Article Text

Abstract
Introduction Racial disparities in cancer treatment contribute to racial disparities in mortality rates. The quality of patient–physician communication during clinical interactions with black patients and non-black physicians (racially discordant) is poorer than communication quality with white patients (racially concordant). Patient and physician race-related attitudes affect the quality of this communication. These attitudes are likely expressed through subtle non-verbal behaviours, but prior research has not examined these behaviours. Nonverbal synchrony, the coordination of physical movement, reflects the preinteraction attitudes of participants in interactions and predicts their postinteraction perceptions of and affect towards one another. In this study, peer reviewed and funded by the National Institute of Minority Health and Health Disparities (R21MD011766), we will investigate non-verbal synchrony in racially concordant and discordant interactions to better understand racial disparities in clinical communication.
Methods and analysis This secondary analysis includes racially concordant (n=163) and racially discordant (n=68) video-recorded oncology interactions, patient and oncologist self-reported race-related attitudes, perceptions of the interaction and observer ratings of physician patient-centred communication and patient and physician affect and rapport. In aim 1, we will assess and compare non-verbal synchrony between physicians and patients in racially concordant and discordant interactions. In aim 2, we will determine the influence of non-verbal synchrony on patient and physician affect and communication. In aim 3, we will examine possible causes (ie, race-related attitudes) and consequences (ie, negative perceptions) of non-verbal synchrony in racially discordant interactions. In aim 4, we will develop and test a mediational model linking physician and patient race-related attitudes to non-verbal synchrony and, in turn, interaction outcomes.
Ethics and dissemination The parent and current studies were approved by the Wayne State University Institutional Review Board. Since only archival data will be used, ethical or safety risks are low. We will disseminate our findings to relevant conferences and journals.
- disparities
- cancer
- racial discordance
- nonverbal synchrony
- race-related attitudes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study explores non-verbal synchrony, a channel of communication that has not been previously examined in medical interactions.
This study uses video-recorded cancer treatment discussions of black and white patients with cancer, recorded with state-of-art recording equipment.
This study uses automated behavioural coding software, which introduces less error than traditional methods using human coders.
This study takes advantage of existing datasets, but the video-recorded and self-report data were not collected with the current hypotheses in mind.
The data are not evenly distributed by sex and race.
Introduction
Racial disparities in cancer mortality and treatment are well documented. In the USA, deaths due to cancer are approximately 20% higher for black patients than for white patients.1 This mortality disparity remains even after controlling for stage at diagnosis, disease aggressiveness, obesity, comorbidities, physician access, insurance status and referrals.2–6 Importantly, this disparity is greatest for the most treatable cancers.7 This strongly suggests treatment disparities may contribute to mortality disparities.8–14 For example, black patients with cancer are less likely to receive chemotherapy for leukaemia, breast, lung and colorectal cancers. If they do receive treatment, it is more likely to be delayed or not adherent to the treatment guidelines set by the National Comprehensive Cancer Network.2 8 15–23 Multiple causes of these treatment disparities exist including tumour biology, socioeconomic status, environment and access to care.6 However, research clearly shows that even when these factors are controlled, racial disparities in treatment remain. We focus on two other contributors to racial disparities in cancer treatments: (1) poor patient–physician communication during oncology interactions24–30 and (2) race-related attitudes and perceptions of physicians and patients.31–42 We are investigating these factors because they account for unique variance in racial treatment disparities.
