Article Text

Abstract
Objectives To describe attendance at emergency departments (EDs) in the year prior to suicide for a sample of mental health patients. To examine the characteristics of those who attended (particularly those who attended frequently) prior to suicide.
Design Case review of ED records for 286 individuals who died within 12 months of mental health contact in North West England (2003–2005).
Method Cases identified through the National Confidential Inquiry into Suicide were checked against regional EDs to establish attendance in the year prior to death. Records were examined to establish the number of attendances, reason for the final, non-fatal attendance, treatment offered and outcome.
Results One hundred and twenty-four (43%) individuals had attended the ED at least once in the year prior to their death, and of these, 35 (28%) had attended the ED on more than three occasions. These frequent attenders died by suicide significantly sooner after their final, non-fatal attendance than other attenders. A clinical history of alcohol misuse was also associated with early death following ED attendance.
Conclusions Over 40% of our clinical sample attended an ED in the year prior to death, and some individuals attended particularly frequently. EDs may therefore represent an important additional setting for suicide prevention in mental health patients. The majority of attendances prior to suicide were for self-harm or to request psychiatric help. Clinicians should be alert to the risk associated with such presentations and to the possible association between frequent attendance and suicide.
- Emergency medicine
- suicide
- mentally ill persons
- emergency care systems
- emergency departments
- mental health
- self harm
Statistics from Altmetric.com
- Emergency medicine
- suicide
- mentally ill persons
- emergency care systems
- emergency departments
- mental health
- self harm
In England and Wales, suicide accounts for approximately 5000 deaths annually.1 The National Confidential Inquiry (Inquiry) collects detailed clinical data on suicides in recent contact with mental health services in the year prior to death.
Previous research has suggested that the Emergency Department (ED) may be a setting for effective suicide prevention.2 Gairin et al3 found that, in the year prior to death, 39% of those who died by suicide visited the ED. Of these, 39% (15% of all suicide deaths) attended the ED as a result of self-harm (most commonly self poisoning). The interval between the final attendance and death was shorter for self-harm attendances than attendances for other reasons.
Other research has focused on frequent or “regular” ED attenders who are often defined as individuals who attend more than three times in 1 year.4 5 Such individuals have been identified as a highly vulnerable group.5 The burden of frequent attenders, both in terms of economic cost and the increased workload to ED staff, has been highlighted,6 as has the increased mortality risk for frequent attenders.5
Mental illness is one of the strongest risk factors for suicide,7 8 but few studies have examined ED contacts before suicide in clinical samples of mental health patients. The current study examined ED attendances in the 12 months prior to suicide among a regional sample of those in mental health service contact in North West England. We were keen to explore the potential for suicide prevention in the ED setting. We had three specific objectives:
Describe the patterns of attendance at the ED in the year prior to suicide.
Investigate the characteristics of those who attended the ED prior to suicide, particularly frequent attenders.
Examine in detail the final attendance prior to suicide, focussing on reason for attendance, treatment offered and how near to death contact occurred.
Method
The methods used in the National Confidential Inquiry into Suicide and Homicide by People with Mental Illness have been described in detail elsewhere9 10 Data collection on suicides involved three stages: (1) collection of a comprehensive national sample, irrespective of mental health history; (2) identification of people within the sample in contact with mental health services in the 12 months before death; and (3) collection of their clinical data. National data on all deaths in England and Wales receiving a verdict of suicide or an open verdict at coroner's inquest were obtained from the office for National Statistics. Both verdicts were used because official UK suicide statistics are based on this definition, and previous research indicates that using only “suicide” verdicts would result in an underestimation of the number of suicide deaths.11 Clinical data were collected via questionnaire using the robust ascertainment procedures employed by the Inquiry.1
Details of the study were sent to all general hospitals in the North West of England (n=38). One hospital was unable to access records prior to January 2004 but still provided details on later attendances. Based on annual attendance figures for 2005–2006 and assuming these remained consistent during the study period, we estimate that our methodology captured over 90% of attendances for the North West population.
