Article Text

Abstract
Background The number of EDs visit is on the increase, and the pressure on EDs is of significant concern worldwide. The usage of EDs by parents of children with minor illness is an important and still unresolved problem causing a burden to healthcare services. The aim of this study was to review the literature to summarise parental reasons for visiting ED for children with minor illness.
Method Seven electronic databases (Medline, Embase, PsycINFO, CINAHL, PubMed, Web of Science and Scopus) were comprehensively searched during a 2-week period in August 2016 and updated between 11 and 20 June 2018. The study selection process was undertaken independently by two authors. Qualitative and quantitative studies that focused on the reasons for parents of children with minor illness to attend an ED were included. Studies were assessed for quality and data were analysed by means of narrative synthesis.
Results Twenty-four studies were included. Eleven studies employed quantitative methods, eleven studies used qualitative methods and two studies used mixed methods. Parental reasons for using ED included perceived urgency, ED advantages (eg, faster service, superior ED resources and efficiency), difficulties with getting a general practitioner appointment, lack of facilities in primary healthcare services, lack of health insurance, reassurance, convenience and access.
Conclusion This review identified some of the reasons why parents bring their children to the ED for minor illnesses highlighting the multifaceted nature of this problem. Understanding parental reasons behind their choice to use the ED may help us better design targeted interventions to reduce unnecessary ED visits and alleviate the burden on overstretched healthcare services. This review may help inform emergency care policy makers, researchers and healthcare staff to understand parents’ reasons for visiting the ED, to better meet their healthcare needs.
- emergency care systems, admission avoidance
- emergency department utilisation
- paediatrics, paediatric emergency medicine
- paediatrics, paediatric injury
- emergency departments
Statistics from Altmetric.com
- emergency care systems, admission avoidance
- emergency department utilisation
- paediatrics, paediatric emergency medicine
- paediatrics, paediatric injury
- emergency departments
Background
The number of EDs visit is on the increase, and the pressure on EDs is of significant concern worldwide.1 The usage of EDs by patients with minor illness is an important and still unresolved problem, which places significant burden on healthcare services,2 increases waiting times in the ED3 and is of significant concern to ED staff, ED directors and policy makers.4
Prior studies suggest that many parents bring children with minor illnesses to the ED when they could be managed in primary care through their own General Practitioner (GP) other primary care provider.5–7 The term ‘minor illness’ was operationally used by Butun and Hemingway8 as non-urgent cases that could be treated by simple medication, self-care or need no treatment. Recent figures on paediatric ED visits suggest around 40% (n=1244) were non-urgent in a study conducted across 12 hospitals in Belgium.9 Just over half (53%) of ED visits were categorised as least urgent in Australia,10 while in the USA between 37% and 60% of 25 million paediatric attendances were considered as non-urgent visits per annum.11 12 Data for England show an increase of 32% in all ED attendance in the past 10 years,13 with visits for non-urgent conditions estimated at 40%.14
Given the demands placed on overstretched ED resources, it is important to understand why parents bring their children with minor illness to the ED instead of primary healthcare. To date, there are no mixed methods systematic reviews that bring together all the available data in this important field. A limited number of systematic reviews (n=3) were identified, which focused on adult patients,15 ED visits solely in the USA16 or reviewed only qualitative evidence.8 Our review specifically focuses on parental reasons for using the ED for their children presenting with minor illness and brings together both quantitative and qualitative data without limitations of date and origin. This review sought to address the question as to why parents bring children with minor illnesses to the ED.
Method
A mixed methods systematic review was undertaken, which applied specific inclusion/exclusion criteria to the identified papers. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines on the reporting of systematic reviews were adhered to throughout.17 We sought to include evidence from any type of empirical research design in order to cover sufficient breadth of the available literature, to increase the validity of our findings and increase their applicability to policy and practice.18
Inclusion and exclusion criteria
Studies that focused on the reasons for parents of children with minor illness to attend an ED were included. ‘Parents’ for this review refer to any parental guardian of a child aged under 18 years, with no consideration of the individual’s gender or age. No restrictions were placed on study design or publication date. Studies published in the English or Turkish languages were considered due to existing familiarity within the research team.
