Article Text

Abstract
Background A third of the world's population does not engage in recommended levels of physical activity (PA), leading to substantial health and economic burdens. The healthcare sector offers a variety of resources that can help counsel, refer and deliver PA promotion programmes for purposes of primordial, primary, secondary and tertiary prevention. Substantial evidence already exists in support of multipronged PA counselling, prescription and referral strategies, in particular those linking healthcare and community-based resources.
Methods The Exercise is Medicine (EIM) initiative was introduced in 2007 to advance the implementation of evidence-based strategies to elevate the status of PA in healthcare. In this article, we describe the evolution and global expansion of the EIM initiative, its components, their implementation, an evaluation framework and future initiative activities.
Results Until now, EIM has a presence in 39 countries with EIM Regional Centers established in North America, Latin America, Europe, Africa, Southeast Asia, China and Australasia. The EIM Global Health Initiative is transitioning from its initial phase of infrastructure and awareness building to a phase of programme implementation, with an emphasis in low-to-middle income countries, where 80% of deaths due to non-communicable diseases already occur, but where a large gap in research and implementation of PA strategies exists.
Conclusions Broad implementation of PA counselling and referral systems, as clinical practice standard of care, has the potential to improve PA at the population level by complementing and leveraging other efforts and to contribute to achieving global targets for the reduction of inactivity and related morbidity and mortality.
- Physical activity promotion in primary care
- Health promotion through physical activity
Statistics from Altmetric.com
Introduction
Physical inactivity is a leading cause of death worldwide.1 It increases the risk of major non-communicable diseases (NCDs) such as coronary heart disease, type 2 diabetes and breast and colon cancers, responsible in 2008 for an estimated five million deaths or about 9% of the total global premature mortality.2 In 2010, almost one-third of the world population was categorised as being physically inactive.3 Accordingly, given its high prevalence, health burden and societal costs, the World Health Assembly has recently adopted combating physical inactivity as a priority objective for global action to help control the rising burden of NCDs.4 ,5 However, much work is needed if these global policies are to be translated into effective priorities for healthcare and public health systems at the local level.
Overall, several evidence-based approaches to increase physical activity (PA) at the population level have been identified, ranging from workplace and community to policy and environmental interventions.6 ,7 However, these interventions have all shown modest effect sizes, and therefore no single intervention will solve the world's inactivity problem.8 Rather, reducing physical inactivity most likely requires more comprehensive solutions, including a ‘whole of society’ approach.9 In addition, efforts are needed to maximise the potential benefits of setting-specific interventions, under a coordinated multisectoral approach.10
The healthcare sector offers a variety of resources, settings and a workforce that can help counsel, refer and deliver PA promotion programmes for individuals of all ages, for purposes of primordial, primary, secondary and tertiary prevention.11 Over the years, different strategies have been used to implement PA into healthcare settings. These include brief PA advice,12 advice plus written PA prescriptions, behavioural change and follow-up tools, also known as ‘green prescriptions’13 ,14 and referral of patients to community-based PA resources, also known as exercise referral programmes.15 Systematic literature reviews have found mixed evidence on the efficacy of PA counselling in healthcare settings, in part due to the use of multiple distinctive approaches, heterogeneous interventions and methodological shortcomings across clinical trials.15–19 However, substantial evidence already exists, with more continuing to emerge, in support of multipronged PA counselling, prescription and referral strategies, in particular those linking healthcare and community-based resources, which have been recently summarised.20
Recognising that PA promotion in the healthcare setting continues to evolve, the Exercise is Medicine (EIM) initiative was introduced to advance the implementation of evidence-based approaches and strategies to elevate the status of PA in primary healthcare.21 Established in late 2007 by the American Medical Association and the American College of Sports Medicine (ACSM), and subsequently coordinated by ACSM, the initiative's overarching goal is to make PA a standard part of the medical paradigm for the prevention and treatment of NCDs in healthcare systems.22 Specifically, EIM calls for PA to be considered by all healthcare providers as a vital sign in every patient visit,23–25 and for patients to be effectively counselled and referred for their PA and health needs. The core principles and strategies of the EIM initiative are based on effective interventions and include elements of the ‘green prescription’ and exercise referral approaches, linking the healthcare and community-based worlds for PA promotion.20 In this article, we describe the evolution and global expansion of the EIM initiative and its components, ongoing implementation and evaluation plans and future initiative activities.