Black patients experience poorer quality communication during oncology interactions compared with similar interactions with white patients. Due to the small number of black physicians, especially black oncologists,43 about 80% of black patients’ clinical interactions are racially discordant (black patients, non-black physicians).44 Patient–physician communication is often of poorer quality in racially discordant clinical interactions than racially concordant ones. Patients in racially discordant interactions tend to ask fewer questions25 and are less likely to participate in decision-making45; whereas physicians tend to be less patient centred,46 47 more verbally dominant,47 more contentious,48 exhibit fewer rapport building non-verbal behaviours49 and provide less information.27 Physicians and patients show fewer expressions of positive affect47 and relationship-building attempts.29
Patient and physician race-related attitudes and perceptions affect interaction outcomes via communication behaviours. Prior research, including our own, suggests that race-related attitudes and perceptions (eg, physician implicit bias against black people, patient suspicion of medical care black people receive) affect communication in clinical interactions and perceptions physicians and patients have of each other during racially discordant clinical interactions.31–33 37 38 For example, physicians with higher levels of implicit (unconscious) bias against black people are perceived as less patient centred and less trustworthy by their black patients than physicians with lower levels of implicit bias against black people.31 40 41 50 Our prior research suggests such perceptions and behaviours are associated with less positive patient expectations about recommended treatments.51 We have also found that black patients with higher levels of suspicion of medical care are less optimistic about outcomes of recommended treatments and are perceived by their physicians to be less educated.52 This, in turn, is associated with less positive physician expectations about how their black patients will do on a treatment protocol, such as their adherence and/or ability to tolerate treatment. Given that these attitudes and perceptions are not directly observable, the only possible way in which they can affect perceptions and expectations is through their influence on communication behaviours.
Relatively little is known about how race-related attitudes and perceptions are manifested in communication behaviours during oncology interactions or the effects of communication on interaction outcomes. Our own and others’ research has shown that non-black physicians’ unconscious race-related attitudes (ie, implicit racial bias) influence their communication with black patients.51 53 54 Studies of non-medical interracial interactions find that implicit bias is more likely to be expressed through less deliberate non-verbal communication (eg, facial expressions, posture) than through more deliberate verbal communication (eg, spoken words).55–58 Black patients’ communication may be driven more by explicit than implicit race-related attitudes and perceptions,59 but its expression may also be subtle and involve less deliberate communication (eg, non-verbal behaviours).54 The behavioural channels through which these race-related attitudes and perceptions are expressed are not known, but non-verbal synchrony is a promising candidate as one of them.
Non-verbal synchrony is the coordination of physical movement that occurs between two individuals during an interaction.60 The construct of synchrony was first introduced more than 50 years ago and has sparked many related areas of study.61 Here, we consider non-verbal synchrony as a dynamic and jointly determined phenomenon, not focused on any particular behaviour (eg, posture, eye contact). Rather, we consider non-verbal synchrony as a form of behavioural matching between two individuals. This matching does not have to occur at the same time (as it would for two people dancing), but it must involve similar kinds of motion and exhibit some sort of coordinated back and forth between individuals.62–64 As an example, an individual shaking his or her head while another individual waves his or her hand would exhibit non-verbal synchrony but they are not mirroring one another nor are they perfectly in time.63
Considerable prior laboratory-based research shows that non-verbal synchrony is often unconscious, unintentional and effortless.65–67 However, non-verbal synchrony can be predicted by preinteraction attitudes68 and has postinteraction consequences.69 People synchronise more with others with whom they have positive relationships,70 those with whom they want to develop positive relationships71 and others whom they trust.68 In a recent experimental laboratory-based study, individuals with higher implicit bias favouring their own race synchronised more with an avatar of their own race than with an avatar of a different race.72 In terms of non-verbal synchrony’s role as a predictor, non-verbal synchrony reflects more subsequent positive affect and liking,69 perceptions of similarity, closeness, rapport with the interaction partner and collaborative problem solving.68 73–75 More relevant to clinical communication, non-verbal synchrony has been found to positively influence therapeutic processes,76 cooperation,77 obedience74 and memory for information provided by the interaction partner.78 79 It is because of this previous research that we will investigate general non-verbal synchrony in this study, rather than, for example, vocal synchrony or synchrony of more precise behaviours such as eye gaze.
To summarise, current evidence indicates that black patients and non-black physicians have negative reactions to each other’s race-related attitudes and perceptions. Also, evidence indicates that these attitudes and perceptions are subtly manifested in communication. Little is known, however, about the channels through which these attitudes and perceptions are communicated. Because non-verbal synchrony is subtle, unintentional, automatic and affect-laden, it may likely serve as a behavioural marker of race-related attitudes and perceptions. Here, we describe the protocol for a study that will help fill this gap in understanding by examining the role of non-verbal synchrony in racially concordant and racially discordant oncology interactions.
