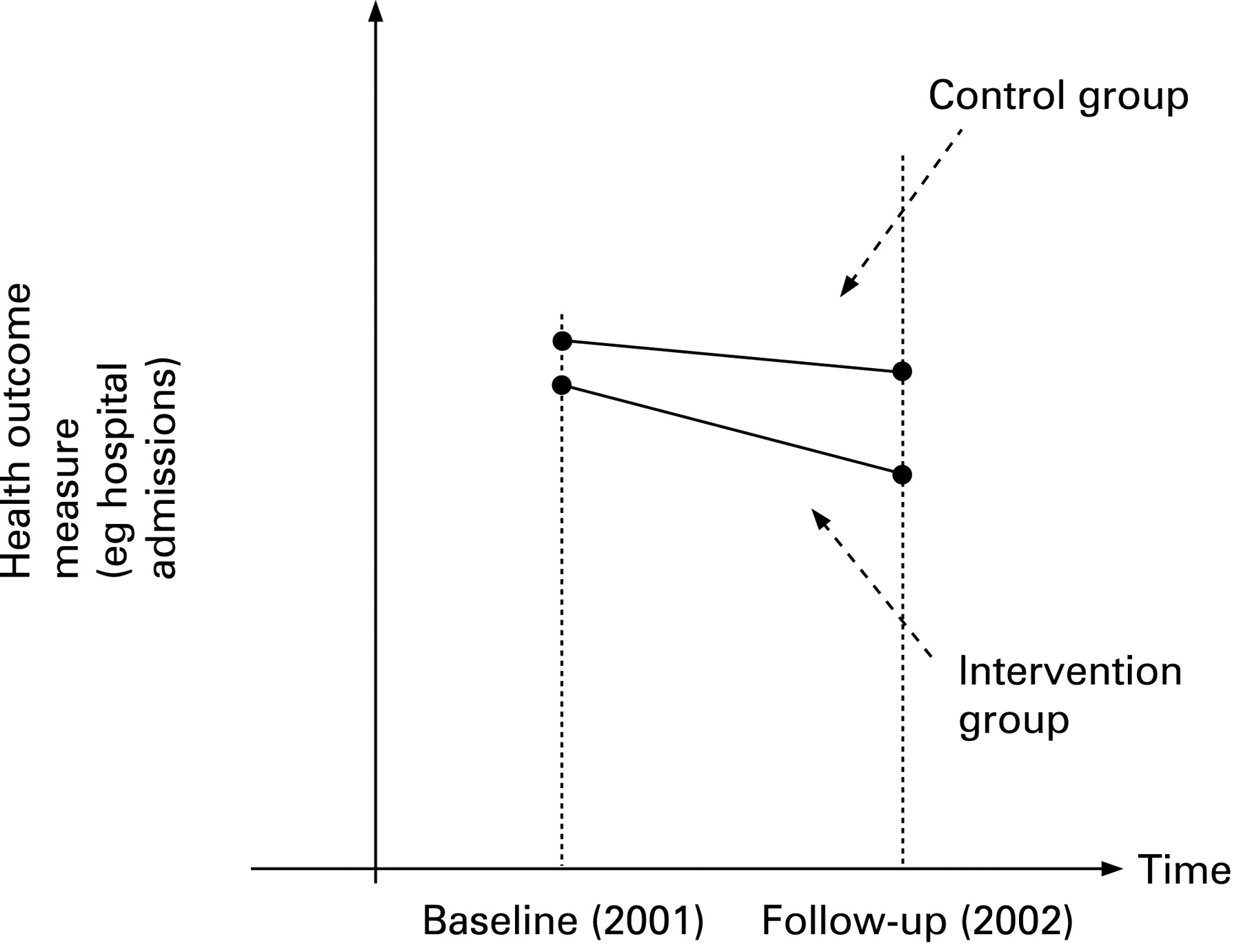
Baseline data were collected over the first winter. Dwellings were then insulated after the first winter, in the case of the intervention group, or after the second winter of the study, in the case of the control group. The analysis allowed for baseline health differences between the control and intervention groups, and changes over time in health conditions and outcomes for the control group (see fig 1). For example, hospitalisations may have fallen x%, say, in the intervention group, between baseline and follow-up winters, but only y%, say, in the control group. The net reduction, allowing for the changes in the control group, and which can be ascribed to the intervention, is, in this example, (x−y)%.

