Article Text

Abstract
Background: Statins, antiplatelet drugs, β-blockers and ACE inhibitors may produce marked benefits in secondary prevention of ischaemic heart disease (IHD), especially in combination.
Objective: To examine trends in treatment and factors associated with treatment using a population-based general practice database.
Design: Analysis of routinely collected computerised data from 201 general practices using iSOFT software contributing to the DIN-LINK database.
Setting and patients: Subjects aged ⩾35 years and registered with the practices; on average, 30 000 men and 21 000 women with IHD each year.
Main outcome measure: Percentage of subjects with IHD receiving individual drugs and combined treatment in any given year.
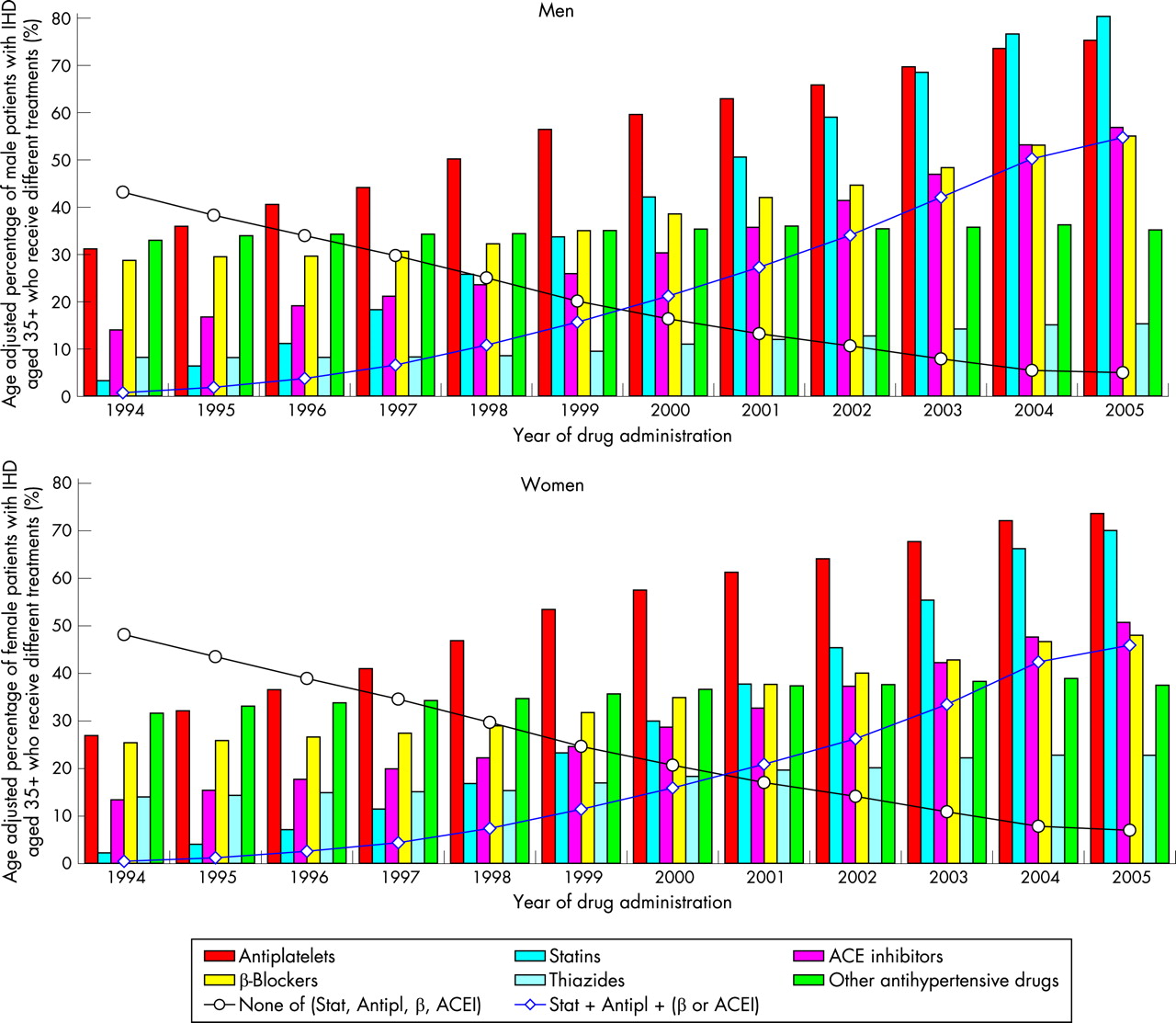
Results: Between 1994 and 2005 use of drugs for secondary prevention increased markedly. By 2005, 80% of men and 70% of women were receiving a statin, 75% and 74% were receiving antiplatelet drugs, 55% and 48% were receiving β-blockers and 57% and 51% were receiving an ACE inhibitor; 55% of men and 46% of women were receiving a statin, antiplatelet drug and either β-blocker or ACE inhibitor, of whom just under half were receiving all four classes of drug. Gender differences were largely explained by more severe disease in men. In 2005, subjects less likely to receive combination therapy were older, had not had a myocardial infarction or revascularisation, and lacked comorbidities such as diabetes or hypertension.