The study was designed to achieve the following aims and hypotheses, which are based on the research reviewed:
Aim 1: Assess and compare non-verbal synchrony between physicians and patients in racially concordant and racially discordant oncology interactions.
Hypothesis 1: Non-verbal synchrony will be greater in racially concordant than in racially discordant oncology interactions.
Aim 2: Determine the influence of non-verbal synchrony on physician communication (eg, level of patient-centredness) and patient and physician affect in racially concordant and racially discordant oncology interactions.
Hypothesis 2: Non-verbal synchrony will positively influence physician patient-centred communication, patient and physician affect, and relational rapport in racially concordant and racially discordant clinical interactions.
Aim 3: Examine the antecedents and outcomes of non-verbal synchrony in racially discordant oncology interactions.
Hypothesis 3: In racially discordant oncology interactions, non-verbal synchrony will significantly negatively covary with patient postinteraction distress and positively covary with (1) patient postinteraction perceptions of physicians’ patient-centred communication and treatment expectations; (2) physicians’ postinteraction perceptions of patient personal characteristics (eg, understanding of treatment options) and their responses to treatment (eg, willingness to follow treatment regimen) and (3) observers’ ratings of physician patient-centred communication, patient and physician affect, and relational rapport.
Hypothesis 4: Non-verbal synchrony will significantly covary with preinteraction race-related attitudes and perceptions of the patient and physicians (eg, physician implicit bias; patient suspicion).
Aim 4: Develop and test a mediational model that links physician and patient race-related attitudes and perceptions to non-verbal synchrony and, in turn, outcomes of racially discordant oncology interactions.
Hypothesis 5: Non-verbal synchrony will mediate the relationship between preinteraction race-related attitudes and perceptions and postinteraction perceptions of the patients and physicians.
Methods and analysis
Overview of proposed study
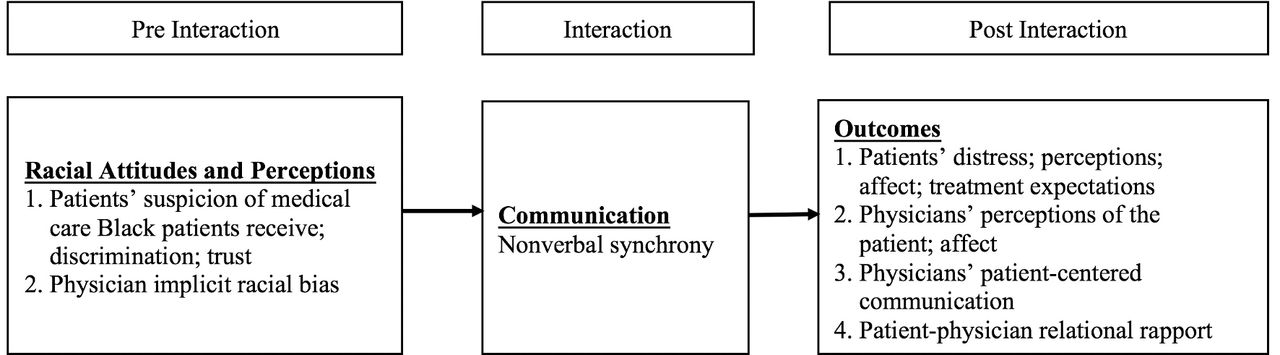
Our goals are to: (1) compare the extent to which physicians and patients synchronise their behaviour in racially concordant and racially discordant oncology interactions; (2) compare the associations between non-verbal synchrony and self-report and observational measures of patient and physician affect and physicians’ patient-centred communication in racially concordant and racially discordant oncology interactions; (3) investigate how race-related attitudes and perceptions (eg, physician implicit bias, patient suspicion) affect non-verbal synchrony in racially discordant oncology interactions; (4) investigate how non-verbal synchrony affects the outcomes of racially discordant clinical interactions and (5) test the conceptual model in figure 1, which predicts that race-related attitudes and perceptions will be associated with patient and physician perceptions and treatment-related outcomes of racially discordant oncology interactions, through their influence on non-verbal synchrony. To achieve these goals, we will conduct a secondary analysis of data from two studies conducted by members of our study team. This secondary analysis was officially funded in September 2017. Thus, it is ongoing and will be completed by August 2019. Study 1, which was funded by the National Cancer Institute (NCI), was conducted at two NCI-designated comprehensive cancer centres between April 2002 and March 2006 (R01CA75003),80 was an investigation of how patient–oncologist communication influences patients’ decision-making about treatment including clinical trials. Study 2 (also funded by the NCI) was conducted at one of the study 1 NCI-designated centres plus another large urban cancer clinic in the same city between April 2012 and December 2014. Study 2 investigated associations between communication and outcomes during racially discordant oncology interactions (U54CA153606-04).81 Only patients and oncologists from these studies who agreed on their consent forms to allow their video-recorded and self-reported data to be used in secondary analyses will be used in the current study. Comparisons of groups did not find any sociodemographic or attitudinal differences between patients/oncologists who did and did not agree to be in secondary analyses.