{kind=link}
Allowing for changes in the control group.
Valuing costs and benefits, and assumptions
The cost side of the analysis is straightforward: the overall cost per household in 2001 was NZ$1800 (excluding value added tax) (NZ$1 = £0.29 and US$0.42 at 2 January 2002.) Three types of benefits from installing insulation were valued—health gains, energy and associated greenhouse emission savings. Health effects able to be quantified and valued were changes in the number of visits to GPs, the number of hospitalisations, and the number of days off school and off work. Potential health gains not assigned a value include the everyday enhancement of physical and emotional wellbeing arising from a warmer and/or more comfortable dwelling, and avoidable premature mortality. Although wellbeing was quantified using a reliable survey instrument (SF36), which assesses changes over time, it has not been possible to place a reliable economic value on the gains.
The cost reduction estimates were scaled up by a factor to allow for gains over a whole year rather than the 3-month winter period monitored in the study. Cold days are likely to be correlated with health impacts. For the horizon of the benefits, an estimate of 30 years is used, taking into account that the insulation can be expected to continue generating benefits over its lifetime, estimated by some manufacturers to be 50 years. A long horizon is consistent with the estimated 90-year average service life of the housing stock:31 the latter implies that an entirely random sample of housing might be expected to have a remaining life of around 45 years. In this study, where the sample is limited to pre-1978 houses, 30 years is around the estimated midpoint of the houses’ remaining life.
Benefits from reduced healthcare needs
The benefit of a reduction in the number of visits to GPs is estimated using GP records of the number of visits, and an estimate of the resource cost of a GP visit.32 The benefit of a reduction in the number of hospitalisations is estimated using the reduction in the number of hospitalisations for respiratory complaints, categorised into overnight (inpatient) and day (outpatient) admissions, together with an estimate of the cost of a hospital admission, ignoring the cost to the household. Estimates for the costs of asthma admissions are used,33 with prices appropriately updated.34 For children, cost estimates for 2002 were NZ$597 for a day admission and $1195 for an overnight admission; for adults (18–64), cost estimates were NZ$740 and NZ$1480; and for older people (65 or over), $1347 and NZ$2694.
Benefits from reduced “days off school” and “days off work”
Days off school represent a cost in terms of forgone education, and may also cause a parent to take a day off work in some cases. Recent New Zealand research suggests that higher levels of absence from school may be detrimental to academic achievement.35 This is consistent with a US study in which absenteeism from school was found to have a significant (p<0.01) inverse relationship with standardised test scores.36 Since absence from school is linked to academic achievement, which in turn relates to earnings, the value (cost) of a day off school for a teenager can be linked to the labour market youth wage rate; conservatively, we assume that for teenagers aged 13–18, the value of a day off school may be around half the youth minimum wage, or around NZ$30 per day.
While dwellings will vary in whether they contain school age children or not, on average the proportion of dwellings with school age children is assumed to stay about the same over the 30-year horizon. We estimate the benefit to society of a worker avoiding a day’s absence from work by taking, conservatively, about 80% of the average daily wage rate for workers,37 on the basis that a day off does not result in a full day’s loss of productivity because some of the loss can be made up upon the worker’s return to work.
Energy-saving benefits
Energy benefits were expected to accrue principally from reduced energy spending. Additional economic benefits can accrue to the electricity network companies in the areas where the houses are located, if households reduce peak demand. This benefit includes the value of avoided additional lines investment to cope with peak loads. The peak load electricity reduction was measured in a subsample of 116 households. In this analysis, the load reduction is reported, but an economic value is not ascribed to it.