Conclusions: Despite high levels of statin and antiplatelet prescribing, opportunities exist for increasing the benefits of secondary prevention, especially through the wider use of combined treatments. Future targets could usefully include combination therapy.
Statistics from Altmetric.com
Secondary prevention of ischaemic heart disease (IHD) is recognised as an important and achievable goal, emphasised by the publication in 2000 of a National Service Framework (NSF) setting standards in this area for the UK1 and reinforced by the introduction in primary care of Quality and Outcomes Framework (QOF) targets.2 In patients with established IHD, risks of recurrent events and death are high and are reduced by treatment with specific drugs. Recently it has been argued that combined treatments including antiplatelet drugs, statins and blood pressure lowering drugs (particularly β-blockers and ACE inhibitors), may produce very marked benefits in IHD prevention,3 perhaps reducing risk by about 75%.4 The case for their use in secondary prevention is strong5 and supported by observational evidence in a primary care setting.6 The case for using several blood pressure lowering drugs in combination at lower doses has also been persuasively argued.7 However, information on the extent of use of treatment combinations is limited. Using a large UK primary care database we report (a) trends in secondary preventative treatment of IHD, focusing on both individual and combination therapy and (b) patient and other factors associated with such treatment. In particular, we examine the role of age, sex, a socioeconomic marker and the role of comorbidities on the likelihood of combination therapy.
METHODS
DIN-LINK
DIN-LINK is a continuing anonymised computerised UK primary care database from practices that use iSOFT (formerly Torex) software from 1989 onwards. This report is based on 201 practices that run an updated version of the software used in an earlier version of the database, previously described.8 9 We have outlined methodology for identifying good-quality data in DIN-LINK,8 and the selected practices had to provide at least 5 years of continuous high-quality data.
The completeness and accuracy of DIN-LINK data have been demonstrated by comparisons with other national data sources. The practices and GPs in DIN-LINK are as comparable to the UK norm as the practices and GPs in other GP research databases.8 9 Morbidity and drug data are coded using Read codes. A sociodemographic indicator at a small area level, the ACORN index,10 has been linked to individual patient records based on the postcode in which a person lives. This process was carried out within practices before the linked data were downloaded in order to preserve anonymity. Multiple levels of aggregation of the index are available, but commonly, the most aggregated level—a five-level classification from “wealthy achievers” through to “hard pressed” is used. From the 201 practices, ACORN scores were available for most patients in 177 of these. Practice region and urban/rural status is also known. Lack of ACORN data for a practice arises from difficulties in electronic communication with the practice and is unrelated to the type of practice or patient. We also analysed the English Index of Multiple Deprivation (IMD; linked via postcode in a similar manner to ACORN), but do not present data as results were similar and for technical reasons it was available for fewer practices and only those in England.
