Article Text

Abstract
Discharge summaries are important medical documents that summarise a patient’s hospital admission. The Royal College of Physicians provides standardised guidance on the content of discharge summaries, given their important role as a handover document to general practitioners (GPs). Our project started in June 2020 on an acute medical ward, where significant variation had been noted in the quality and content of discharge summaries. A multidisciplinary team (MDT) was formed including doctors, nurses and hospital/community pharmacists, as well as a patient representative, to ensure active patient co-design. The problem was scoped by asking GPs to provide feedback via surveys and process mapping. Our aim was to increase the compliance of discharge summaries with 10 core criteria from a baseline of 55% to 95% by June 2021. Change ideas were developed by the MDT and were tested using plan–do–study–act (PDSA) cycles that included additional pharmacy support, a discharge summary template and individualised feedback. The project reached its goal of 95% compliance in January 2021, 5 months ahead of the target date, and this improvement has been sustained since. The project expanded to a second acute medical unit ward in May 2021. The expanded project reached its goal of 90% compliance within 6 weeks and maintained sustained improvement with further PDSA cycles. A standard operating procedure has been created to help embed the changes on these wards. Our future aims are to redesign and improve the current electronic system and to help spread positive changes throughout the Trust.
- Continuous quality improvement
- Patient Discharge
- Continuity of Patient Care
- Electronic Health Records
- General practice
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Continuous quality improvement
- Patient Discharge
- Continuity of Patient Care
- Electronic Health Records
- General practice
Problem
Discharge summaries are important medical records that summarise a patient’s hospital admission, for the benefit of both the general practitioner (GP) and the patient. A discharge summary should contain a sufficient level of information to ensure that both patients and other healthcare professionals are aware of the relevant events of a hospital admission.1 2 The transition between different levels of care represents a potential area where patient care is at risk.3 It is important that clear communication is maintained between primary and secondary care regarding discharge plans.4 Poorly completed discharge summaries can negatively impact on the quality of clinical care provided, the safe transfer of care to the community, as well as patient safety and experience.
We developed 10 core criteria that should be included in discharge summaries, based on guidance from the Professional Record Standard Body2 and the Royal College of Physicians.1 These can be listed as: reason for admission, relevant medical and surgical history, primary and secondary diagnoses, key investigations and results, procedures, social context, plan for follow-up, medications changed during admission and the indications for this, medications to be reviewed by the GP and why, and GP actions post discharge. A baseline audit of the compliance of discharge summaries from an acute medical ward (ward 22) was undertaken in order to set a goal for our project. This showed discharge summaries achieved an average of 55% compliance with our 10 predetermined core criteria. We therefore set our project aim to improve the quality of discharge summaries by including all core criteria, from a baseline of 55% compliance to a target of 95% by June 2021. The project was subsequently expanded to a second acute medical unit (AMU) ward (ward 2) due to the success on the initial pilot ward.
Background
The project is based at a busy district general hospital providing planned and emergency care to local residents. The site has over 520 acute beds and in excess of 150 000 emergency department attendances per annum. On an average day, the acute medical team admit between 40 and 50 patients per 24 hours.
It was noticed that there were a number of issues raised to the Trust regarding discharge summaries, in particular GP quality alerts and Patient Advice and Liaison Service (PALS) feedback received from patients. This led us to re-examine how discharge summaries are completed and in what way we could both standardise and improve their content using quality improvement (QI) methodology. One of the recurrent themes highlighted was the variability in completion between different wards and trusts, leading us to centre our work around standardising discharge summary completion.
In order to understand more about the problem, a baseline questionnaire was distributed to various members of the multidisciplinary team (MDT), including GPs, hospital doctors, pharmacists and nurses. MDT feedback suggested that there were a number of elements of required documentation that were frequently missed or inappropriately documented, such as the patient’s social history, medication changes and follow-up plan. This feedback, combined with the results of our baseline audit suggesting poor compliance with key discharge summary elements, highlighted specific areas that were consistently poorly completed. We built on this information by using an MDT process mapping exercise, to ascertain the steps involved in creating a discharge summary. This was important to understand the individual components of the AMU discharge system, as well as the barriers to good quality discharge summary completion. Specific barriers we identified included a high turnover of staff on the wards, insufficient time for discharge summary completion coupled with a significant burden of clinical jobs, as well as poor awareness among new staff as to what specific information should be included. We also contacted another London National Health Service (NHS) Trust that had completed a similar QI project aimed at improving the quality of discharge summaries in the emergency department.5 Our team reviewed examples of their driver diagram, measures and change ideas for inspiration.