The benefit of electricity or mains gas savings is based on an estimate of the number of units (kWh) of electricity or gas saved during the three winter months of the study; and an estimate of the value of a residential electricity or gas unit at around the time the insulation was installed.38 We make a conservative assumption of a zero real price increase over the estimation horizon. Thus, this study’s energy saving estimates probably understate the true value of savings.
Benefits of greenhouse gas emission reductions
These benefits were estimated for the energy savings for which the most reliable data could be collected, that is for electricity and mains gas. Valuation assumed a per unit value of NZ$30 per tonne of CO2, based on interpretation of a range of sources,39–41 and that the real price of CO2 per tonne would be maintained over the 30-year horizon.
Discounting
Since all the benefit flows accrue over time, the flows are converted to present (discounted) values, using a 5% discount rate and a 7% rate over a 30-year horizon. The 5% rate is viewed as a representative “base case” discount rate, and 7% is provided as a sensitivity analysis variant, recognising that views vary concerning appropriate rates. We consider that a social rate of time preference concept (associated with a lower rate) is more applicable than an opportunity cost of capital concept reflecting financial sector interest rates.15 42 We place more weight on the 5% rate because the housing context is one of “social” investment, in the sense that insulation appears to be underprovided by the market, and yields a mix of health, energy saving and environmental benefits over time. We note that the New Zealand Treasury until recently used a rate of 10%, but now suggests a “standard” rate of 8% and a rate for building investments of 6%.43
RESULTS
In the random control trial, almost all the differences between the intervention and control groups on measured outcome variables were statistically significant.30 Consequently the statistical tests on individual outcomes are not repeated here. We report here, in order, estimated health benefits, energy savings, imputed CO2 emission reduction benefits and, lastly, an overall estimate of the net benefits, in present value terms, of the investment in insulation. Table 1 shows a small increase in the number of GP visits over the 3 months of winter. The estimated total cost increase is around NZ$165 per household.
Hospital respiratory admissions data are shown in Table 2, for both outpatient and inpatient admissions. Teenage admissions data are not separated out, because hospitalisations are a very rare event in this age group. The reduction in inpatient (overnight) hospital stays for older people constituted the greatest area of health cost saving.
Days off school are shown in table 3, for school age children and teenagers (gains for pre-school children are not readily valued and are therefore excluded). Similarly, days off work are shown in Table 4. For both sets of data, changes in “days off” are estimated based on the children/adults for whom data are available for both 2001 and 2002.
Table 5 reports estimated energy savings. A “typical” household (one with a heating pattern typical of the weighted average of all households in the study for which there is good data) benefited from net energy savings (metered electricity and gas) of 13% since intervention group energy use declined 5% while control group use increased 8%. This net saving amounts to around 318 kWh per household over the winter, and 532 kWh over a full year. Although the reduction in metered energy use was not statistically significant at 5% (given the limited number of households for which both years’ records were available), the reduction in energy use based on both measured and self-reported energy use was statistically significant at the 1% level (p = 0.0006)29 (table 4). Because it is more difficult to price non-metered energy sources such as firewood, we have estimated the value of metered energy use only.
Note, in addition, that a subsample of electricity consumption in 116 houses in one city in this study showed a significant average decrease in peak period demand of 25.5% from 2.15 kW to 1.60 kW. This has significant regional and potentially national implications for power generation, as it is peak demand that drives the need for electricity generation, transmission and distribution capacity at the margin.44
CO2 savings are estimated on the basis of metered energy savings.
Total savings (monetary value of benefits discounted back to the point at which the costs are incurred) are shown in table 6: they amount to NZ$3374 per household, with total costs of $1800. Thus, net benefits (or to be exact, the NPV of net benefits) are $1574 per household. About two-thirds of the benefits are due to reductions in hospital admissions. The benefit–cost ratio is 1.87:1, a comfortable margin above 1.0. At a higher discount rate of 7%, the ratio is 1.59.