Subjects
People aged 35 years and over and registered with the practice on 31 December and for 6 months previously contributed to that year’s denominator. IHD status was derived from diagnostic Read codes in the electronic records, each person being assigned to one of four categories based on the most severe status recorded thus far: non-specific IHD Read codes, angina, myocardial infarction (MI), coronary artery revascularisation. Read-coded diabetes and hypertension comorbidities were also extracted. Diabetes was further classified by the presence of treatment in 2005 (“insulin”, “oral” if only oral hypoglycaemic drugs were prescribed, or “diet” if no drug was prescribed).11
For subjects in each year, prescriptions were identified for (a) antiplatelet drugs; (b) statins; (c) angiotensin converting enzyme inhibitors or angiotensin receptor antagonists (ACEI); (d) β-blockers; (e) thiazide diuretics and (f) other antihypertensive drugs (British National Formulary categories: 2.6.2. and 2.5, except 2.5.5.1 and 2.5.5.2).
Statistical methods
Treatment rates for each year were directly standardised for age to the 2005 population for men and women separately, using four age groups (35–64, 65–74, 75–84, ⩾85). Our analysis of combination therapy primarily focused on three-combination treatment, defined as the presence of statins, antiplatelet drugs and β-blockers or ACEI in a given year. Further analyses examined four-combination therapy (all four of statins, antiplatelet drugs, β-blockers and ACEI in a year) and five-combination therapy (defined as four-combination therapy and a diuretic or other antihypertensive drug in the year).
Factors predicting the prescription of three-combination treatment in 2005, in patients with a history of IHD, were analysed by fitting a hierarchical logistic model with practices being at “level 2” and individual patients at “level 1”; in effect, practice was being treated as a random effect. Factors investigated were age, sex, type of IHD, ACORN and IMD scores, history of hypertension and diabetes, and urban–rural status and region of practice. An interaction between sex and IHD type was also added, to allow for treatment rates by type of IHD to differ by sex. Analyses using different outcomes (“no treatment”, “number of drugs”) were also carried out. All regressions were performed using PROC GENMOD in SAS version 9.1 for Solaris (SAS Institute, Cary, NC, USA).
RESULTS
On average, 30 000 men and 21 000 women were identified as having IHD each year, based on any previous occurrence of specific IHD Read codes in a patient’s record (table 1). Age-adjusted prevalence of recorded IHD increased steadily from 1994 (7.57% men, 4.88% women) to 2002 (8.28% men, 5.49% women), before falling to its 2005 levels (8.14% men, 5.24% women) (table 1). This trend was also seen in practices providing data throughout (data not shown). Of these patients, men were almost twice as likely to have an MI or revascularisation—a trend that remained consistent over time (in 2005 61.5% of male IHD was classed as MI/revascularisation compared with only 36.6% of female IHD). Individually, the revascularisation group showed the highest relative increase between 1994 and 2005 (male revascularisation increased from 12.6% to 28.3% of all male IHD, female from 3.2% to 11.2%).
Trends in secondary prevention 1994–2005
Use of individual secondary prevention drugs has steadily increased, markedly so for statins, antiplatelet drugs and ACEI (fig 1 and supplementary data). From 1999, β-blocker usage also increased. Use of thiazides and other antihypertensive drugs remained largely unchanged. The greater use of thiazides in women appears due to treatment of coexisting hypertension and IHD (data not shown). The (age-adjusted) percentage of patients receiving no preventative treatment declined in men and women between 1994 and 2005 (from 43.2% to 5.0% in men, and from 48.2% to 7.0% in women), in contrast to the marked rise in the proportion of patients receiving combined therapy; three-drug combined therapy rose from 0.8% to 54.7% in men and 0.5% to 45.9% in women (see table 1 and supplementary data).
{kind=link}
Subjects with angina (or non-specific IHD) were consistently less likely to receive three-drug combination therapy than those with a history of MI or revascularisation (in 2005 44.7% vs 61.0% for men and 39.1% vs 57.7% for women; table 1).