Emergency Department records for a consecutive sample of 286 North West Inquiry cases occurring between 1 January 2003 and 7 May 2005 were reviewed in order to establish patterns of ED attendance throughout the North West in the year prior to death. Patient details (name, dates of birth and death, and address) were sent to EDs in close geographical proximity to the deceased's home address to identify whether the patient had attended the department in the 12 months before death. Individual patient details were sent to between one (for rural locations) and six (for urban areas such as Greater Manchester) EDs in order to capture as many attendances as possible. For any attendances identified, researchers visited the department and reviewed ED records. Information was collected on the number of attendances at the ED and detailed information gathered on the final, non-fatal attendance at the department (including reason for attendance, time and date of attendance, details of any treatment or assessment offered, any referrals made and outcome of the attendance).
Analysis
Data were entered into SPSS and analysed using SPSS V.11.5. Initial descriptive analysis was conducted to establish patterns of attendance to the ED and to identify those patients who were regular or frequent attenders. “Frequent attenders” were defined as those patients who had attended the ED more than three times in the year prior to death.5
Further descriptive analysis was carried out to identify socio-demographic and clinical characteristics of attenders, non-attenders and frequent attenders. χ2 tests of association were conducted on categorical data to establish differences between groups of attenders at final attendance prior to suicide. For continuous data, Mann–Whitney and t tests were used to establish differences between groups. We also examined predictors of death within 1 month of final attendance at the ED using a logistic regression analysis. Initially unadjusted odds ratios (ORs) were calculated. The ORs were then adjusted in a multi-variate model for age quartile, sex, serious mental illness and a history of self-harm. We also explored time to death using formal survival methods (Cox's regression analysis and Kaplan–Meier plots).
When percentages are quoted, these refer to valid cases, that is if an item of information was not known about a person, he/she was excluded from analysis of that item. As a result, denominators may vary slightly between analyses.
Results
Characteristics of the sample
The sample was predominantly white (n=267, 93%), and over half were unemployed or on long-term sick leave at the time of death (n=157, 55%). The age of the sample ranged from 19 to 95, with a mean age of 47 years. The male-to-female ratio was 2:1. The most common method of suicide was hanging/strangulation followed by self-poisoning.1 Fifty-five cases (20%) had a primary diagnosis of schizophrenia and other delusional disorders, 134 (48%) affective disorders, 26 (9%) alcohol dependence and 8 (3%) drug dependence.
Attendance patterns at emergency departments
Of the 286 cases, 124 (43%) attended at least one local ED in the 12 months prior to their death. Of these, 23 attended two different EDs, and three attended three. Those who attended multiple EDs were from urban areas with several local hospitals. The number of attendances in the year prior to death ranged from 1 to 30 (mean=3.26, median=2 SD=3.68, IQR=1, 4) as shown in figure 1.

Total number of ED contacts in the 12 months preceding suicide.
Characteristics of non-attenders, attenders and frequent attenders
Those who attended EDs in the year prior to death and those who did not were similar in terms of their main characteristics.
Of the 124 who attended an ED in the year prior to death, 35 (28%) had attended on more than three occasions and were considered “frequent attenders”. Table 1 shows the characteristics of frequent attenders and all other attenders.
Descriptive features and primary diagnosis for frequent and other attenders to the ED in the North West in the year prior to death
Frequent attenders were significantly more likely to have a history of self-harm and alcohol abuse than other attenders and significantly less likely to have a primary diagnosis of affective disorders (bi-polar disorder or depression) than other attenders. Frequent attenders were also more likely to be unemployed and had significantly more attendances for psychological reasons (including self-harm) in the year prior to death than other attenders.
Final attendance prior to death
The most common reasons for the final, non-fatal attendance to the ED were self-harm (n=48, 39%), requests for psychiatric help (n=35, 28%), physical injury/illness (n=30, 24%) and alcohol intoxication (n=8, 7%). Patients whose final attendance was a result of self-harm had significantly more attendances for psychological reasons (including self-harm) in the year prior to death than those whose final attendance was for alcohol or physical injury (median=2, IQR=1–4 vs median=0, IQR=0–1; Mann–Whitney U=411 p<0.001). Eleven of the 31 cases (36%) who went on to die by self-poisoning had a final attendance at the ED as a result of an overdose.