Conceptual model.
Data sources
Participants, procedures and measures in study 1
Patients from study 1 who are in the current study include 163 self-identified White (92 male; 71 female) patients who were meeting with a white medical oncologist for the first time to discuss treatment for their cancer. On consent, which occurred immediately prior to meeting their oncologist, patients completed a survey assessing their sociodemographic characteristics. Oncologists were 22 white male medical oncologists (no female oncologists participated in study 1) who saw at least one participating patient (M=7.4, SD=7.0). On consent, oncologists completed a demographic survey. Examination rooms were equipped with unobtrusive digital audio and video recording devices. Studies have demonstrated the non-reactance to the recording process,82 and enhanced validity compared with audio recording alone.83
Participants, procedures and measures in study 2
Patients from study 2 who are in the current study include 68 black female patients who were meeting with a non-black medical oncologist for the time to discuss treatment for their cancer. While patients were recruited for study Two irrespective of sex, only six of the patients who enrolled were males. A meaningful statistical comparison on the variables of interest by patient sex cannot be conducted with so few male participants. Thus, we are excluding them from further analyses. On consent, patients provided sociodemographic information and completed measures of suspicion of medical care black patients receive34 and trust in medical institutions.84 There were 16 medical oncologists (7 females; 9 males; 8 white; 6 Asian/Pacific Islander; 2 Arab/Middle Eastern) who saw at least one participating patient (M=5.2, SD=6.4). On consent, oncologists completed a demographic survey and the implicit association test, which assesses implicit racial bias against black people.85 Just as in study 1, examination rooms in study 2 were equipped with unobtrusive digital audio and video recording devices.
In study 2, oncologists were consented on enrolment, and the video-recorded clinical interactions took place within 2 weeks after patients consented. Immediately after the interactions, patients completed measures of distress,86 perception of the physicians’ patient-centred communication87 and expectations about recommended treatment. Also, immediately after interactions, oncologists completed measures of perceptions of the patient and how well the patient would do in treatment. One week later, patients reported their level of trust in their oncologist84 in a telephone survey. Trained observers later observed and rated video-recorded interactions to assess physicians’ patient-centred communication.48 To do this, coders applied a global scale of physicians’ patient-centred communication which assessed physicians’ informativeness (eg, ‘the doctor thoroughly explained everything to the patient’); supportiveness (eg, ‘the doctor made the patient feel completely at ease during the consultation’) and partnership building (eg, ‘the doctor encouraged the patient to express concerns and worries’).48 At least two observers rated physicians’ patient-centred communication (three observers rated 15% of interactions to ensure continued reliability); inter-rater reliability was acceptable (intraclass correlation coefficient=0.57–0.74, p<0.05). Each physician’s patient-centred communication score was the average of observer ratings.
