Article Text

Abstract
Background: Eosinophilic oesophagitis is a rarely diagnosed condition involving eosinophil infiltration of the oesophageal mucosa and creating significant symptoms of dysphagia. Failure to diagnose this disorder relates to reluctance to biopsy an apparently normal oesophagus. This is essential for histological diagnosis. To date, treatment success has been achieved only with corticosteroids. We describe here the use of an eosinophil stabilising agent Montelukast for the symptomatic relief of these patients.
Patients and methods: Twelve patients have been identified with this condition in our unit since 1995, after thorough investigation of their dysphagia. We commenced eight of these patients on the leukotriene receptor antagonist Montelukast to symptomatically improve their swallowing while avoiding the use of long term corticosteroids.
Results: Many of these patients had been previously misdiagnosed, and therefore inappropriately and unsuccessfully treated for an extensive period prior to referral to our unit. All patients were unresponsive to acid suppression therapy alone but showed improvement in their swallowing on Montelukast. Six of eight reported complete subjective improvement, five patients remaining completely asymptomatic on a maintenance regimen.
Conclusions: Eosinophilic oesophagitis is a disease that is often misdiagnosed due to lack of awareness and reluctance of clinicians to biopsy an apparently normal oesophagus in dysphagic patients, and therefore obtain a histological diagnosis. Investigation of these patients adds further evidence to this condition being a separate pathological state from gastro-oesophageal reflux and eosinophilic enteritis. Montelukast has been found to be of significant help in the symptomatic control of these patients while avoiding long term corticosteroids use.
- dysphagia
- eosinophil
- Montelukast
- oesophagitis
- EO, eosinophilic oesophagitis
- LTRA, leukotriene receptor antagonist
- GORD, gastro-oesophageal reflux disease
Statistics from Altmetric.com
- EO, eosinophilic oesophagitis
- LTRA, leukotriene receptor antagonist
- GORD, gastro-oesophageal reflux disease
Attwood et al called attention to eosinophilic oesophagitis (EO) as a distinct clinical condition in 1993. In this disease an intense eosinophilic infiltration is seen in the oesophagus of dysphagic patients.1 Previously, eosinophils in the oesophagus were regarded as an incidental component of gastro-oesophageal reflux disease2 or a variant of eosinophilic gastroenteritis.3,4 However, the distinct clinical syndrome of EO is not usually seen with either of these. Most recent literature refers to EO in children but the adult phenomenon may escape diagnosis due to lack of awareness of this as a separate pathology.1,5
The hallmark of this condition is intermittent and often painful dysphagia which may become constant as the disease progresses. Thorough investigations often show essentially normal or mildly abnormal oesophageal endoscopy, pH, and manometry studies which are not consistent with the severity of symptoms described. Mechanical obstruction is usually absent and, unless a biopsy is taken, these patients are found to be a diagnostic and management enigma.1
Management of these patients has been made difficult due to diagnostic problems and a poor understanding of the disease pathogenesis. Acid suppression has no effect despite the theory that this condition is secondary to gastro-oesophageal reflux.2 Antihistamine medications have been used but with no reported success. Oesophageal dilatation has been undertaken for purely symptomatic relief but unfortunately this can be very uncomfortable and provides only short term relief.1 Corticosteroid therapy has been described with some success. 5,6 However, symptoms soon relapse after ceasing therapy, and the significant side effect profile of long term steroid therapy greatly limits their value in this setting.5
In the paediatric setting, this condition is far more widely recognised. The standard therapy regimens consist of an elimination diet and corticosteroids.7 However, this is an arduous undertaking and would probably be unacceptable to the adult population.
A recent case report by Schwartz and colleagues8 describes the use of Montelukast (Singulair; Merck Sharp and Dohme Ltd, UK) in the treatment of steroid dependent eosinophilic gastroenteritis. Montelukast is a leukotriene receptor antagonist (LTRA) which actively and selectively blocks the leukotriene D4 receptor.9 It was originally licensed as a cysteinyl leukotriene antagonist for use in asthma. We have been using Montelukast in the treatment of EO in a similar way for some years. This report describes our clinical experience of patients with EO treated in this way.