Search strategy
The search strategy included a list of relevant keywords and terms, including common abbreviations and alternative spellings (eg, British and American). Seven electronic databases (Medline, Embase, PsycINFO, CINAHL, PubMed, Web of Science and Scopus) were comprehensively searched in August 2016 and further updated between the 11 and 20 June 2018. The keywords included (parent* OR carer* OR caregiv* OR family*) AND (child OR children OR baby OR babies OR infant* OR adoles* OR teen* OR p?ediatric*) AND (minor illness OR non-urgent OR non-emergency OR non-critical OR non-essential OR non-serious) AND ((emergency ADJ (department OR service OR hospital OR centre OR center OR accident OR ward OR unit) OR (accident and emergency)).
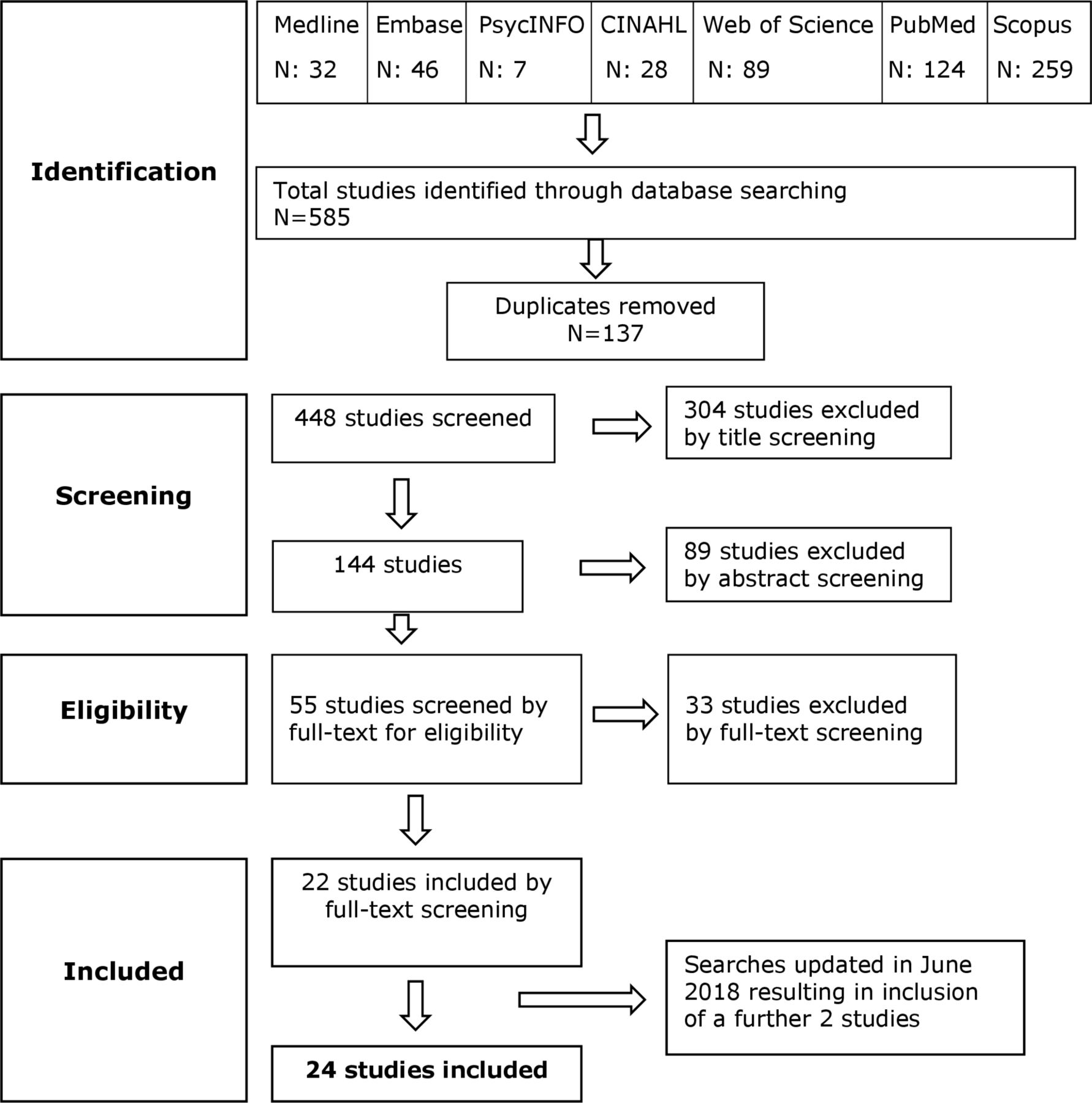
Two authors (AB and ML) independently performed and agreed on the study selection. The searches yielded a total of 585 studies which included 137 duplicates. Following duplicate removal and title review, 304 studies were excluded. Abstract review of the remaining 144 studies excluded a further 89 manuscripts. Full-text screening, employing the prespecified inclusion/exclusion criteria, was applied to 55 studies which resulted in 33 further exclusions, leaving a final total of 22 included studies. Updating the search strategy in June 2018 resulted in the inclusion of two additional studies. Therefore, a total of 24 studies were included in this review. A PRISMA flow diagram of the study selection process is presented in figure 1.