Measurement
Data were collected weekly throughout our project, with 10 random discharge summaries sampled from the ward each week and their compliance assessed against the 10 core criteria that should be included. To minimise selection bias, the medical record numbers of a random selection of discharge summaries were supplied by the ward clerk. Team members then assessed each summary individually, scoring against the key criteria using an anonymised spreadsheet. Our outcome measure was the average compliance of all 10 summaries each week, and the process measures were each individual core component. The 10 individual process measures were tracked to guide targeted plan–do–study–act (PDSA) development throughout the project. In total, over 500 summaries were assessed over 12 months for our pilot project, with a further 300 being assessed for our second pilot ward.
Throughout the project, we have monitored the number of complaints and quality alerts raised from each of the acute medical wards regarding discharge summaries to track our progress.
Design
We used a multidisciplinary approach to address the problem of variability of discharge summaries, even though we were specifically targeting what clinicians (doctors and physician associates) wrote in each summary. Our project team was established in June 2020 with a junior doctor as the project lead and an acute medical consultant as the project sponsor. The team included ward doctors, a physician associate, community and ward pharmacists, a GP, senior nursing staff from the ward, a QI coach. We initially held weekly virtual meetings due to the restrictions of the COVID-19 pandemic, which were then reduced to monthly meetings.
An important element in our project was patient co-design involving a patient representative. Our patient representative joined our project team having had personal experience of the hospital discharge process. They were invaluable in maintaining a patient-centred focus and ensuring that the specific aspects of discharge summaries, which matter to patients remained a priority for improvement. Our patient representative developed a questionnaire to assess patient understanding of discharge summaries, which was subsequently used for a PDSA cycle on our second pilot ward, with direct patient feedback shared at Board rounds (ward 2). Patient feedback has been positive with 80% reporting discharge summaries were easy to understand and 100% stating that they felt confident about plan following discharge.
Strategy
We ran multiple PDSA cycles on both wards inspired by the change ideas developed with the MDT.
Our first PDSA cycle involved including a pharmacist on the medical ward round, who identified which patients that were planned for discharge and provided feedback on what information should be included on discharge summaries regarding medication changes. This PDSA intervention lasted for 1 week, and we reached an average compliance of 74%. Our second PDSA involved a ward doctor providing individual feedback to those clinicians completing fewer than 8 of the 10 core elements (80% completion of discharge summary core elements). This PDSA was run 6 weeks after the first intervention lasted for 1 week and achieved an average compliance of 87%.
Both of these two PDSAs demonstrated positive feedback from the ward teams and improved the average compliance of discharge summaries. They were judged not to be sustainable long-term interventions however, as they were highly labour intensive strategies that involved significant time and commitment from both pharmacists and ward doctors that was not possible to maintain alongside their prior clinical duties and ward routine.
Our third PDSA cycle was the introduction of a template document containing all 10 core criteria listed as subheadings, with staff members asked to use the template for discharge summary completion for 1 week. It was noted that a template was introduced successfully when transitioning to a single e-discharge system, in a separate QI project.6 The template was created as a word document and saved on the network shared drive to be accessed by all clinicians. The intervention was run 2 weeks following our third PDSA and showed an improvement in compliance to 76% from 52% the previous week. The feedback from staff on the ward was positive, including that the template gave them a useful structure, made the process more efficient and increased the speed at which they were able to complete discharge summaries. Due to the positive feedback that we received from this PDSA, we adapted this format for further testing for our fourth PDSA cycle. This PDSA was run 2 weeks after our third PDSA, and was performed over a 2-week period. We combined this with project posters on the ward detailing weekly compliance updates. This again showed an improvement in the data to 83% and 84% average compliance over the 2 week period, with further positive feedback from the ward clinicians.
Given that we achieved significant and sustained improvement in average compliance on our initial pilot ward, our project was subsequently expanded to another AMU ward (ward 2) in May 2021. Baseline compliance on this ward was measured as 61%. With the success of the discharge summary template (PDSA 3) on the initial pilot ward, this was the first PDSA to run on our second pilot ward over a 1-week period. Introduction of this template showed an improvement in average compliance to 92% for that week. This showed that the positive effects of our discharge summary template were reproducible on multiple wards. We received similar positive feedback from clinicians again regarding its usefulness and efficiency.
The second PDSA involved using the patient feedback questionnaire, developed by our patient representative, to gauge patient feedback. This was run 8 weeks following our first PDSA, and was performed over a 2-week period. The patient feedback was shared with the ward at board round. We achieved an average compliance of 87% and 91%, and pharmacy input in changes to medications on discharge.
The third PDSA on the ward was run by the ward pharmacist and junior doctor, and involved a pharmacist documenting a summary of relevant medication changes and medications for review in the patient’s notes, so this was highlighted to doctors at discharge. This was run 2 weeks after the third PDSA, and lasted for 1 week. We achieved an average compliance of 91% with this intervention. Feedback from doctors suggested it was useful to have other members of the MDT with more knowledge of particular issues (such as pharmacists in regards to medications) providing guidance on discharge summary completion.