The launch and growth of EIM as a Global Health Initiative
Approximately 2 years after the 2007 launch of EIM in the USA and the establishment of the EIM Center at ACSM's Indianapolis-based headquarters, representatives from scientific, public health and medical associations of several countries requested the EIM Center to expand its initial scope beyond the USA and begin a multinational collaboration to make EIM a global effort. Thus, the EIM Center was renamed the EIM Global Center, with an initial strategy being to build global awareness and help create a global infrastructure to catalyse widespread implementation of PA promotion in healthcare settings, with a particular focus on physicians and other healthcare providers (HCPs). To this end, in the initial 3 year globalisation period (2010–2013), the EIM Global Center has identified key partners across the globe and established seven EIM Regional Centers in North America, Latin America, Europe, Africa, Southeast Asia, China, Russia and Australasia. Each EIM Regional Center is responsible for providing guidance and coordination of EIM-related activities in their region and, when feasible and appropriate, supporting the establishment and continued growth of EIM in other countries in their region. This approach has been highly successful in helping ‘spread’ the EIM initiative globally. At the beginning of 2011, there were 15 countries with an EIM presence, whereas in September 2013 the number of EIM countries has grown to 39, as shown in figure 1.
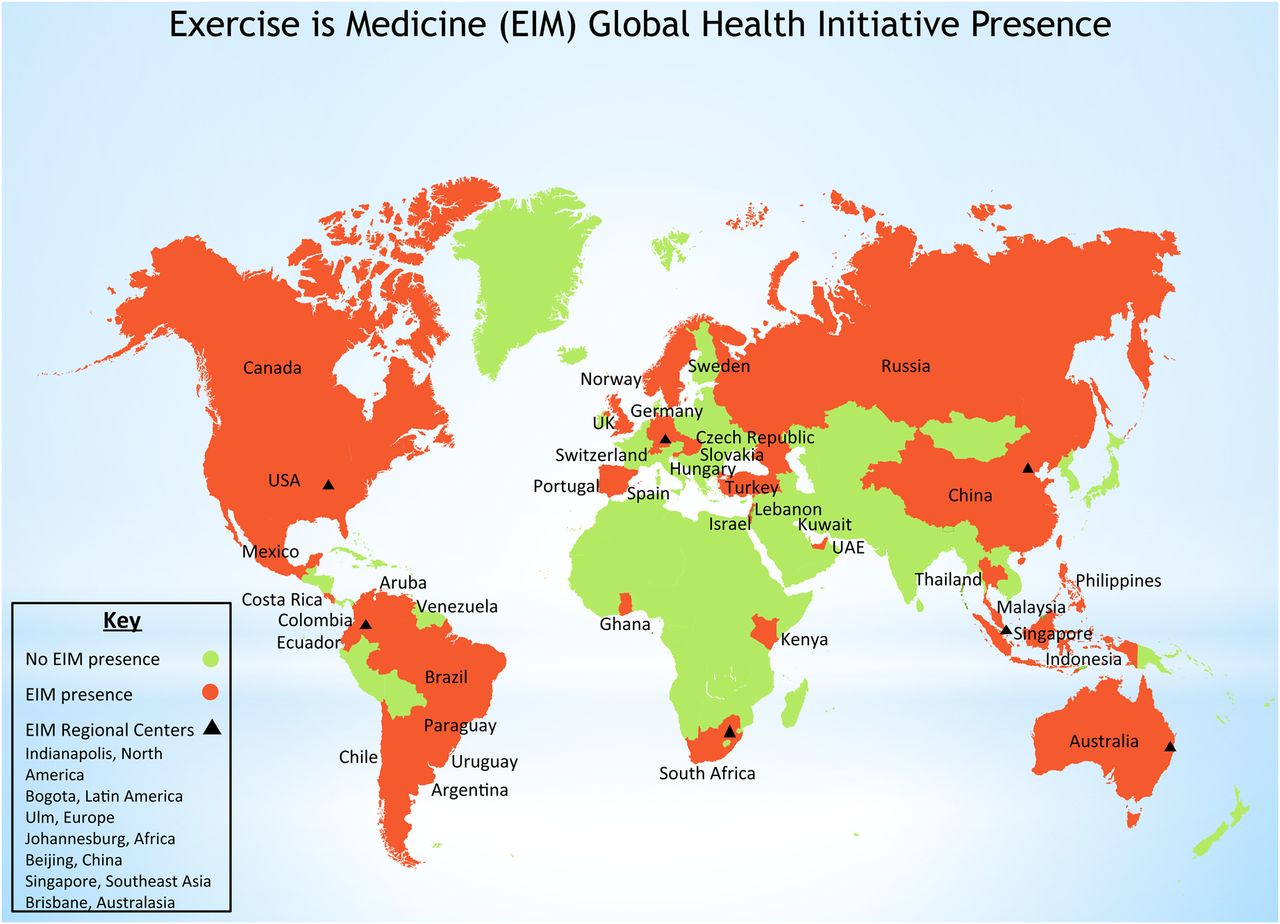
Exercise is Medicine (EIM) Global Health Initiative Presence.