Five 1 min video slices were created from each of the recordings from the two studies (n=340 slices) by dividing each video recording into five equal segments and selecting the first minute from each segment.55 88–90 The slices were observed and rated by naïve observers who had no training other than instructions to provide their ratings for patient and physician affect (eg, warm/friendly) and relational rapport (eg, attentive). The use of naïve observers is consistent with this type of methodology.55 88
Hypotheses and data analysis
Aim 1: assess and compare non-verbal synchrony between physicians and patients in racially concordant and racially discordant oncology interactions
We will achieve this aim by first matching video recordings from study 1 and study 2 on patient and physician sex and other sociodemographics. Although our focus is on racial concordance/discordance, prior research suggests that patient and physician sex affects communication in medical interactions.91–95 However, as described above, matching on sex is constrained by the distributions in the original recordings. Thus, from study 1, we will use 71 white female patients and 92 white male patients who interacted with White male physicians. From study 2, we will use the 34 black female patient/non-black male physician dyads and 34 black female patient/non-black female physician dyads. Thus, within race concordant and race discordant interactions, we will examine the effects of sex concordance and discordance. We acknowledge that this is not a full factorial design, but it will permit us to examine the influence of race concordance/discordance on non-verbal synchrony and, also partially examine whether the influence of race on non-verbal synchrony is moderated by patient and physician sex. To minimise any other differences between black patients and white patients, we will also do block matching of patients from study 1 with patients from study 2 on characteristics that might affect non-verbal communication (eg, age, type of cancer). We expect this matching will reduce the number of patients available from study 1 by 20%–30%, but sufficient cases will be available for well-powered analyses of racial concordance/discordance. We will then further the equivalence of patients with advanced methods of propensity scoring.96–98