MATERIALS AND METHODS
Since 1995 we have identified 12 patients referred to our unit with EO. Until the advent of Montelukast, and its wide availability in 1998, a variety of treatment regimens had been tried with differing success. Treatment of these patients was primarily adjusted according to the severity of symptoms. Those with mild symptoms were commenced on either cinnarizine (Stugeron; Janssen-Cilag Ltd, UK) 15–30 mg three times daily or sodium cromoglycate (Nalcrom; Pantheon Healthcare Ltd, UK) 200 mg four times daily. Patients with more severe symptoms were commenced on oral corticosteroid therapy and showed significant symptom relief. One of three patients showed significant improvement on cinnarizine. One patient’s symptoms spontaneously resolved while another was helped by myotomy.10
Patients who previously showed improvement in symptoms with steroids and those with poor relief from other regimens were commenced on Montelukast in an attempt at symptom control without the need for long term corticosteroid therapy.
Investigation of patients with EO was standardised. Each patient underwent oesophagogastroduodenoscopy (Fujinon Series EG410-HR and EG410D gastroscopes; Fujinon Inc. USA) and multiple biopsies using the 2.2 mm Boston Scientific Microvasive Radial Jaw 3 with Needle (Boston Scientific Intl, France), both at diagnosis and again 4–9 months following commencement of Montelukast. All were performed following fully informed consent under sedation using 4–8 mg midazolam (Hypnovel; Roche Products Ltd, UK). Formalin fixed biopsies were then processed in paraffin sections, stained with haematoxylin and eosin, and examined under high power view (×40: field area 0.166 mm2) in random orientation by a single pathologist.
Manometry and pH studies were undertaken on all patients to identify any motility disorders or reflux. Stationary manometry was performed using a five channel solid state catheter (Gaeltec Ltd, Scotland, UK), while 24 hour pH was measured 5 cm above the lower oesophageal sphincter using an antimony electrode on a single channel probe (Medtronic Functional Diagnostics, Denmark) and recorded on a Digitrapper III (Synectics Medical, Sweden). Acid exposure and DeMeester score were then calculated on Gastrosoft computer software (Gastrosoft Inc., USA). Bile reflux was tested in one patient using Bilitec 2000 (Synectics Medical).
The dose was adjusted according to tolerance and symptoms. Initial treatment was with Montelukast 10 mg daily but was increased if required up to a total of 100 mg daily. This starting dose was the same as that used for patients with severe asthma in hospital. Once symptom relief had been achieved, the dose was then reduced to maintenance levels where symptom control was retained. In all patients this was between a total dose of 20 mg and 40 mg/day.
Patients
Median age of patients with EO was 40 years (range 22–64; interquartile range 35–55). Onset of symptoms was at a median age of 33 years (range 15–62). Median length of time patients had symptoms prior to referral to our unit was 36 months (range six months to 18 years) (table 1). Eight patients were referred directly from gastroenterologists, one from a neurologist, one from a cardiothoracic surgeon, and two from general practice. Two patients had also seen ear, nose, and throat surgeons prior to attending our department.
Patient characteristics
All patients presented with dysphagia as their primary symptom. They did however have a variety of other symptoms, notably odynophagia in seven patients, and a further potential allergic disorder in six (table 2).
Patient symptoms and previous investigations
At referral, nine patients had previously had a flexible gastroscopy, two of these had also had rigid oesophagoscopy, and three had undergone a barium swallow. The diagnoses given at referral were oesophageal dysmotility in one patient, acid or alkali reflux with or without stricture in six patients, and suspected oesophageal carcinoma in another (table 1).