We found no significant differences in time between final attendance and death between those who had attended following self-harm and those who had attended for other reasons. However, time between final attendance and death for frequent attenders was significantly shorter than it was for other attenders (median 24 days vs 93 days; Mann–Whitney U=1087, p=0.009).
Figure 2 shows the assessment and outcome of patients who attended following self-harm or to request psychiatric help. Patients attending following self-harm had little evidence of psychosocial assessment (n=11, 24%), but most were admitted following attendance (n=35, 73%). Conversely, most patients requesting psychiatric help had evidence of assessment (n=22, 65%), but less than half were admitted (n=15, 43%).
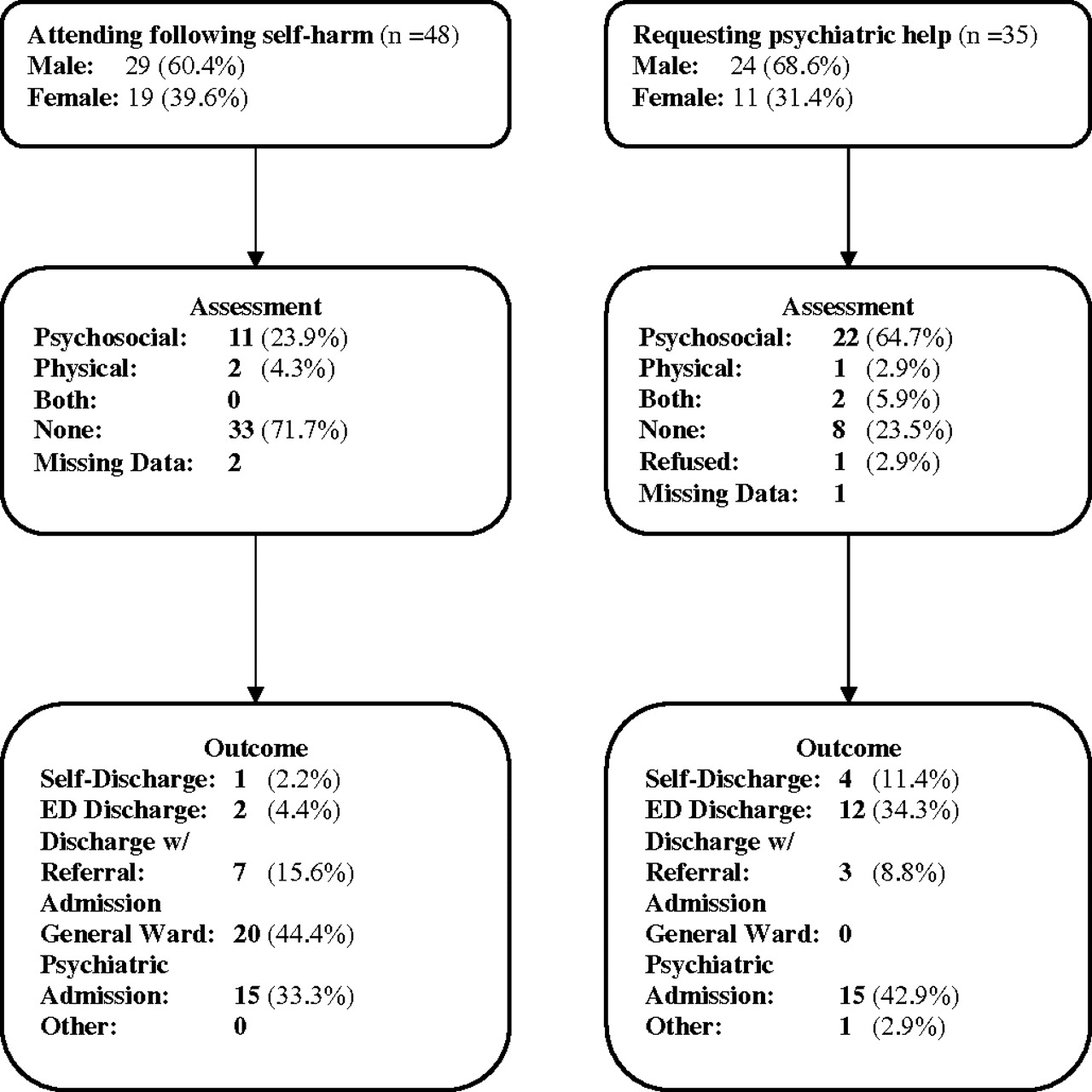
Assessment and management of patients in this study who had attended the ED as a result of self-harm or to request psychiatric help prior to death.