The EIM Global Center has taken a multisectoral approach to drive the establishment of EIM National Task Forces (NTF) in each country. Each NTF is composed of representatives from a combination of the country's national primary care associations, other medical and healthcare associations (cardiology, endocrinology, sports medicine, nursing, nutrition/dietetics, physical therapy), physical education, academic institutions and, when possible, the Ministry of Health or National Public Health Institute. Close collaboration with media and industry partners and leveraging the expertise that they provide in key areas, such as public messaging, is also seen as critical and highly encouraged.
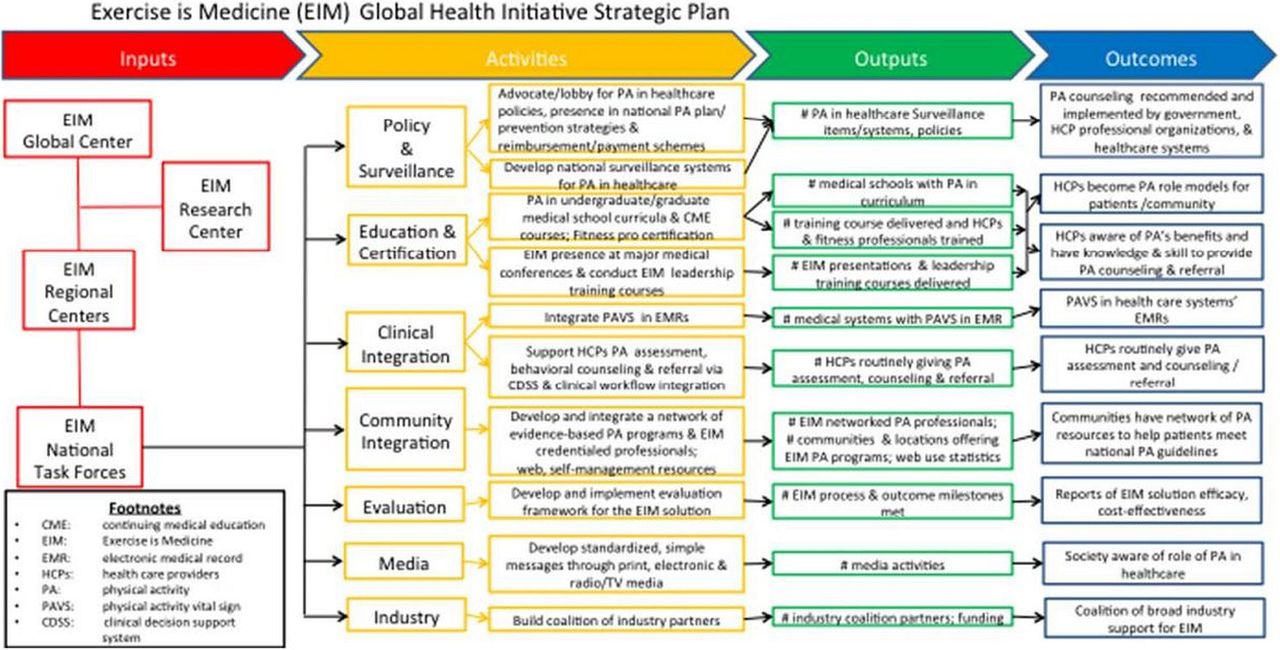
The EIM Global Health Initiative strategic plan for implementing the EIM Solution and associated NTF core activities is presented in figure 2. The main components of the EIM Solution (clinical integration and community programmes) are described in detail below, but in brief the aim is that activities in these two key areas will lead to the integration of a physical activity vital sign (PAVS) in electronic medical records (EMRs), the development of national networks of evidence-based community PA programmes and resources and a clinical decision support system linking the two, so that HCPs can provide behavioural PA counselling and refer patients to fulfil their PA ‘prescription’ in the community. To be optimally effective, however, it is also essential that the clinical and community integration activities being implemented be augmented by carefully targeted activities in the areas of policy and surveillance, evaluation, HCP education and fitness professional certification, as well as media and industry support. Funding for the EIM Global Health Initiative supports efforts to catalyse implementation of PA promotion in healthcare settings at the ground level and advance education, policy and surveillance work in this area. However, implementation efforts require demonstration projects at the local (ie, large hospitals/health systems), regional and national levels (ie, private and/or public health plans). The EIM Global Health Initiative provides support and guidance to EIM Regional Centers and NTFs to advance this agenda, including the process of obtaining resources for targeted implementation and evaluation of the EIM Solution. There are currently some implementation projects underway that will test several aspects of the EIM solution and explore their long-terms effects (beyond 12–24 months) and cost-effectiveness in the USA and in low-to-middle income countries, and we expect to publish these results once available. Funding for these demonstration projects has come from private and public research funds.