RESULTS
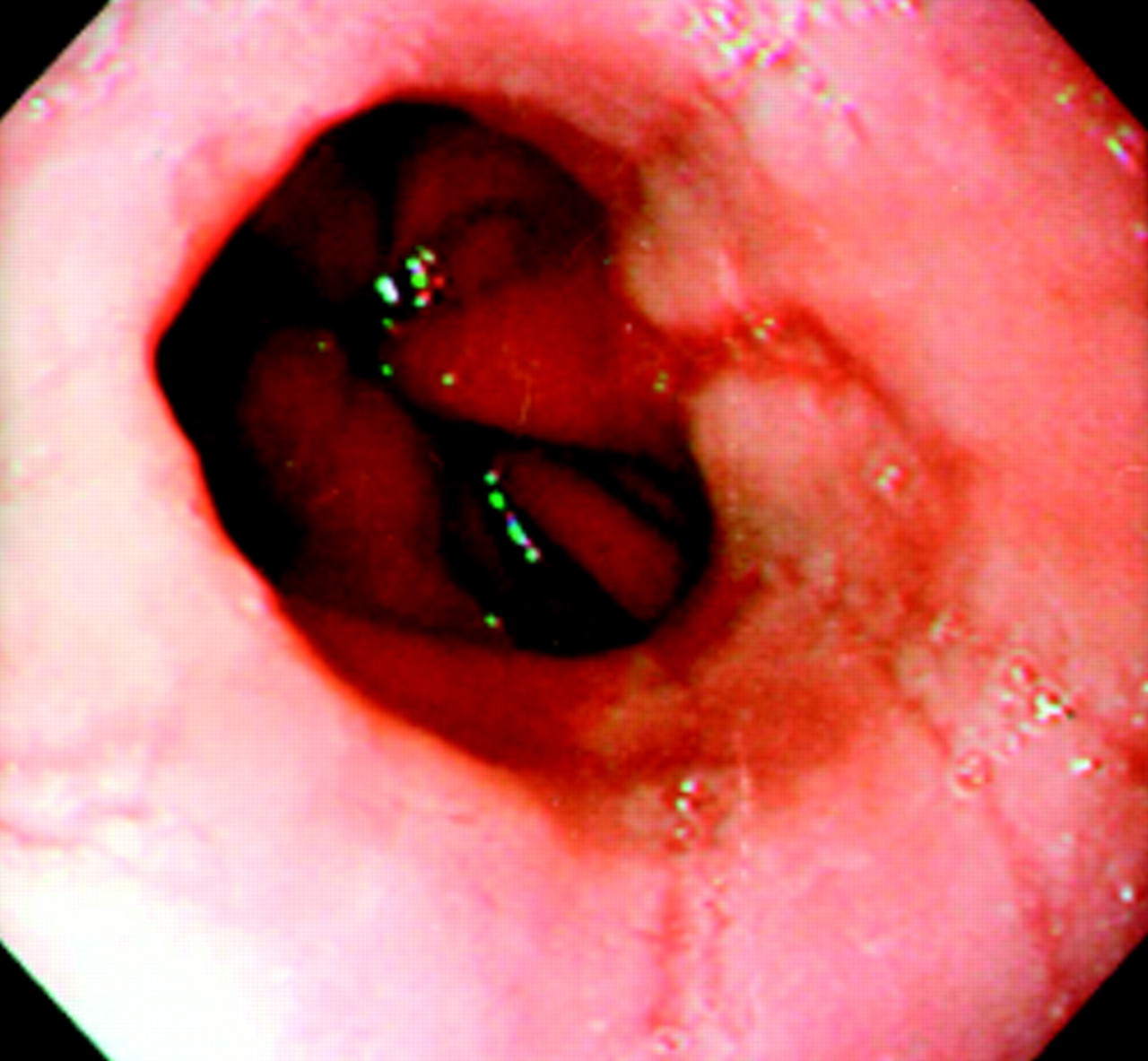
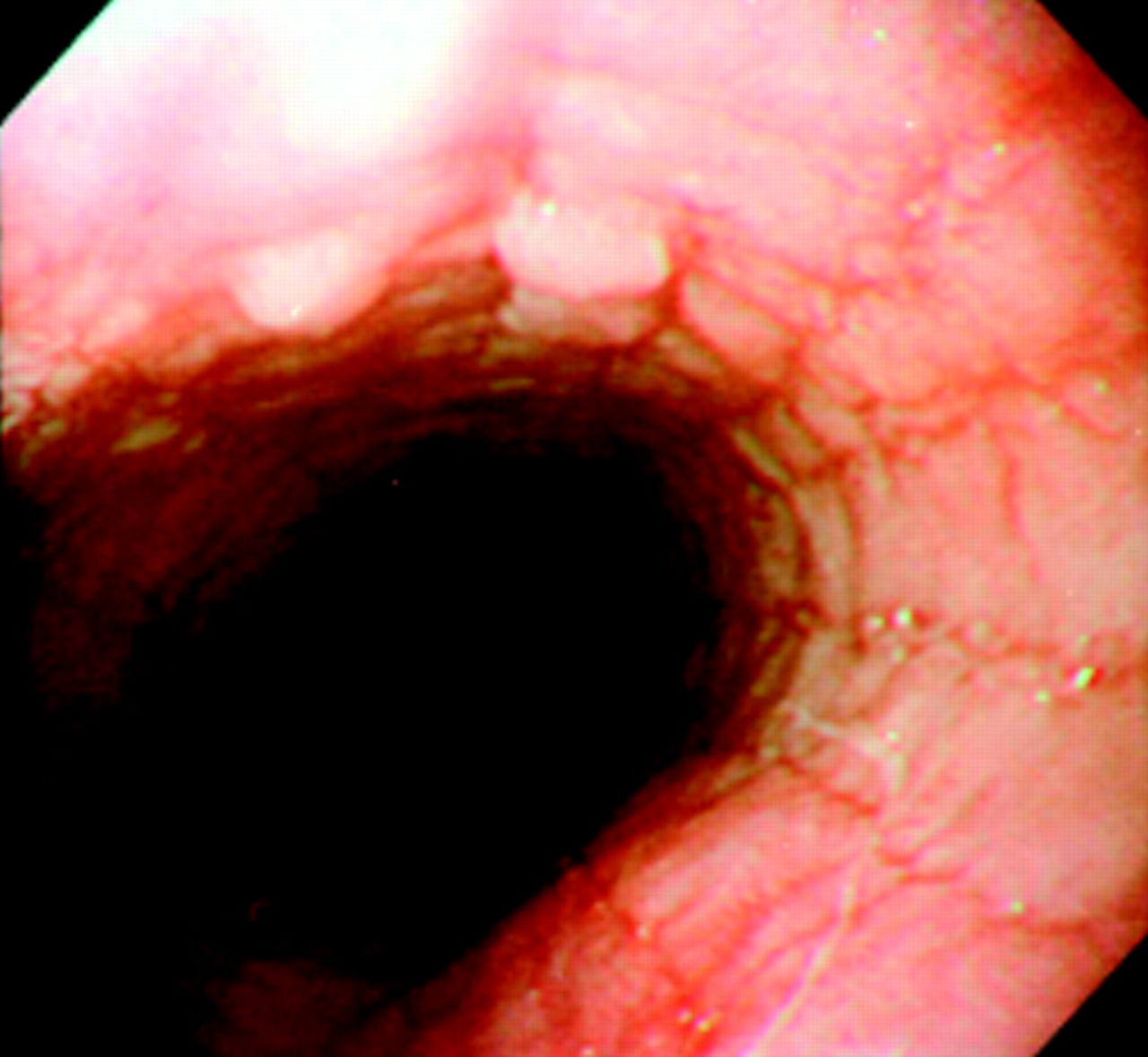
A specific pattern of mucosal change was observed at endoscopy in nine patients. Two patients had concentric rings (fig 1) and four had linear furrows (fig 2) in the mucosa. In three patients there were both furrows and rings, creating a cobblestone effect (fig 3). Two patients had a macroscopically normal oesophagus while one was seen to have apparent extrinsic compression caused by an intramural leiomyoma.

Endoscopic view of a dysphagic patient with eosinophilic oesophagitis, illustrating clearly a concentric ring pattern.
Endoscopic view of a dysphagic patient with eosinophilic oesophagitis, illustrating linear furrows.