Timing of death following final attendance at ED
We explored the timing of death in relation to final attendance in two ways. Initially, we examined the predictors of death within 1 month of final attendance at the ED using a logistic regression analysis. Table 2 shows the variables that had an OR of 1.5 or greater. Frequent attendance and a history of alcohol misuse were significantly associated with death within 1 month of attendance. A history of drug misuse and a final attendance for psychological reasons or self-harm were of borderline significance. Adjusting these results for age quartile, sex, serious mental illness and a history of self-harm attenuated the ORs slightly. We also explored time to death using a survival analysis. Cox's regression analysis showed that two variables were significantly associated with early death following final attendance. (ie, a shorter interval between last ED contact and death) These were frequent prior attendance (HR=1.69 (1.13–2.53) p=0.015) and unemployment (HR=1.54 (1.07–2.21) p=0.022). Figure 3 shows the Kaplan–Meier plots for these variables.
Predictors of death within 1 month of ED attendance

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier plots for unemployment and frequent attendance at the ED.
Discussion
Main findings
A significant proportion of mental health patients who went on to die by suicide attended the ED in the year prior to death. Forty-three per cent of the sample attended the ED on at least one occasion, and 12% of the total sample (n=35) attended an ED on more than three occasions and could be considered “frequent attenders”.
These frequent attenders went on to die by suicide significantly sooner after their final, non-fatal ED attendance than less frequent attenders. Most frequent attenders had a history of self-harm (94%), two thirds a history of alcohol abuse (68%), 63% were unemployed at the time of death, and almost half (49%) had a history of drug abuse. Frequent attenders also had significantly more attendances for psychological reasons or self-harm in the year prior to death than all other attenders.
In general, early death following final attendance was associated with frequent prior attendance at the ED and a history of alcohol misuse. The survival analysis suggested that social factors such as unemployment may have been associated with a shorter time to death.
Two thirds of the final, non-fatal attendances to the ED in this study were as a result of self-harm or to seek psychiatric help. The most common form of self-harm was overdose. Over one third of those who went on to die by self-poisoning had a final attendance at the ED as a result of an overdose. The majority of those who had presented with self-harm prior to death were admitted to general medical or psychiatric care.
Key findings in relation to previous research
This is one of the few studies to our knowledge to explore the issue of ED attendances prior to suicide in a clinical sample of mental health patients. Consistent with Gairin's general population study,3 a similar proportion of our sample attended the ED prior to death (43% vs 39% in the Gairin study). The same proportion of attenders had presented with self-harm (39%) in both studies.
Best practice guidelines recommend that all self-harm patients attending the ED receive a psychosocial assessment,12–14 but like previous studies,15 16 we found a low documented level of psychosocial assessment. However, this does not appear to reflect a lack of care, as the majority of patients attending following self-harm were admitted to hospital for further treatment or discharged with follow-up from other services. Only 4% were discharged without further treatment or follow-up.
Strengths and limitations
The primary strength of the current study is that it covered almost all ED attendances for people in recent contact with mental health services in the North West between January 2003 and May 2005. Based on annual attendance figures from 2005–2006 for EDs in the North West, we estimate that our methodology captured the majority of local ED attendances for the North West Inquiry population. Data collected from ED records was linked with information on the Inquiry database enabling examination of the clinical and demographic characteristics of ED attenders.