{kind=link}
Flow diagram of search strategy.
Quality assessment and data extraction
Quality assessment and data extraction of the included studies was conducted by AB with ML checking for accuracy; consensus was reached via discussion. The quality of all qualitative studies was assessed using an appraisal checklist developed by the National Institute for Health and Care Excellence.19 The quality of quantitative studies was assessed using the National Institute of Health quality assessment tool.20 Each tool contains 14 criteria that focus on the research question, objectives, method, population, data, discussion and limitations. All included studies were classified as having good, fair or poor methodological quality based on quality assessment tools. A data extraction tool was employed to consistently extract data from 24 included studies. This tool aided in summarising key features of the studies including setting, design, participants, method of data collection and findings.
Data analysis
Due to the heterogeneity of included studies, a narrative synthesis was deemed as the most appropriate way to analyse the data. Narrative synthesis is an approach which focuses on textual data to summarise and explain findings from a systematic review which has included studies employing diverse methods, populations and measurements.21 Heterogeneity in narrative synthesis is explored through comparison of study characteristics21 and is described in table 1 and below.
The characteristics of the included studies
Results
Overview of included studies
Twenty-four studies published between 1988 and 2017 were included in the review. All included studies were reported in English; no Turkish research was located. Eleven studies employed quantitative methods of cross-sectional designs,5 6 9 12 22–28 eleven studies used qualitative methods which included observational, ethnography and grounded theory designs4 29–38 and two studies used mixed methods using cross-sectional designs.39 40 Data collection instruments across all studies were either interviews or questionnaires. Each included study had a different data collection instrument. Fourteen studies were conducted in the USA, three in Canada, two in the United Kingdom (UK), two in Australia, one in Belgium, one in Singapore and one in Lithuania. Sample sizes ranged from 1231 to 31179 participants with an overall total of 7561. Eight included studies collected data following triage while participants were waiting to be seen by a doctor.5 24 25 27 29 30 38 39 Eight studies collected data from participants who triaged as non-urgent, but there was no further information regarding whether this occurred before or after ED visits.12 22 23 28 31 33 34 37 The data of three studies were collected after participants visited the ED.26 32 35 Five included studies did not provide any information about when the data were collected.4 6 9 36 40 Further characteristics of the included studies are presented in table 1.
Quality assessment
The quality of included studies were judged as good, fair or poor based on two quality appraisal tools. Seven studies were assessed as having good quality,4 29 30 32 34–36 fourteen studies were considered as having fair quality5 6 9 22–24 26 28 31 33 37–40 and three studies were assessed as having poor quality.12 25 27 The results of the quality assessment are presented in table 1. Studies which received a high-quality appraisal score provided information about the research question, aim and objectives, design, participants, settings, time-frame and ethical issues. Studies that were assessed as possessing lower quality failed to explain how data collection carried out, the role of the researcher, sample size calculation and the potential role of confounding variables. No studies were excluded based on quality assessment in an attempt to provide sufficient breadth of data from diverse sources.
Strengths and weaknesses of the included studies
The majority of studies used a single setting for data collection,4 5 12 22–29 31–33 35–37 39 40 which may limit the generalisability of their findings. In contrast, some studies used multiple settings which increased robustness of study design.6 9 30 34 38 Four qualitative studies stated that data saturation was reached,29 32 33 35 while some used triangulation to further substantiate findings.30 33 Such approaches are commonly employed to increase the robustness of qualitative data. Using convenience sampling4 9 12 22 23 25 30 34 35 39 limited the representativeness of study findings. Without fail, data were obtained from populations in high-income countries, suggesting that the needs and preferences of parents from low-income and middle-income countries are unknown.