DISCUSSION
The present benefit–cost study summarises the overall social impact of the intervention, which showed positive effects which were mostly statistically significant. We are interested in the social implications of the intervention for policy.45 The benefit estimates in this study are generally based on the 1281 households and 4183 people in whose houses insulation was installed (91% of the original sample of 1400 enrolled households). For energy and CO2 savings estimates, however, we have less complete information, and estimates are based on a sample of households for which we have complete energy use data.
The overall result of a benefit–cost ratio approaching two (and an NPV of around NZ$1570 at a discount rate of 5%) means that the benefits accruing over time, in terms of health gains and energy savings, are a comfortable margin in excess of the costs of installing insulation in the houses in the study. The estimated benefits are resource savings in the health sector and energy sector, and the value of avoided days off school and work, together with wider community benefits of emission reductions. We note that fiscal savings (reduced government health spending) in the health sector will be less than resource savings. More than half the total benefits (61%) were health sector gains.
The overall benefit estimate may be understated for various reasons. First, there was some heterogeneity in the delivery of the intervention—about 90% of the households received around 80% or more of the intervention. The analysis was based on “intention to treat” and thus the heterogeneity means that the total benefits are likely to be understated. Second, there was a discrepancy between self-reports of visits to GPs and visits recorded by the stated household GP. While there was a statistically insignificant increase in household GP-reported visits, there was a statistically significant saving in self-reported GP visits.30 Many people in New Zealand visit a number of GPs, and self-reports may in fact be no more inaccurate than the records of GPs. The decision on grounds of consistency to use GPs’ records of visits rather than self-reported data in the total net benefit estimate means that the latter may be understated.
Third, energy saving estimates (electricity and mains gas) exclude other forms of energy saving, that is, reductions in bottled gas, wood and coal use for those dwellings with these forms of heating (typically complementary to electricity use). Although these are difficult to value reliably, we know that the quantities of wood and coal used fell for insulated dwellings in the study compared to control group dwellings. In fact, in terms of estimated kWh, energy consumed in alternative forms fell at least as much as energy consumed in metered forms (electricity and gas). Exclusion of non-metered fuels, together with conservative assumptions such as that of no assumed increase in real energy prices or CO2 prices over the next 30 years, means that estimates of overall energy and carbon emission savings are conservative.
Fourth, there are difficulties in obtaining reliable unit costings, including for hospital admissions and for valuing days off school. We have therefore used conservative estimates of costings of hospitalisation and days off school. The latter, for example, are based on considerations of forgone education and the need for children off sick to require care, thus incurring a loss of productivity. However, the total value of days off school, estimated for teenagers at around NZ$30 per day and for children 6–12 at around NZ$15 per day, is not particularly sensitive to unit costings. For example, if the unit cost for a child losing a day off school were NZ$30 rather than NZ$15, the total net present value of savings per household would rise by only 4% (in the 5% discount rate case).
The total benefit figures summarised above also exclude certain aspects of benefit noted above, in particular, significant enhancement of physical and emotional wellbeing arising from a warmer and/or more comfortable dwelling, possible reductions in mortality, and long-term health benefits as a result of reduced childhood illness. Cold housing is associated with avoidable excess winter mortality among older people, and insulation is likely to reduce this rate of mortality, although a study with greater statistical power is necessary to test this. Because these benefits are not readily valued does not mean they are any the less important, as noted elsewhere.46
A number of factors should be considered in drawing broader conclusions about potential benefits of retrofitting insulation for a wider population. The full benefits will only accrue in initially uninsulated houses, but some benefits will accrue even where houses are only partially insulated. It is also worth noting that the households in the sample were a mix of tenure types, although with a smaller proportion renting than the general population.29 The households were also distributed across a mix of areas, including small semi-rural areas, towns and cities, in both the North and South Islands. These areas are not atypical; they tend to be lower socioeconomic status areas, but not markedly so. There is also a limited number of house construction types in New Zealand and the sample was indicative of the range.