The prevalence of four-drug combined therapy (antiplatelet + statin + beta-blocker + ACE inhibitor) rose from 0.1% in 1994 to 25.9% in men and 19.2% in women in 2005, while the percentage receiving five-drug combined therapy (adding a third antihypertensive drug) was 11.1% in men and 10.1% in women in 2005. To establish that the antihypertensive drugs given as part of the four- and five-drug combinations were actually being given together rather than as alternatives at different times of the year we reviewed a random sample of individual records for 2005; 80–90% of subjects were correctly classified. We also assessed the consistency of classification between 2004 and 2005. Of 2886 men and 1839 women classified as receiving five-combination therapy in 2004 (and registered in 2004–5), the majority (2145 men (74%) and 1278 women (69%)) were again so classified in 2005, while of the remainder 296 (10%) men, 196 (11%) women were classified as four-combination and 264 (9%) men and 182 (10%) women as three-combination therapy.
Factors predictive of combination therapy in 2005
Table 2 summarises the factors predicting the probability of receiving at least three-combination treatment in 2005. While men were significantly more likely to be receiving three-combination treatment (OR = 1.42, table 2), this difference was reduced after adjustment for other factors such as age and IHD type (adjusted OR = 1.09 95% CI 1.04 to 1.14). Moreover, there was clear evidence that the sex difference varied by severity of IHD diagnosis (table 2, bottom). Thus, while three-combination therapy was more probable among men with non-specific IHD (OR = 1.14), it was less likely in men than in women with an MI (OR = 0.90) or revascularisation (OR = 0.84).
Patients with a history of hypertension (OR = 1.50–1.76) or any type of diabetes (OR = 1.23–1.73) were more likely to be receiving three-combination treatment. Our socioeconomic markers (ACORN shown in table 1) showed no association with prescribing. The IMD (data not shown), which was available only for English practices, also showed no association. Region and rurality showed weak statistically significant associations, with three-combination therapy being slightly more likely in more northern regions (OR = 1.11 vs southern regions, 95% CI 1.00 to 1.24) and in rural practices (OR = 1.09 vs inner city practices, 95% CI 0.95 to 1.26).
Results were very similar if we used four- or five-drug combination therapy as the outcome.
DISCUSSION
Between 1994 and 2005, the use of medications for secondary prevention of IHD (particularly statins and antiplatelet drugs) increased markedly. By 2005, 80% of men and 70% of women were receiving a statin, while 75% of men and 74% of women were receiving antiplatelet drugs. The use of combination treatment also increased, so that by 2005 55% of men and 46% of women were receiving a statin, antiplatelet and either a β-blocker or ACEI; just under half of each group were receiving all four drugs. Law et al have argued that low-dose combination treatment with blood pressure lowering drugs increases efficacy and reduces side effects7; though this analysis was based on an analysis of primary prevention trials, the case was made for treatment of raised blood pressure using such an approach in high-risk groups. It is therefore encouraging that at least 10% of both men and women were receiving an antiplatelet, a statin, a β-blocker, an ACEI and a third antihypertensive drug in 2005. Review of individual patient records suggested that the majority of patients in the four-and five-combination groups were prescribed these combinations together and not at different times during the year. This interpretation is reinforced by the consistency of the treatment categories from one year to the next.
What is perhaps surprising is that the increase in preventative therapy has been steady throughout the period, suggesting no sudden impact of either earlier guidelines or of the NSF. It is perhaps too early to assess the full impact of the QOF since this would only have affected 2005 figures.
While women were less likely to receive treatment, especially combination therapy, our analyses highlight that this is not true for women with severe disease; women with an MI or revascularisation were more likely than such men to receive combination therapy. We have previously suggested that this may be related to initiation of treatments in secondary care.12 Reasons for differences in treatment between the sexes appear to be more subtle than the unfair gender discrimination that has been suggested.13–15
Our data emphasise that those aged over 75 are less likely, and those over 85 much less likely, to receive combination therapy. This is consistent with previous reports, which found statins, β-blockers and ACEI less likely to be prescribed in older patients.15 16 It is apparent that the treatment gap is greatest in older subjects where the event rate is also highest and thus the greatest mortality benefits may be gained.