{kind=link}
{kind=link}
Exercise is Medicine (EIM) Global Health Initiative Strategic Plan.
Most countries require this ‘systems change’ approach to spark the necessary institutional and personal impetus for healthcare systems and HCPs, respectively, to break the barriers that impede the integration of clinical-community linkages for PA promotion. These include individual level barriers such as reluctance by HCPs to refer patients to community-based PA programmes. In addition, there is inadequate HCP training, self-efficacy and motivation to deliver PA counselling which we believe is key to the long-term success and sustainability of the EIM Initiative. For example, there is consistent evidence showing that physically active HCPs actually provide more and better PA counselling to patients.26 Other barriers include the lack of clear clinical-community linkages and programmes delivery infrastructure and policy barriers such as the lack of viable financial sustainability and innovative payment models for the clinical-community integration.20 If these changes are implemented in a feasible and sustainable fashion and on a sufficiently large scale, we believe they may have the potential to bring about increases in PA at the population level since PA promotion in clinical settings and referral schemes have proven effective in a variety of settings.8 ,12–20 ,27 There is also emerging evidence regarding its cost-effectiveness,28–32 early return on investment due to lower healthcare utilisation and costs,33 ,34 and sustainability if patient adherence can be maintained in ‘real-world’ scenarios.27 ,35
Evolution of the EIM Global Health Initiative—the EIM Solution
While the initial phase of the EIM Global Health Initiative (2010–2013) focused on raising awareness for the importance of integrated PA promotion in healthcare and the establishment of NTFs, the second phase of the initiative will revolve around the implementation of the EIM ‘Solution’. The EIM Solution is a standardised approach, informed by the available evidence,20 for assessing and prescribing PA in primary care and referring to local networks of community-based PA resources. The EIM Solution consists of five ‘steps’ that occur in three modules integrating clinical and community resources for PA promotion, via the use of health technology and decision support systems (see table 1).
The Exercise is Medicine Solution Model
Clinical module
The clinical module has three steps: PA assessment, PA prescription/behavioural counselling, and referral of patients to self-management or EIM-certified programmes and professionals. The first step of the EIM Solution, assessment of current PA levels, is achieved through the use of the PAVS,23–25 a tool designed to allow physicians, or members of their primary care team, to assess and record the PA levels of their patients in less than a minute. While more comprehensive PA assessment tools are available for use,36–38 the time demands placed on HCPs necessitate a simple and rapid PA assessment tool. The current EIM Solution PAVS consists of two questions: ‘On average, how many days per week do you engage in moderate to strenuous exercise (like a brisk walk)?’ and ‘On average, how many minutes do you engage in exercise at this level?’ (web appendix figure 3). These screening questions provide a snapshot of whether the patient is meeting current PA guidelines.39 ,40 The utilisation of the PAVS tool in the clinical setting is optimised in the practice workflow when it is integrated as a required response in the EMR system. The assessment of PA initiates further discussion between patients and HCPs about activity levels, their importance for health, NCD prevention and management and also enables the healthcare team to monitor changes in PA levels over subsequent medical visits. The PAVS was first implemented in clinical practice in 2010. It has recently been validated23 and its use linked to favourable changes in metabolic outcomes25 in a population of over one million adults in the Kaiser Permanente healthcare system in California.