Most of the areas in the sample have been growing rather than suffering depopulation; this is relevant when considering the horizon of benefits from installing insulation. The lifetime of dwellings in New Zealand is considerably longer than the assumed 30-year horizon of the insulation benefits, as noted above. Nevertheless, we have estimated the sensitivity of the conclusion to assuming a 20-year (rather than 30-year) horizon of benefits from the insulation: at a 5% discount rate, and with a 20-year horizon, the benefit–cost ratio is reduced from 1.87 to 1.52 (NPV of NZ$935), still well above the breakeven level of unity, and implying that, even with a short horizon, benefits continue to comfortably exceed costs.
From a policy viewpoint, the questions addressed in this study are significant because of imperfections in the housing market.47 48 Such imperfections often reflect lack of information. For example, house buyers may not be aware that the health and energy benefits of better insulation may offset the additional costs of insulation, and building professionals such as builders and architects may not “build in” insulation because of uncertainty about whether the upfront costs will deter customers. Tenants are likely to be even less informed than house buyers, and landlords have weaker incentives to have regard to dwelling fabric and comfort than buyers, and thus may exert little influence on the actions of house builders and developers.19
Other imperfections reflect “externalities”: better insulation, where it generates better health outcomes, provides spillover benefits to the wider community in the same way that an effective public health system generates social benefits. To the extent that insulation also lowers energy use, it generates environmental benefits (less air and water pollution, lower greenhouse gas emissions) and again, such benefits accrue to the wider community. Moreover, reductions in peak period demand generate electricity system benefits, a regional public good.
In short, there are various reasons why the market underprovides housing insulation, and these reasons include a lack of information about the health and energy benefits of such housing improvements. The corollary is that estimates of the full benefits of retrofitting insulation can be useful to policy advisers assessing the case for public investment in supporting the retrofitting of housing insulation.
Drummond and colleagues,45 (pp 8, 121) in a recent review of economic evaluations of public health interventions, noted that very few studies have considered costs and consequences outside the health sector and that very few complex interventions delivered at the population level have been subjected to economic evaluation. The present housing study involved consequences both inside and outside the health sector (e.g. reduced days off school, important in the education sector) that were able to be evaluated due to the trial’s design, even though the study was costly and complex. The study suggests that future research along similar lines to evaluate other housing determinants of health, energy and environmental outcomes will also be useful in a policy context.
CONCLUSION
Recently, the London Economist noted that house insulation improvements represent the lowest cost way, and can be a “negative cost” way, of achieving carbon emission reductions.49 The present study confirms that there are good reasons besides carbon emission reductions for retrofitting house insulation. We have directly estimated values for a range of benefits of retrofitting house insulation, and provided robust empirical benefit–cost data for the first time. The main results are that energy and environmental savings (such as carbon emission savings), are modest but significant, with larger savings accruing in terms of health benefits. The study underlines the point that, from a health, energy and environmental perspective, the value for money of improving housing quality by retrofitting insulation is compelling.
What is already known on this subject
Retrofitting insulation in dwellings provides health benefits and energy savings.
There is little empirical research on the extent of the economic value of different elements of benefit, and the overall cost-effectiveness of public policies to retrofit housing insulation.
What this study adds
This study, based on the Housing, Insulation and Health Study, provides economic value estimates for a range of co-benefits of retrofitting housing insulation, including the value of savings in GP visits, hospitalisations, reduced time off work and school, energy savings and reductions in CO2 emissions.
This assists policy advisers in evaluating and comparing benefits, including health and environmental benefits, when assessing the value for money of interventions to improve housing quality.
Acknowledgments
The authors are grateful to the many people who took part in this study. It was funded by the Health Research Council of New Zealand, Energy Efficiency and Conservation Authority, Ministry of Health, Solid Energy, Orion, Christchurch City Council, Environment Canterbury, Hutt Mana Community Trust, MARIA, Eastern Bay of Plenty Energy Trust, Wellington City Council and Housing New Zealand Corporation. We would also like to thank Dr Nigel Isaacs for his assistance with the energy data.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: Ethics approval was obtained.