{kind=link}
{kind=link}
{kind=link}
Combination of furrows and rings creating a cobblestone effect seen in eosinophilic oesophagitis at endoscopy.
Biopsies were examined and formal eosinophil counts were taken using an eyepiece graticule. From this an eosinophil density per mm2 was calculated. Median density of eosinophils was 342.5/mm2 (range 115–871.3), equivalent to 56.9 per high power field. All eosinophils were concentrated in the intraepithelial layer except for one patient who had eosinophils present in the muscle layer but had few in the intraepithelial layer (20.3 per mm2). This patient had a myotomy and a biopsy which was taken at thoracotomy. All of the remaining patients had endoscopic biopsies and therefore no information on eosinophil infiltration of the muscle layer was available. On inspection of the biopsy slides it was evident that eosinophil infiltration was non-uniform. There was marked variation within each section, and microabscesses were also present in the intraepithelial layer. Treatment with Montelukast for more than four months did not change the density of eosinophils.
pH and manometry studies showed that all but one patient had no evidence of reflux, with median DeMeester scores of 7.4 (range 0.9–10), median oesophageal exposure time to a pH <4 of 1.5% (range 0.3–2.6%), and a median lower oesophageal sphincter barrier pressure of 20 mm Hg (range 5–39). One patient presented with significant reflux and a Schatzki ring, which required dilatation. His DeMeester score was 20; the time for oesophageal acid exposure was 5.9%, and his lower oesophageal sphincter pressure was 9 mm Hg. This patient appeared to have dual pathologies, which was evident when he required acid suppression therapy, in addition to Montelukast, for symptom control.
Eight patients have been commenced on Montelukast. Two had previously responded to corticosteroids but were reluctant to remain on this therapy for the long term. Every patient had been treated with a proton pump inhibitor previously, and two with a combination of antihistamines and motility agents (table 3), all without success. Cessation of the acid suppression therapy showed no detrimental effect in 11 of 12 patients. Montelukast has restored a comfortable swallow in all those treated, except for two patients who still have some residual discomfort despite experiencing improved symptomatology.
Treatment results
Montelukast was tolerated well at 30 mg daily but five patients required an increased dose. Seven of the eight showed complete subjective improvement in dysphagia symptoms with a maintenance dose of 20–40 mg daily. The eighth had moderate improvement at 30 mg but could not tolerate the 40 mg dose due to myalgia and nausea. He did however choose to remain on the medication (table 3).
These patients have now been treated with Montelukast for a median of 14 months (range 4–28). No relapse of symptoms has been described while continuing on the medication but six patients have had recurrence within three weeks of cessation or reduction in medication. Three patients still experience other symptoms occasionally, such as odynophagia. Several side effects were documented, most notably nausea in four patients and myalgia in one, but there was a significant subjective improvement throughout the group. Of this series of patients, eight remain on Montelukast, one is still on cinnarizine, and three require no further medication. One has undergone surgery and has been reported on previously.10
DISCUSSION
Eosinophilic oesophagitis is a distressing condition of dysphagia which responds well to Montelukast. The difficulties related to diagnosis are primarily due to failure to appreciate subtle mucosal changes at endoscopy and therefore failure to biopsy where no significant pathology is visualised. EO is only identified histologically using oesophageal biopsies where high densities of eosinophils (>20/high powered field) are found infiltrating the mucosa.1 From our group of patients it is also clear that there is still a significant problem with the diagnosis of EO. Median time from onset to diagnosis was 33 months, which should be improved with greater understanding and awareness of this separate disease entity.