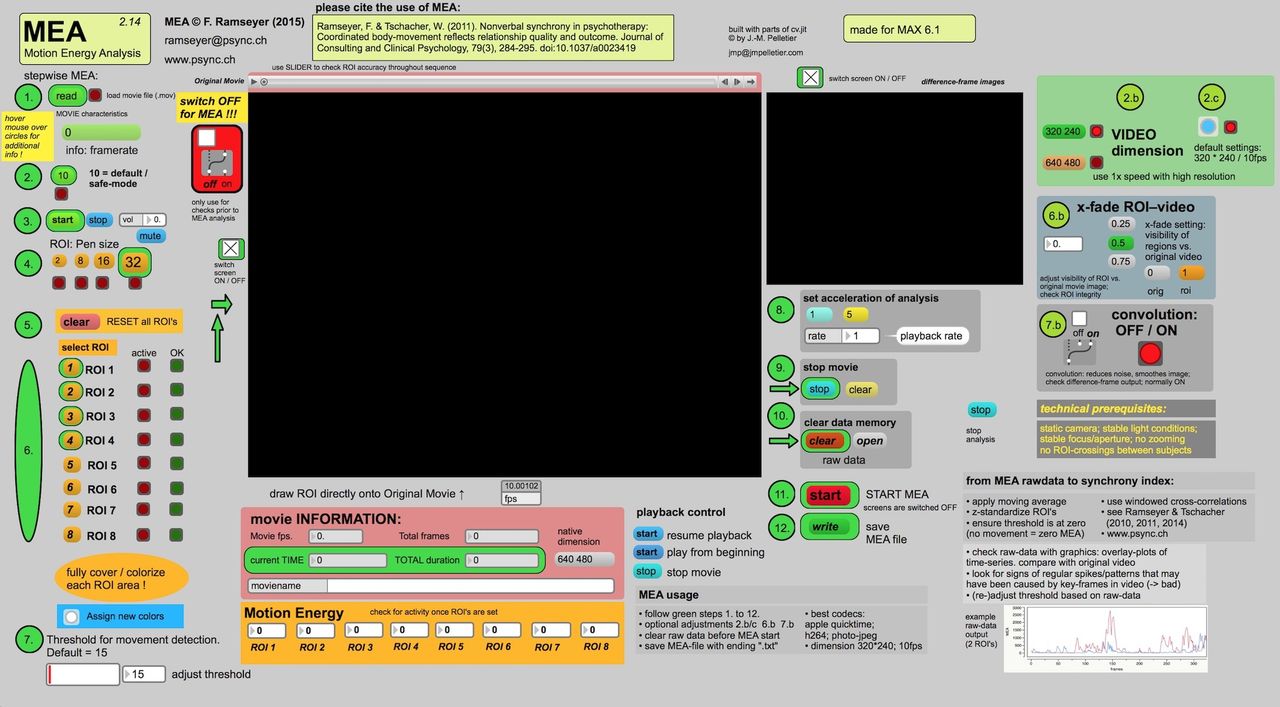
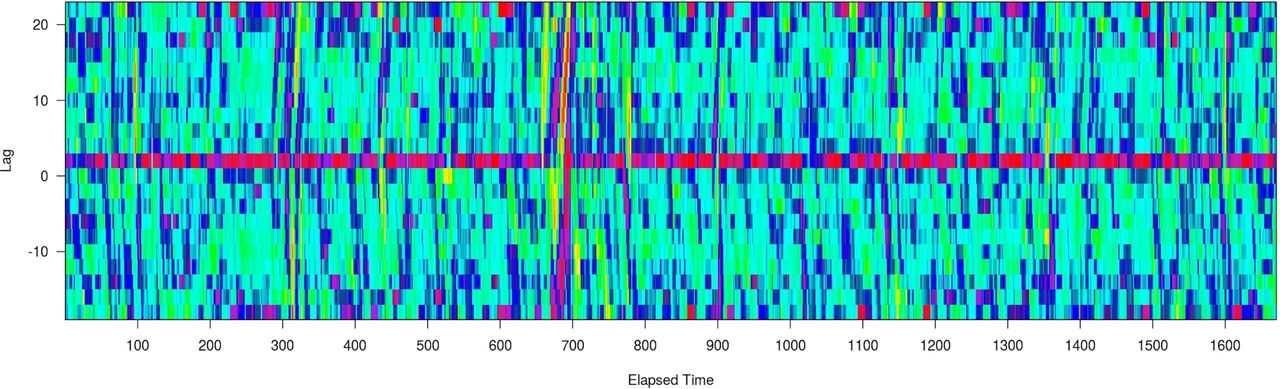
We will assess non-verbal synchrony in all matched interactions using customised Motion Energy Analysis (http://psync.ch/?p=9)76 99 software to obtain synchrony scores for each interaction. Figure 2 is a screenshot of the Motion Energy Analysis software. Motion Energy Analysis is an objective automated method that continuously monitors the amount of movement occurring in predefined regions of interest.62 76 100 Motion Energy Analysis captures frame-by-frame movement and provides quantification of change in movement in the ‘regions of interest’. In this study, we consider each individual as one ‘region of interest,’ allowing us to capture full body movement. Motion Energy Analysis uses pixel-differencing methods to measure total amount of movement. We will quantify non-verbal synchrony by deriving scores using windowed cross-correlation matrices to obtain synchrony scores for each interaction.101 Non-verbal synchrony tends to ebb and flow during conversations.91 Windowed cross-correlation accounts for the possibility of changing synchronisation by comparing small sections of time at different time lags. By looking at multiple smaller sections at multiple different lags, windowed cross-correlation is able to estimate synchronisation between systems which do not have a constant lag. Figure 3 is windowed cross-correlation output displayed as a heat map with warmer colours representing strong positive correlations between the two individuals’ behaviour (eg, positive non-verbal synchrony) and cooler colours representing strong negative correlations (eg, negative non-verbal synchrony). These synchrony scores are dyadic attributes that represent amounts and relationships of synchronous movement within dyads. Once we have obtained these scores, we will compare (1) effects of race concordance versus discordance on non-verbal synchrony and (2) effects of sex concordance versus discordance on non-verbal synchrony and (3) determine the relative impact of race concordance/discordance versus sex concordance/discordance on non-verbal synchrony.

Motion Energy Analysis software.

{kind=link}
{kind=link}
{kind=link}
Window cross-correlation output.