We subsequently reduced the frequency of data collection to fortnightly due to sustained improvement. We performed a fourth PDSA 11 weeks later in order to ensure we sustained positive improvement. This was performed over 1 week and involved a repeat of the second PDSA in which patient feedback was obtained and shared at board round. We achieved an average compliance of 93% for that week, and subsequently reduced data collection to monthly intervals.
Results
Our main outcome measure was overall compliance with the 10 core elements that should be included in every discharge summary. Throughout the project, weekly data collection allowed us to rapidly assess changes in our data and determine their relation to individual PDSA cycles. We have seen data improvement with all of our PDSA cycles, which was sustained following our third PDSA cycle in November 2020, as demonstrated in figure 1.
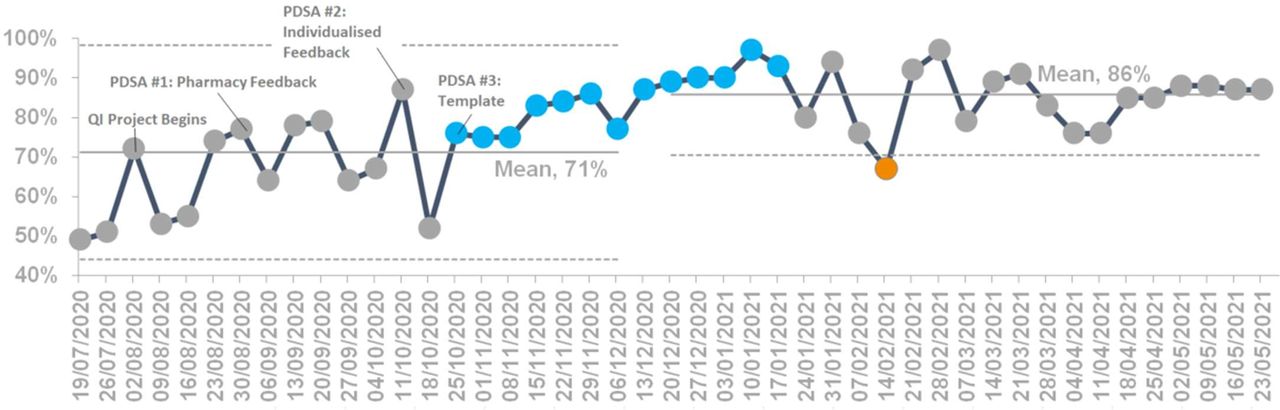
Discharge summary content: overall compliance (ward 22). PDSA, Plan, Do, Study, Act; QI, quality improvement.
On our first pilot ward, we reached 97% compliance in January 2021 from a baseline of 55%, 5 months ahead of schedule. This positive improvement was sustained over the following 5 months with an average compliance of 80% with minimal intervention. Due to consistently high compliance, we were able to decrease data collection over the last 2 months of the project and start measuring for assurance. The project on our initial pilot ward was completed in June 2021, and monthly assurance data were collected over the following 5-month period. Average compliance during this period was 85% without any further intervention, showing these changes had been successfully embedded.
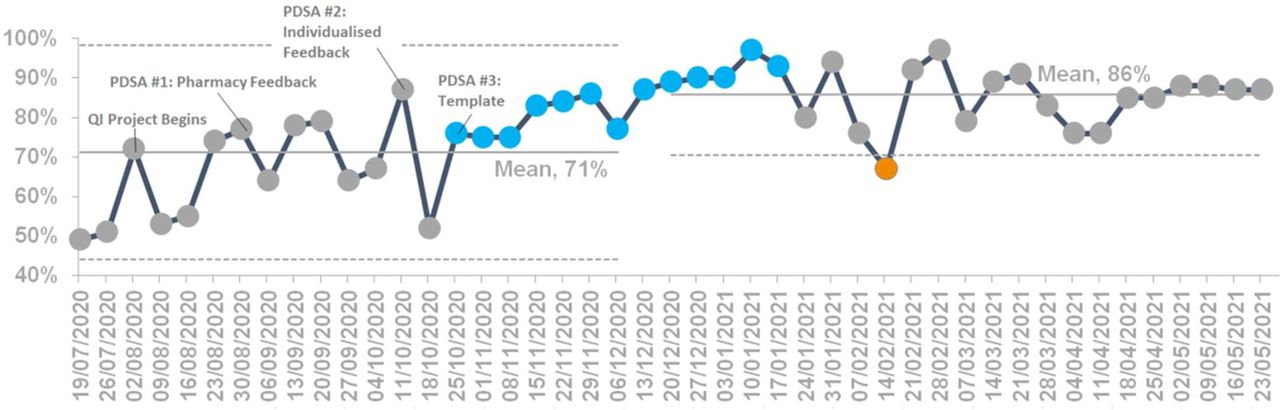
Our project expanded to a second pilot ward in the Trust in May 2021. Starting from a baseline average compliance of 61%, we have demonstrated improvement to 92% average compliance following our first PDSA on this ward in June 2021 as seen in figure 2. We have demonstrated significant improvement within 4 months of the project starting, evidenced by average discharge summary compliance increasing to 92% following the first PDSA, 91% following both the second and third PDSAs and 93% following our fourth PDSA. Mean compliance has increased and has been sustained at 86% as demonstrated in figure 2.