Perceived urgency
Perceived urgency was the most frequently cited reason for visiting the ED by parents of children presenting with minor illnesses. This issue was identified in 17 of the included studies.4–6 9 23–25 27 28 30 33–35 37–40 Some parents felt that their child’s condition constituted a genuine emergency before their ED attendance.34 According to a study by Phelps et al,6 conducted in the USA, 35% (n=70) of caregivers in their sample of 200 felt that their child was very sick and needed to receive immediate care. Parents considered that it was more appropriate to immediately attend the ED5 24 40 for fear that their child’s symptoms might become more serious with delay.4 25 27 39 Parents were most concerned by fever and felt anxious if they perceived the fever to be high.33 35 In addition, some parents did not feel confident about managing the illness at home or going to primary healthcare providers, if they perceived the child’s condition as urgent.9 35 37 Additionally, some parents felt that there was nothing further they could do at home and, therefore, preferred to visit an ED.
ED advantages
The perceived advantages of ED use were reported in 17 studies.4–6 12 22 25–30 33 35 36 38–40 These included ED staff expertise with children, faster service, quality of care, opening hours, previously positive experiences in the ED, better ED resources and efficiency. Parents believed that ED staff were more skilled in caring for children than their GP or primary care provider.12 29 30 33 35 36 In some cases, parents preferred to entirely bypass their GP in favour of the perceived expertise of the ED staff.33 Also, many parents reported choosing the ED due to shorter waiting times.4–6 22 26 27 30 33 The availability of superior resources in ED were cited by a number of studies as influencing parents’ reasons for attending.4 5 22 29 30 32 36 39 Truman and Reutter39 found that parents felt ED staff possessed both the knowledge and equipment to treat their child. Salami et al22 also found that the ED was chosen because of the perceived availability of diagnostic tests. The quality of care delivered in the ED also impacted on parents’ decision regarding their usage.4 6 12 22 29 36 38–40
Problems with primary healthcare services
Fourteen studies reported perceived deficiencies with primary healthcare services, which affected parents’ decision to attend the ED.4 5 9 22 23 26 27 29–31 34 35 37 40 These included difficulties with obtaining an appointment, dissatisfaction with their GP, lack of confidence in their GP, mistrust of primary healthcare services and non-registration with a GP practice. Problems in relation to the nature of primary healthcare services included specific working hours and lack of facilities. A large number of participants (n=104, 43%) in the study by Hendry et al,5 conducted in the USA, visited the ED based on parents’ previous experiences of being referred by their GP. These problems with primary healthcare services affected parents’ use of ED for minor illnesses.
Convenience and access
In 15 included studies convenience and access were frequently reported reasons in parents’ decisions to attend the ED.4–6 9 22 25–27 29 31 33 37 39 40 Some parents found ED services more convenient due to childcare arrangements5 and preferred the immediacy of not needing an appointment.29 Parents also tended to use the ED due to its accessibility and its proximity to their home.4 6 9 26 27 33 37 39 40
Out of hours
Parents reported using the ED for minor illnesses due to a lack of out-of-hours service provision by primary healthcare providers.5 6 9 12 22 25 26 30 35 37 39 40 One study found that 21 participants (28%) chose to attend an ED as the paediatrician’s office was closed during the day39 and 40 participants (28.4%) in a second study reported using the ED following work, when their primary healthcare provider was closed.40 Some parents stated that their doctor’s office was closed and the ED was the only available service for care.6 The demands of work mean that parents cannot always alter their work schedule, and therefore a visit to the ED after working hours is the only available option.30 35
GP referral
Several studies found that parents were referred to the ED for minor illness by their GP.6 23 24 26 27 29 30 34 37 40 Twenty-one per cent (n=41) of participants in the study by Phelps et al,6 and around 59% (n=177) of those in the study by Smith et al27 visited the ED because they were referred. Whether this is a precautionary action, or the GP lacks capacity, such referrals place unnecessary demands on already stretched ED resources.
Lack of health insurance
Lack of health insurance, inadequate insurance coverage or financial issues were cited as reasons for attending the ED in seven included studies, five of which were conducted in the USA, one in Australia and one in Singapore.12 22 23 26 30 35 40 Lack of health insurance meant that many parents had little choice in visiting the ED to seek help for their child.22 30 The nature of cover provided by the health insurance policy was cited as a reason for some participants attending the ED. For example, 12 participants (17.4%) in the study by Smith and McNamara26 reported that their insurance provided cover for ED but not for visits to their GP.