The aetiology of EO is not fully understood. It has been theorised that infiltration of eosinophils into the oesophageal mucosa is the oesophageal manifestation of allergic eosinophilic gastroenteritis,3,4 or is this condition associated with reflux disease?2 Although response to steroids has been reported to be significant in some patients, as it was in our patient group, they do not manifest any other signs or symptoms of eosinophilic gastroenteritis, suggesting that the two pathologies may not be linked, as previously suggested.3,4 It is also very clear that these patients do not respond well to acid suppression therapy and that histological and endoscopic findings, although similar, are not completely consistent with the reflux aetiology postulated by Lee.2
Reflux as a causative mechanism is still a widely held belief. Morrow et al’s11 paper postulated the disease phenomenon of so-called “ringed oesophagus” as primarily a result of gastro-oesophageal reflux disease (GORD). This ringed oesophagus, by definition, has all the hallmarks of EO. The connection between the two supposedly different pathologies has not been made as pH/manometry studies showed GORD in only two patients in their study.11 In their series of 19 patients, all presented in the same way as our group, with progressive dysphagia. Half of the patients had onset in the same age range and all had concentric rings, very similar to those found in five patients from our group with proven EO. Only 11 patients had available biopsies from endoscopy, highlighting the lack of routine biopsy of all patients with dysphagia of unknown cause. All showed significant infiltration of eosinophils but quantitative measurements were omitted from the results. In our study only one patient was shown to have significant acid exposure on 24 hour monitoring. In their paper, Morrow et al treated a single patient with corticosteroids. The patient made a significant improvement, as would be expected in a patient with EO. The remainder however were treated with repeated and often painful dilatation along with acid suppression. Somewhat surprisingly they report subjective improvement in symptoms despite unproved reflux and even absence of reflux symptomatology in nearly 50% of patients. Morrow et al conclude by advocating repeat dilatation and acid suppression therapy in a patient group with identical presentation and similar histological findings to our own, a view we do not from our experience share.
Of our patients, only 50% had a history of atopy (table 1).5 Similarly, there was no improvement with the use of antihistamines in the treatment of symptoms, except in one patient, which suggests a different pathogenesis from an allergenic cause. Our patients showed no symptoms as young children. The onset of the disease appeared on the whole later in life, implicating a separate pathological state than the more widely reported paediatric EO. This again is attributed to reflux disease in the main which does not fit our patient group.6,7
The difficulty of diagnosis through lack of biopsy has caused one of our patients to be referred to a psychiatrist for what the clinician believed to be a psychogenic disorder. A second patient’s dysphagia was thought to be a manifestation of his severe depression, and was again referred to a psychiatrist. These patients have been discharged from the care of the mental health team following confirmed true diagnosis, and have returned to normal social function.
It is clear that this pilot use of Montelukast for the symptomatic treatment of EO shows that there is an effective treatment and an alternative to long term corticosteroid therapy. Montelukast selectively blocks the D4 receptor of cysteinyl leukotrienes present in eosinophils. All cysteinyl leukotrienes are arachidonic acid derived inflammatory mediators,12 which are important in asthma.13 The actions of leukotrienes include: eosinophil attraction and migration, powerful constriction of smooth muscle, airway oedema, mucous hypersecretion, and reduction in ciliary motility.3,4 They are predominantly released by eosinophils, basophils, and mast cells.14,15 By blocking the D4 receptor the inflammatory action of the eosinophil cell is reduced. Eosinophils are not removed, there actions are simply negated, which was clearly seen in our repeated biopsy results.
Three published randomised control trials of Montelukast, for both chronic and exercise induced asthma, have shown significance in either symptom improvement or reduction in the requirement of other therapies, such as corticosteroids.16–18 The current guidelines allow Montelukast and other LTRAs to be used in asthma that is difficult to control, despite the use of corticosteroids, and not as firstline therapy.19
In conclusion, we have introduced a new potential treatment for EO. The study highlights the problems of diagnosis and lack of awareness and understanding of the aetiology and pathogenesis of the disease, and produces new evidence to refute the claims that this is a pathological state caused by gastro-oesophageal reflux or atopy. The use of Montelukast in this instance showed improvement of symptoms, although subjective, throughout the group. However, we have treated only a small number of patients and further randomised control trials, using this as a pilot study, are required to assess the full benefits of Montelukast in this condition. We stress the importance of oesophageal biopsies in all patients with dysphagia. This should be part of the standard protocol for investigation of these patients and the only way that the diagnosis of EO can be made.