The second step of the EIM Solution is for HCPs to provide patients with behavioural counselling using established tools such as shared decision making, the 5As and stages of change models,41 ,42 as well as an appropriate PA prescription. It is important to note that not all physicians or primary care providers may have the time, tools, medical system support or self-efficacy to provide extended PA behavioural counselling to patients in the clinical setting. Adapting to this reality, the EIM Solution provides medical systems the flexibility to incorporate allied health professionals that can provide behavioural counselling in the PA prescription/referral workflow. These professionals, sometimes referred to as PA intervention advisors, can serve an important role in ‘bridging’ the HCP's PA recommendations to the community referral system and providing patients with in-depth, personalised counselling and follow-up (web appendix figure 4). However, the spirit of the EIM Solution is for every patient to receive, at a minimum, a written prescription from their primary care provider to engage in recommended PA levels for health.21 ,22 ,39 ,40
Through the work of expert ACSM panels, more than 40 customised PA prescriptions and ‘Action Guides’ for a wide variety of illnesses, from NCDs to mental health, have been created to help HCPs provide a personalised PA prescription based on the patient's needs. Disease-specific prescriptions can be prepopulated in the EMR system (web appendix figure 5) to match the patient's NCD status (table 2) and delivered to patients during the medical visit or sent to them at a later time via mail or electronically, via the EIM integrated clinical decision support systems. These and other EIM tools can be freely accessed and printed by the HCP via the internet if they are not yet integrated in their EMR systems.21
EIM credential for PA and exercise referrals
In the third step of the clinical module, HCPs provide their patients with a PA referral to existing community-based PA resources, tailored to the patient's specific needs and health status (web appendix figure 6). Patients can be presented with three referral options to meet their individual needs: (1) self-management via web resources, (2) individual (one-on-one) consultation with an EIM-certified fitness professional and (3) EIM-certified classes that include behaviour modification and group-based PA. For those who wish to work independently, clients can be engaged in evidence-based self-management programmes available through the internet, mobile applications and print-based materials. For patients seeking more structured guidance, the referring HCP can direct them to the local network of EIM certified professionals and programmes.
The EIM Solution clinical module implementation will vary in each medical system or clinician's group (web appendix figure 4). NTFs can adapt their implementation based on the target population, practice environment, presence of allied health professionals, team care approaches and the availability of EMRs and technology. This is a critical step to fully integrate EIM's clinical decision support system to assess, prescribe, counsel and refer patients based on their PA needs and preferences. In particular, among clients with NCDs and risk factors, the EIM prescription and referral components are individualised according to a simple algorithm based on recognised preparticipation PA risk tools and the potential need for supervised exercise43–47 (table 2). This information is then embedded in the clinical decision support system to facilitate the individualised PA prescription and referral process (web appendix figures 5 and 6). Rather than ‘over-medicalising’ PA promotion, the EIM Solution strives for a balanced approach to offer every person touched by the healthcare system, including those apparently healthy but inactive as well as those with NCDs, a simple PA public health message based on current recommendations,39 ,40 which can be furthered tailored based on the patient's individual needs and health status.
The community module—development of a community referral network
The fourth step of the EIM Solution takes place as part of the community module. In this module, community resources are identified, catalogued and, if necessary, furthered developed. This is to provide a network of EIM-certified professionals and programmes so that HCPs can quickly identify and refer their patients to appropriate, locally existing resources (web appendix figure 7). This step is analogous to the model of a network of community-based pharmacies to which HCPs can send their patients to fill their drug prescriptions. A second essential part of the community module is the development of qualified EIM professionals, who will also populate the EIM referral network. NTFs may again customise the EIM Solution for their needs by determining national requirements for the PA programmes and professionals to whom HCPs can refer patients. In the USA, to ensure an adequate level of quality in PA counselling and training, ACSM has recently created the EIM Credential—a process targeted at qualifying health fitness professionals to receive patient referrals at one of three risk categories, based on their education and current certification levels (table 2). Details on the nature and how to obtain the various levels of the EIM Credential can be found elsewhere.48 The educational content and test of competency that form the basis of the EIM Credential can be a useful basis on which NTFs can build their own national networks for patient referrals. The development of the EIM Credential, or similar certifying process, is an essential step in establishing a network of fitness professionals that can command and maintain a high level of trust from participating HCPs and healthcare systems in countries where EIM is being implemented.