The need for reassurance
The need for parents to be reassured over their child’s illness was another reason for visiting the ED.4 22 24 28 30 32 34 38 Parents preferred not to take sole responsibility for their children’s illnesses; they preferred to visit the ED to ensure the illness was nothing to worry about. Parents expressed their need for reassurance because of their children’s inability to explain the effects of their conditions.30 The need for reassurance that their children were safe from harm was a primary determinant in parents’ decision making.32 This need appeared to be increased among parents of newborns and first-time parents.4
Gaining a second opinion
Some parents had availed of a prior medical opinion before attending the ED but desired a second opinion on their child’s condition.5 A parent in the study by Guttman et al30 reported feeling afraid that she was not giving her child the right medication. Therefore, this participant came to the ED to gain a second opinion and a better explanation of the medication. Soliday and Hoeksel40 reported that some parents were not satisfied with their primary care physician’s recommendation and so preferred to visit the ED for their child’s care. In addition, some parents visited the ED following advice from trusted individuals in their social network.28 Table 2 shows parents’ reasons for visiting the ED and the number of included studies which reported these.
Frequency count of parents’ reasons for attending the ED
Discussion
This review sought to identify why parents bring their children with minor illness to the ED. Our findings highlighted that parents’ reasons for using the ED included the perceived urgency of their child’s condition, advantages of the ED (eg, better resources, faster service and ED staff expertise with children), problems with primary healthcare services (eg, the inability to receive a timely GP appointment and mistrust), convenience and access issues, out of hours, referrals by GP, financial issues, reassurance and desire for a second opinion. The majority of included studies were assessed as having high methodological quality.
Parents’ perception of the urgency of their child’s condition was one of the most cited reasons for using the ED. Clearly, parents worry about their child’s health and seek care as soon as possible, rather than waiting at home or for the next available appointment with their primary care physician. Parents appear to see the ED as the most appropriate place to seek care during this worrying time. It is difficult to change the behaviour of parents who perceive their child’s condition as urgent due to the emotionally charged nature of such situations and a possible lack of experience or knowledge of the child’s condition. The importance of perceived urgency has been highlighted as an issue in another study, particularly with first-time parents, who may lack experience in dealing with a sick child.10 Providing parents with knowledge about what constitutes urgent and non-urgent care for common childhood diseases would aid parents’ decision making in attending the ED.29 37 It has been recommended that increasing the insight and knowledge of parents in the appropriate use of healthcare services could improve the quality of care in ED, decrease inappropriate usage and reduce costs.9 Additionally, greater health literacy, or the provision of feedback on usage, could dissuade attendance. May et al38 claim that parents’ low health literacy is associated with worry and lack of knowledge about their child’s health, which results in an inability to provide self-care and a tendency to use the ED as a readily available source of care. Therefore, increasing parental health literacy may help parents to better assess their child’s condition and subsequently provide opportunities for self-care or the use of alternative healthcare providers.
Several studies highlighted that parents used ED due to its perceived advantages. Some parents perceived ED doctors as more skilled than GPs or they believed their child would receive better care at the ED.29 The provision of better care was highlighted in another study as a reason for attending ED by 47% of their sample.41 In addition, some parents argued that ED staff possessed greater expertise in working with children.29 30 Visiting the ED may be considered as a rational choice for parents who perceive ED staff to be more skilled than their primary care physicians, seek reassurance concerning their child’s condition and perceive their child’s condition as urgent. Findings also showed that parents used the ED due to its resources and availability of diagnostic tests. This may be based on the perception that the ED possesses greater resources and access to a wider variety of specialisms and equipment. A study by Keizer Beache and Guell42 reported that past positive experiences and quality of care in the ED affect people’s decision to use the ED.
Restricted opening hours, lack of appointments and availability of GP services, dissatisfaction with their GP or mistrust of primary care provider were shown to affect parents’ decision to use the ED. These reasons were cited in the majority of included studies and show that some parents are not satisfied with the services provided by their GPs and therefore visit the ED for care. A recent review by Butun and Hemingway8 suggested that if parents are dissatisfied with their primary care provider or with received treatment, it is more likely that they will not revisit these services. These findings are further supported by previous researchers who cite frustration from patients who must contend with long waiting lists, poor communication and restricted opening hours when attempting to gain an appointment with their primary healthcare provider.41 As a result, Weber et al3 argued that using the ED may be a rational decision for those who have unmet healthcare needs. Therefore, it would be beneficial that primary healthcare services might want to focus on how to meet with patient’s need and ultimately increase the level of patient’s satisfaction. The provision of greater access to primary healthcare services, greater efficiency, better communication skills and improved appointment scheduling may help decrease non-urgent ED visits. There is also need for greater provision of resources and triage of patients within primary care to divert parents from attending the ED. Where available, out-of-hours services could be better used to reduce non-urgent cases.