Hypothesis 1: Non-verbal synchrony will be greater in racially concordant than in racially discordant oncology interactions. To obtain time-varying synchrony scores, we will block each interaction into five equal segments and obtain synchrony scores for each segment using Motion Energy Analysis. This procedure also allows us to adjust for patients and physicians moving outside of the regions of interest set at the beginning of each segment and maximises the likelihood that we capture all patient and physician movement. For example, this strategy will help us capture continuous movement even if a patient or physician gets up from a seated position and walks outside of the predetermined region of interest. To model changes in dynamic and overall levels of synchrony, we will use structural equation modelling (SEM) methods, latent differential equations (LDE) and multilevel modelling (MLM) methods. LDE is a special case of SEM that allows for estimation of parameters of a proposed underlying dynamical system. LDE models contain parameters pertaining to the dynamics of a given system (eg, ‘eta’ and ‘zeta’ parameters of a latent harmonic oscillator model). We will use multigroup SEM modelling to test for differences in these parameters between racially concordant and racially discordant interactions. By using a likelihood ratio test comparing two models where (1) these dynamic parameters are free to vary and (2) where these parameters are constrained to be equal across models, we will be able to determine if the motion dynamics differ between racially concordant and racially discordant interactions. Using a three-level HLM model with time segments (level 1) nested within patient (level 2) and patient nested within physician (level 3), we will model changes in non-verbal synchrony based on a categorical variable modelling either racially concordant or racially discordant interactions. Assuming 168 dyads, an alpha of 0.05, a correlation coefficient of 0.1 and a linear time effect, we have a power of 0.8 to detect an effect size of 0.50.
Aim 2: determine the influence of non-verbal synchrony on physician communication and patient and physician affect in racially concordant and racially discordant oncology interactions
We will first collect the same observational measures for study 1 as in study 2, including physician patient-centred communication and patient and physician affect, and rapport. Trained research assistants will rate each of the racially concordant interactions on physicians’ patient-centred communication.48 Next, we will create thin slices of the interactions from study 1 and naïve observers will rate the slices using the same measures of physician–patient affect and rapport as in study 2. Then we will use the synchrony scores from aim 1 to compare the relationship between non-verbal synchrony and patient–physician affect and rapport in racially concordant and discordant interactions.
Hypothesis 2: Non-verbal synchrony will influence physician patient-centred communication, patient and physician affect, and relational rapport in racially concordant and racially discordant clinical interactions. We will use MLM and multigroup SEM to create a mediation model where non-verbal synchrony will predict level 2 (patient) and level 3 (physician) outcomes. Assuming 168 dyads, an alpha of 0.05 and a correlation coefficient of 0.1, we have power of 0.8 to detect an effect size of 0.48.
Aim 3: examine the antecedents and outcomes of non-verbal synchrony in racially discordant oncology interactions
We will achieve this aim using the synchrony scores from the racially discordant interactions in study 2. We will examine the relationships between non-verbal synchrony and (1) interaction outcomes collected in the parent study including: patient satisfaction, distress, perception of physicians’ patient-centred communication and treatment expectations, and physician perceptions of the patient (eg, willingness to follow treatment regimen) and (2) preinteraction physician and patient race-related attitudes and perceptions (eg, implicit bias; suspicion), also collected in the parent study.
Hypothesis 3: In the racially discordant oncology interactions, non-verbal synchrony will significantly negatively covary with patient postinteraction distress and positively covary with (1) patient postinteraction perceptions of physicians’ patient-centred communication and treatment expectations; (2) physicians’ postinteraction perceptions of patient personal characteristics (eg, understanding of treatment options) and their responses to treatment (eg, willingness to follow treatment regimen) and (3) observers’ ratings of physician patient-centred communication, patient and physician affect, and relational rapport. Using LDE, we will model dynamic parameter values of the fluctuations in non-verbal synchrony over the course of each interaction. These values will then be used as first-level predictors in an MLM model. The second-level predictors for this model will be values associated with physician and patient postinteraction perceptions of the interaction and of each other. Assuming 68 dyads, an alpha of 0.05 and a correlation coefficient of 0.1, we have a power of 0.9 to detect an effect size of 0.56.
Hypothesis 4: Non-verbal synchrony will significantly covary with preinteraction race-related attitudes and perceptions of the patient and physicians (eg, physician implicit bias, patient suspicion). We will create a three-level MLM. We will model synchrony assessed over five time segments nested within each patient and each patient nested within physician. Each patient–physician dyad will have its own average synchrony score.