{kind=link}
{kind=link}
Discharge summary content: overall compliance (ward 2). PDSA, Plan, Do, Study, Act; QI, quality improvement.
From a subjective perspective, the pharmacy team reported that as summaries were now clearer, screening and review time of medications were improved within the hospital and the transfer of care to the community was more efficient. Junior doctors and physician associates have provided feedback that discharge summaries are easier and quicker to complete now due to the standardised approach. Due to the positive and sustained change that we demonstrated throughout this project, we have designed a standard operating procedure document and a third pilot in the paediatrics department has recently commenced.
Since the project began, there have been no PALS complaints or GP quality alerts raised relating to discharge summaries and their quality or content.
Lessons and limitations
This project has been successful in enacting meaningful change within the acute medicine system; however, it has highlighted certain challenges with implementing this improvement as set out below.
The strengths of this QI project specifically include the involvement of the MDT and value of patient co-design. Specific feedback from our patient representative stated ‘as a member of the QI project team, I have been able to share my experience and contribute ideas for improving the quality of discharge summaries. Patients and carers need to know what happened to them in hospital and why decisions were taken. A well-written, detailed discharge summary can support GPs and others to make future decisions that can potentially lead to better outcomes for patients’. MDT and patient-specific feedback has allowed us to demonstrate the importance of discharge summaries and encourage a behavioural change within our clinical staff.
Throughout this project, we have used QI methodology with MDT involvement to achieve a specific, measured, achievable and realistic aim, and we have demonstrated meaningful change that will positively impact on both patients and healthcare professionals in the community and hospital settings. We have celebrated the success of our work with colleagues at QI showcase presentations, Trust Board meetings and poster presentations at national and international level. This project has been excellent at demonstrating successful scale up and expansion to other pilot areas following sustained improvement.
The positives of this project did not come without a number of challenges. We were able to see that maintaining change can take time, in particular due to the constant rotation of staff within all areas of the NHS. While we had excellent feedback and responses from junior doctors, due to the 4–6 monthly nature of rotations, we have had to repeatedly raise awareness and reintroduce ideas to new staff rotating on to the wards. This challenge has been encountered in previous projects targeting discharge summaries.7 As mentioned, some PDSA cycles had positive results but were not able to be reproduced on a larger scale. Having a pharmacist present on medical ward rounds was beneficial to all members of the team, but due to staff shortages in the context of the COVID-19 pandemic, it was not able to be consistently trialled over a longer time period on our acute medical wards.
We have been able to demonstrate clearly what can happen when team members from different areas of the NHS come together to try and enact change, and how QI can be used to make a positive difference to patient outcomes and enhancing staff experience. Behavioural change has been key in this project. Clinicians are time pressured and encouraging them to dedicate time to discharge summaries requires a greater understanding of why they are important.
Conclusion
Discharge summaries are important pieces of medical documentation that are used by both healthcare professionals and patients to understand the events of a hospital admission, as well as ensure safe handover of care. Using structured QI methodology, with MDT involvement and a patient-centred approach, we have significantly improved the content and quality of discharge summaries on the acute medical wards in a sustainable manner. We hope that the improvement we have achieved with the implementation of a template for discharge summary completion will be expanded across the trust in the near future, with plans to change the electronic discharge system to include elements of this template.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The author would like to acknowledge the contributions from Reshma Chhana as our senior community pharmacist who helped ensure we were coordinated with community pharmacy teams and Kirsten Fernandes, ward pharmacist, who helped run plan–do–study–act cycles and drive the project forwards with specific pharmacy input.
Footnotes
PS and TDS are joint first authors.
Twitter @alexandrastrks
Contributors PS and TDS contributed equally to this paper so should be listed as joint first authors and both should be listed as guarantor. Both PS and TDS were project leaders for the initial and pilot quality improvement (QI) projects, respectively, designing and running the projects on the ward, presenting at local meetings to clinical and management teams, as well as analysing the data and writing this paper. CS was our QI coach throughout the project and helped write and edit this paper. AS was our QI data analyst who provided the data analysis for the project and made the control charts. SM was our patient representative who helped to codesign and run this project throughout. JL was our consultant sponsor of the project, helping to guide our work and engage senior members of the trust management to help us enact change. SK, BD, AM and EB were all team members responsible for weekly data collection, raising awareness of the project on the wards and running of individual plan–do–study–act cycles.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.