The findings of this review note the importance of access issues and convenience in ED usage. Access issues, such as transportation and distance of healthcare services to home, led parents to use the ED. The findings of convenience and access issues are supported by previous researchers who valued the access and convenience of attending the ED.41 As a result, the close geographical distance of the ED may have an impact on parental decision to use the ED.43 Some parents found the ED more convenient because of working hours4 5 37 and because they did not require an appointment.29 The demands of work mean that many parents are unable to change their working schedules or take time off work, and therefore the after-hours service of the ED is a more convenient way to meet their healthcare needs. The problem of parents not wanting to take time off work to seek care and accessing alternative after-hours services is evident in the literature.44 Patients have expressed a desire to be seen by their primary healthcare provider suggesting that if such services were made more accessible there would be a corresponding decrease in ED attendance.10 45 Some parents thought that their ED visit could have been avoided if their GP practice held more flexible opening hours when they initially sought care.45 It would appear that if alternative services were available to parents, non-urgent visits to ED could be prevented.46 Such a reduction could conceivably be accomplished by extending the opening hours of primary healthcare providers and improvement in after-hours services.
Strengths and limitations
One of the strengths of this review is the comprehensive search strategy employed, which used seven electronic databases and the independent application of inclusion/exclusion criteria, standardised data extraction and quality appraisal by two authors. However, we did not undertake an exploration of the grey literature and it is possible that we have omitted some relevant papers.
All included studies in this review were carried out in wealthy, well-resourced countries (the USA, the UK, Canada, Australia, Belgium, Singapore and Lithuania). It is likely that, while many of the issues will remain the same for low-income and middle-income countries, some will be unique given the variability in cultural, economic and political contexts. The categories created through our narrative analysis are therefore limited by the available literature derived from high-income countries. By limiting our searches to the English and Turkish languages, we may have inadvertently excluded important sources of additional information. In addition, many of the included studies failed to define the term non-urgent.4–6 12 22 25 27 31 33 36–38 40 The lack of clear definition raises doubts as to whether these studies were measuring the same concept and creates difficulties when making comparisons between studies.
Future research
The characteristics of different healthcare systems might affect decisions to attend ED for minor illnesses. Therefore, it is advisable to compare and contrast a range of different systems to capture such inherent variability. As all included studies were conducted in high-income countries, it is suggested that there is a need for further investigation among low-income and middle-income countries, which may provide important and unique insights. In addition, Stockwell et al47 argued that parents’ reasons for using the ED with their children, rather than the GP, have changed significantly between 1997 and 2006. According to Stockwell et al,47 families living in the USA were less likely to visit ED for reasons of perceived urgency (21.7% vs 62.5%) in 2006 compared with 1997; however, they were more likely to visit ED due to limited access to their primary healthcare services (43.5% vs 20.3%). In the current climate of continuing change within the healthcare systems, it is important to conduct research about parental reasons for using the ED on an ongoing basis to meet with parents’ needs.
Conclusion
The reasons for parents visiting ED with their children for non-urgent conditions are complex and multifaceted. This review identified some of the difficulties within healthcare systems, which resulted in parents using the ED to access care for their children. Therefore, addressing problems of parental mistrust of primary healthcare services, poor communication skills, restricted opening times and difficulties with GP appointments is important to change patterns of behaviour. By understanding parental reasons for using the ED, primary healthcare providers could better design and target interventions to increase levels of satisfaction and therefore divert parents from the ED. Greater health literacy and support for parents are needed if we are to reduce the increasing burden placed on global healthcare services. This review may inform policy makers who seek to reduce ED visits by understanding parental reasons for using the ED and their health needs to design interventions for this multifaceted issue. Future interventions could be designed to impact parents’ decision making prior to ED attendance.
Acknowledgments
This piece of research has been presented at the 28th International Conference on Pediatric Nursing and Healthcare in 2017 in Edinburgh, UK.
References
Footnotes
Contributors All authors were involved the conception, design, analysis and interpretation of data of this review. AB created the search strategy and carried out the search. AB wrote the manuscript and received regular feedback from ML, FL and JMG.
Funding PhD funding was provided by the Ministry of National Education, Republic of Turkey.
Competing interests The reviewers declare that there are no conflicts of interest. This review has been completed as part of Butun’s PhD studies at Queen’s University Belfast.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.