Aim 4: Develop and test a mediational model that links physician and patient race-related attitudes and perceptions to non-verbal synchrony and, in turn, outcomes of race-related discordant oncology interactions.
Hypothesis 5: Non-verbal synchrony will mediate the relationship between preinteraction race-related attitudes and perceptions and postinteraction perceptions of the patients and physicians. To examine the proposed mediations in a multilevel context, we will use multilevel SEM, as described by Preacher et al.102 103 These models address potential conflated estimates of mediated effects that can arise when using multilevel data. Time segments will be nested within each patient and each patient will be nested within physician, with synchrony varying at each time point. We will use a single mediation model to assess how physician and patient race-related attitudes and perceptions influence interaction outcomes via their influence on non-verbal synchrony.
Patient and public involvement
Cancer survivors were heavily involved with both study 1 and study 2. Investigators had extensive conversations with survivors about their experiences as patients and survivors, which helped guide the research questions, measured outcomes and design of both studies.
Patients were not directly involved with developing the research questions and outcomes for this secondary analysis. However, this work extends naturally from the considerable previous work we have done focused on understanding and improving patient–oncologist communication for all patients, with special attention to patients more vulnerable to cancer treatment and mortality disparities. This secondary analysis will investigate another important aspect of patient–physician communication that our patient and physician partners have agreed needs research attention.
Recruitment to both study 1 and study 2 was done by the investigators and their research and clinic staff. As principal investigator, LMH, will disseminate results from this investigation through the Karmanos Cancer Institutes’ Department of Community Outreach and Education, which has regularly scheduled meetings with cancer survivors, caretakers and community stakeholders.
Ethics and dissemination
Only patients and physicians from the previous studies who provided their consent for secondary analyses of their data were included in the current study. The nature of the data makes it unlikely we will encounter ethical or safety issues.
We will submit our ongoing findings to relevant communication, social psychology and oncology conferences. Similarly, we plan to submit the final manuscripts to high-impact communication, social psychology and oncology peer-reviewed journals.
Strengths and limitations
This secondary analysis is innovative in its focus and method. This study explores non-verbal synchrony, a channel of communication that has not been previously examined in medical interactions. It takes advantage of existing datasets, which include video-recorded cancer treatment discussions of black and white patients with cancer, recorded with state-of-art recording equipment. It also applies automated behavioural coding software, thus introducing less error than traditional methods using human coders.
However, this study is not without limitations. First, this study takes advantage of existing datasets, but the video-recorded and self-report data were not collected with the current hypotheses in mind. Second, the data are not evenly distributed by sex and race. As is often the case with medical research involving actual patients, the distributions of study patient characteristics are constrained by the distributions of patient demographic and medical characteristics of the patients who are treated at the participating hospitals. This reality precludes us from fully examining all combinations of race and sex. However, there are advantages to the fact that this research is conducted in a real-world, rather than a laboratory setting; also, we are able to account for some variability in our models by treating certain factors (eg, cancer type) as random effects. Last, although given a design that is adequately powered to make both between-subject and within-subject comparisons, it is still possible we may find no significant findings regarding non-verbal synchrony. Of course, this finding would be interesting in and of itself and would direct research attention to other avenues of investigation.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
Footnotes
Contributors All authors meet criteria for authorship. LMH: principal investigator, involved in all aspects of conceptualisation and study design. RM: research assistant, involved in the study design and responsible for design and implementation of statistical anlayses. TLA: coinvestigator, involved in all aspects of conceptualisation and study design. SB: coinvestigator, involved in all aspects of conceptualisation and study design and responsible for design and implementation of statistical analyses. SE: coinvestigator, involved in all aspects of conceptualisation and study design. LAP: coinvestigator, involved in all aspects of conceptualisation and study design.
Funding This work was supported by the National Institutes of Health/National Institute on Minority Health and Health Disparities 1R21MD011766-01A1 (LMH, PI).
Competing interests None declared.
Patient consent Not required.
Ethics approval Studies 1 (069003B3D), 2 (125211B3E) and the current study (044716B3E) are all approved by the Wayne State University Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.