Patients with hypertension or diabetes were more likely to have their IHD aggressively treated than patients without these comorbidities. This is unsurprising, given the increased risk of further IHD events of these patients. The absence of any significant association with socioeconomic status is consistent with previous work on statins in DIN-LINK,12 on statins and treatment of hypertension in the Health Survey for England,17 18 and on statins in the British Regional Heart Study,19 and emphasises the equity of provision of treatment in primary care in the National Health Service. Similar results have been reported from Spain20 and Scotland.15 Interestingly, the small but statistically significant association between region and probability of combination therapy is the opposite of that expected if it were postulated that generally less affluent areas would be less likely to receive optimal treatment.
This study provides a population perspective on use of secondary prevention, and is not limited to use of therapies in patients recently seen in secondary care. It is therefore not surprising that the prescribing rates are lower than in EUROASPIRE II.21 Results of EUROASPIRE II suggested that in 2000 the UK was ahead in prescribing of statins, but behind in prescribing other medicines.21 However, one population based study of 16 694 patients with IHD registered with a French Farmers Insurance Fund in 200422 reported lower prevalence rates for statins, antiplatelet drugs and ACEI and similar rates of β-blockers to those of our study. It is difficult to assess how representative of France this large study was. The French study was based on medications bought and reimbursed, whereas our study is based on prescriptions issued. Few population-based surveys exist from other European countries for comparison. There is a strong case for setting up a European collaboration which would be able to present routinely collected data for different countries and which would allow fair comparisons of how drug therapies are being delivered under different healthcare systems.
Our study has several strengths. All patients, by definition, are known to general practitioners, and all registered with a practice are included (eliminating non-response bias), while recording of prescriptions issued is virtually complete. The large number of practices provides ample statistical power and geographic representation.
Two potential limitations require comment: the representativeness of DIN practices and the accuracy of Read codes for identifying subjects with IHD. In the past we noted that the DIN population has an identical age–sex structure to the national average and documented the very similar rates of IHD diagnosis and of statin prescribing for secondary prevention of IHD in GPRD practices.8 12 The Read codes we used are essentially those used in QOF, but supplemented by inclusion of revascularisation codes. A study from 2001 in one practice suggests that such an approach can be both sensitive and specific.23 The criteria used to identify patients with IHD have been influenced by the introduction of QOF. We have recently identified how GPs have systematically reviewed IHD codes to coincide with the introduction of the QOF targets.24 The impact of this on rates of secondary treatment of IHD will probably have been to accentuate slightly the rise in treatment rates from 2003 on. Curiously, this is a period when the rise in secondary prevention rates has slowed. This may be because we are reaching saturation in the prescribing of statins and antiplatelets and suggests a need to focus on combination therapy.
Finally, it needs to be recognised that it is unrealistic to expect 100% of patients to receive all medications. For example, a very few patients will be sensitive to aspirin and β-blockers may be contraindicated in some patients with asthma. This is recognised within the QOF system where exception reporting is allowed and the highest target is 90%.2
CONCLUSIONS
Prescribing of antiplatelet and statin drugs is at a high level in the UK. However, there is still scope for improvement in secondary prevention by increasing use of β-blockers, ACEI and other blood pressure lowering drugs in patients who can tolerate them. The greatest scope for improvement is in those patient groups least likely to receive treatment—older patients and those with less severe disease. Primary care has an important role because such patients are less likely to be in contact with secondary and tertiary care services. Future updates to the NSF could usefully include combination therapy as a target. The case for wider availability of combined preparations, to increase coverage and compliance, needs consideration.
REFERENCES
Supplementary materials
web only table 94/1/83
Files in this Data Supplement:
Footnotes
Competing interests: NR is a director of Cegedim Strategic Data, which markets DIN-LINK data to pharmaceutical companies.
Ethics approval: Ethical approval for use of the DIN-LINK database for this project was given by the Wandsworth research ethics committee.
Funding: This project was funded by the BUPA Foundation. The Wellcome Trust funded the development of the database. SDeW is part funded by a grant from Cegedim.