Step 5: active health technology
The fifth step of the EIM Solution is the incorporation of active health technology into the patient care model. The use of active health technology is an important step in providing patients with real-time feedback as they engage in their selected EIM programmes. Objective PA assessment tools (pedometers, accelerometers, smartphone applications, etc) can help monitor patients as they progress through their PA programmes. As patients are monitored, they can be provided with real-time feedback (ie, automated reminders, cues for action) to continuously assist them in filling their EIM prescription. Additionally, active health technology can be used to record and modify future PA sessions, as well as provide feedback on progress made over the course of the programme. The use of active health technology will also enable linkage between self-care and community programmes with the patient's healthcare team. Data collected from individual or group-based sessions (ie, intensity, duration and frequency of activity) can be relayed back to the patient's medical record, using health information privacy standards, allowing HCPs to take an active role in discussing health and fitness improvements made from one medical visit to the next (web appendix figure 8).
An overview of the EIM solution execution, as well as its clinical, community and active health technology modules and five steps, is provided in a flowchart format (web appendix figure 4).
EIM education and training programmes
Training of HCPs (ie, physicians, nurses, physician assistants, case managers, fitness professionals, etc) has been identified as a primary focus for the EIM Global Health Initiative. The majority of countries and global organisations affiliated with EIM are targeting their initial efforts on providing PA education and training for HCPs (ie, physicians continuing medical education (CME) training) and EIM health professionals (ie, fitness professionals, case managers). To assist in the initiative's global expansion, the EIM Global Center is currently working to develop standardised training and assessment protocols for different HCP groups. The EIM training programmes will provide NTFs with a flexible series of options in conducting training courses for their healthcare workforce in the essentials of PA for health, PA prescription as well as behavioural counselling strategies. Until now, the Latin America Regional Center has trained more than 1200 physicians and other HCPs in seven different countries in the region, using an 8 h CME course, with plans to scale up this process. A similar course has been piloted by the Southeast Asia and China NTFs. As outlined in the EIM's strategic framework (figure 2), NTFs will assess foundation, process and primary indicators associated with EIM education and training activities. Foundation indicators might include PA in the undergraduate and graduate education of HCPs or an analysis of the national guidelines and recommendations for the PA training of HCPs. Process indicators could include the number of training courses conducted and the number of HCPs certified at the training courses. Finally, primary indicators will assess HCP outcomes such as knowledge, attitudes, behaviours and practices (both personal and professional) and the long-term impact that these changes have on patient counselling and PA levels.
EIM solution evaluation framework
As the EIM Global Health Initiative transitions to a second phase of development, the focus now shifts to establishing an evaluation framework that provides a set of metrics that allow for: (1) a critical examination of the processes involved in the establishment of the EIM Solution model, (b) an analysis of the effectiveness of the EIM Solution in increasing PA levels and improving health outcomes in the short term and long term (beyond 12–24 months) and (c) a series of standardised indicators that will allow for comparisons across the different countries participating in the EIM network. Given the global scope of EIM, it is necessary to develop a flexible model that can be easily adapted for application in a wide variety of healthcare systems at the local, regional and national levels, allowing for the varied regional and national characteristics in which the EIM Solution is being implemented.
With this in mind, a multilevel framework of indicators, following the example of previous Institute of Medicine evaluation models,49 has been recommended to serve as an objective measure of progress in the global implementation of EIM, as outlined in the EIM strategic plan (figure 2). The indicators suggested for inclusion in the EIM evaluation model can be grouped into three general categories: foundation, process and primary indicators (table 3). Together, these indicators will assess the progress towards the overarching goal of EIM, increased PA levels in targeted population, as well as improvements in body composition and other inactivity related NCDs and risk factors. As the EIM Solution is implemented across a healthcare system, consideration of these indicators is essential in assessing its successful implementation and progress towards achieving the overarching goals of the initiative.
Overview of the EIM Solution evaluation framework
Looking towards the future
A third of the world's population does not engage in recommended levels of PA3 and the associated health2 and economic50 burdens of inactivity and inaction51 are substantial. In collaboration with partners and colleagues facing similar barriers to implementing and sustaining PA promotion in healthcare settings, over the past 3 years there has been a rapid growth in the network of HCPs and healthcare systems around the globe interested in the EIM approach. The EIM Global Health Initiative is now transitioning from its initial phase of infrastructure and awareness building to a phase of programme implementation, evaluation and dissemination of the EIM solution, coupled with continued strategic growth. A particular emphasis for EIM implementation is in low-to-middle income countries where most people live and where 80% of deaths due to NCDs already occur,2 but where a large gap in research and implementation of PA strategies exists.52 The EIM Global Health Initiative will also become a forum to learn from previous successful experiences and ongoing efforts using clinical-community linkages for PA promotion that have been implemented in several countries including New Zealand,53 Wales,27 ,54 Sweden,55 Switzerland56 and Brazil57 ,58 among others.
Despite progress in the field of PA promotion in healthcare,17 ,19 ,20 much is still lacking. More translational research is needed for the large-scale implementation of PA promotion in healthcare in different settings, populations and healthcare systems. In particular, issues around the long-term effectiveness, adherence and sustainability of these programmes need to be addressed. While the integration of PA into healthcare is a recognised strategy in a few nations’ formal public health strategies,10 ,11 ,59 more policy efforts are needed throughout the globe. Finally, the field still lacks a comprehensive global monitoring and surveillance framework and an adequately trained health workforce to ensure adequate implementation. Integrating PA counselling and referrals via clinical-community linkages around the globe is a complex process that will benefit from an academic hub to coordinate efforts and provide scientific direction to the EIM global health initiative. Therefore, the Initiative will establish the EIM Research Center to initiate and collaborate on projects in the areas of translational research, programme design and evaluation, economic analyses, workforce training, policy and development of surveillance and monitoring frameworks. These activities constitute a critical step in the successful implementation and scale-up of the EIM initiative in the USA and globally.
It is essential to continue to globally build strong, compelling cases on improved health outcomes and potential healthcare cost containment derived from the integration of the proven benefits of PA into routine healthcare. Evidence supports a multisectoral approach to PA promotion that includes governments, NGOs, academic institutions and industry, to accelerate the deployment of PA strategies to help prevent and treat the global epidemic of obesity and other NCDs.8 ,9 Broad implementation of PA counselling and referral systems, as a clinical practice standard of care, has the potential to improve PA at the population level by complementing and leveraging others PA promotion efforts and contributing to achieving the recently agreed upon global targets to reduce the prevalence of inactivity and NCD morbidity and mortality.4 In the context of an ‘all of the above’ and ‘whole of society’ approach, the EIM solution to integrated PA promotion in healthcare can be seen as an additional and relevant piece of the global public health solution to inactivity.
What are the new findings?
-
Broad implementation of evidence-based strategies for physical activity (PA) promotion via counselling and referral systems, as a clinical standard of care, has the potential to help reduce population inactivity rates and related non-communicable diseases morbidity and mortality.
-
The Exercise is Medicine (EIM) global health initiative can help accelerate the integration of PA promotion in healthcare settings by aiding the establishment of an infrastructure of policy, surveillance, training and implementation research activities in this area.
How might it impact on clinical practice in the near future?
-
Assessment of PA as a vital sign and integration of clinical-community linkages for PA referral are likely to be increasingly used, in particular with the aid of electronic medical records.
-
EIM and other evidence-based, cost-effective, prevention-oriented strategies are likely to be increasingly implemented in healthcare systems around the world in response to the growing disease and economic burden associated with non-communicable diseases.
Acknowledgments
The authors would like to acknowledge the scientific and programmatic contributions provided by the global EIM network, including EIM's staff and Advisory Board, the EIM Regional Centers and National Task Forces, the EIM Network Builders Solutions Team and EIM's global partners: The Coca Cola Company, Technogym, Anytime Fitness and DUNK. In particular, they would like to acknowledge the following representatives of the global EIM network: Dr Robert E Sallis—Chair, EIM Advisory Board, Dr John Duperly—Director, Latin American EIM Regional Center, Dr Jürgen M Steinacher—Director, European EIM Regional Center, Dr Boris Polyaev, Director, Russian EIM National Center, Dr Louis J Holtzhausen—Director, African EIM Regional Center, Dr Wenhua Zhao—Director, Chinese EIM Regional Center, Dr Ben Tan—Director, Southeast Asian EIM Regional Center, Mr Chris Tzarimas—Director, Australasian EIM Regional Center, Mr Phil Trotter—Director, Network Builders Solutions Team.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors FL, MS and AH wrote different sections of the article and all authors reviewed and approved the submitted article. AH is the guarantor.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.