However, our findings need to be interpreted in the context of a number of methodological shortcomings. We only looked at ED attendances by a group with high morbidity and mortality and significant care needs. It would have been informative to have examined attendance patterns in a general population control group, but this was beyond the scope of the current study. However, many of our findings are similar to Gairin's3 general population study, and it is possible that our findings will be applicable to the general population, particularly as a majority of people who go on to die by suicide have been found to have evidence of mental disorder.8 In addition, our study only examined attendances at EDs local to the patient's home address. We therefore would miss any ED attendances occurring in other locations, but previous research on self-harm episodes in Manchester suggests that such “cross flows” of attendance are comparatively rare.17
While the current study accurately illustrates patterns of ED attendance, detailed information was only collected on the final non-fatal attendance prior to death. Therefore, we are unable to comment on treatments received on previous attendances and what impact these may have had. This is particularly relevant in the analyses of frequent attenders. Also, as information was only collected from ED records, we were unable to evaluate the quality of care given to the patient by the hospital once they left the ED.
Details of attendances which resulted in death were deliberately excluded as it was felt that in these cases there was no possibility of intervention by ED staff to prevent suicide. However, examining these attendances (particularly in cases where the patient was conscious on arrival) could have provided useful information about the level of care received at the ED. Previous research has indicated that improved medical management of self-poisoning may have the potential to reduce suicide.18
Implications
We found that a significant proportion (over 40%) of a clinical sample who died by suicide attended an ED in the year prior to death, and some individuals attended particularly frequently. Although psychiatric services clearly have a prominent role in preventing suicide in mental health patients, EDs may represent an important additional setting for suicide prevention. The majority of attendances prior to suicide were for self-harm or to request psychiatric help, and clinicians should be alert to suicide risk associated with such presentations.
All people who attend the ED following self-harm should receive a psychosocial assessment at triage and a more detailed assessment if required,13 but this study and several others16 19–21 show that this is not happening. Although a busy ED triage may not be the ideal setting for such an assessment, patients report a positive response to assessments when conducted in an appropriate manner,19 and assessment is also vital for identifying future risk of further self-harm or suicide.22 In order to communicate the importance of psychosocial assessment and to ensure that assessments are conducted appropriately, ED staff may require specific training in how to deal with patients following self-harm.8 13 19 22 Training should also address any negative attitudes staff have towards self-harm as this can have a negative impact on assessment and treatment.2 15 23
As well as ensuring that patients attending the ED receive adequate assessment, ED staff could also play a role in reducing suicide risk by facilitating adequate follow-up care. Although 73% of patients who attended the ED following self-harm were admitted for further treatment and only 4% were discharged without follow-up, 34% of those requesting psychiatric help were discharged without referral. Follow-up care of patients following self-harm or a suicide attempt has been shown to reduce future attempts and visits to the ED.8 22 This may be particularly relevant for frequent attenders.
The present study also highlights the possible association between frequent attendance and future suicide. Frequent attenders may represent a high-risk group,5 24 25 and this should be recognised by emergency services. Closer liaison with general practitioners and mental health services to ensure appropriate and consistent management of these often complex patients when they attend the ED may be of benefit. Such an approach requires ED staff to be able to access information about mental health diagnoses and care plans issued by other agencies and adequate information sharing between the different agencies. Previous studies have highlighted the need for a more coordinated approach to care between hospitals and community health services,8 19 22 but further research is still required to identify the most effective strategies. In addition to frequent attendance, alcohol misuse and possibly unemployment may also be associated with increased risk of early death by suicide following attendance at the ED, and clinicians should be alert to these factors and their possible association with suicide risk.
Acknowledgments
We thank all participating Emergency Departments that allowed us access to medical records. The study was carried out as part of the National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. We thank the other members of the research team: Kirsten Windfuhr, Harriet Bickley, Jimmy Burns, Isabelle Hunt, Rebecca Lowe, Phil Stones, Pauline Turnbull, Sandra Flynn, Cathy Rodway, Alison Roscoe and Kelly Hadfield. We acknowledge the help of health authorities and trust contacts and consultant psychiatrists for completing the questionnaires.
References
Footnotes
Funding The work of the National Confidential Inquiry is funded by the National Patient Safety Agency.
Competing interests Declared. Professor Appleby was formally the National Director for Mental Health and is now National Clinical Director for Health and Criminal Justice, England. Professor Navneet Kapur is Chair of the Guideline Development Group for the new NICE guidelines in the self-harm.
Ethics approval This study was conducted with the approval of the North West Multi-centre Research Ethics Committee, 02/8/74.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey