Article Text

Abstract
Objectives: In January 2007, opt-out HIV testing replaced provider-initiated testing at the sexually transmitted infections (STI) outpatient clinic in Amsterdam, The Netherlands. The effect of the opt-out strategy on the uptake of HIV testing was studied and factors associated with refusal of HIV testing were identified.
Study Design: Data routinely collected at the STI clinic were analysed separately for men who have sex with men (MSM) and heterosexuals. Logistic regression analysis was used to identify factors associated with opting out.
Results: In 2007, 12% of MSM and 4% of heterosexuals with (presumed) negative or unknown HIV serostatus declined HIV testing. Refusals gradually decreased to 7% and 2% by the year end. In 2006, before the introduction of opt-out, 38% of MSM and 27% of heterosexuals declined testing. The proportion of HIV-positive results remained stable among MSM, 3.4% in 2007 versus 3.7% in 2006, and among heterosexuals, 0.2% in 2007 versus 0.3% in 2006. In both groups factors associated with opting out were: age ⩾30 years, no previous HIV test, the presence of STI-related complaints and no risky anal/vaginal intercourse. Among heterosexuals, men and non-Dutch visitors refused more often; among MSM, those warned of STI exposure by sexual partners and those diagnosed with gonorrhoea or syphilis refused more often.
Conclusions: An opt-out strategy increased the uptake of HIV testing. A sharp increase in testing preceeded a more gradual increase, suggesting time must pass to optimise the new strategy. A small group of visitors, especially MSM, still opt out. Counselling will focus on barriers such as fear and low risk perception among high-risk visitors considering opting out.
Statistics from Altmetric.com
Before highly active antiretroviral therapy (HAART) was introduced, HIV testing in The Netherlands was performed only on request because knowledge of positive HIV status had meagre advantages. Once HAART was generally available, the Dutch strategy changed from testing on request to provider-initiated testing for certain risk groups. Despite this change, 20–40% of persons infected with HIV in The Netherlands are unaware of being infected, a proportion similar to the rest of Europe (30%).1–3
The sexually transmitted infections (STI) outpatient clinic of Amsterdam’s Health Service offers free STI/HIV screening, counselling and treatment. At the end of 2000, it started provider-initiated HIV testing for all clients during STI consultations. HIV testing increased from 15% in 2000 to 40% in 2004 for men who have sex with men (MSM) and from 30% to 56% for heterosexual individuals. The introduction of HIV rapid testing in 2005 increased the uptake to 47% among MSM and 62% among heterosexuals.4 To increase uptake further, an “opting out” strategy was initiated in January 2007. The HIV test is now part of routine STI screening, and all visitors are tested for HIV unless they decline. In this study, we describe our first-year experience with the opt-out strategy in a large STI clinic. First, we place the recent uptake of HIV testing in the context of a larger time period. Second, we evaluate the effect of the new strategy on the uptake and the proportion HIV-positive diagnoses, comparing 2006 and 2007. Third, we identify factors associated with refusal of testing and explore self-reported reasons for opting out.
METHODS
Study setting and clinic routine
The STI outpatient clinic in Amsterdam annually performs approximately 26 000 new consultations, providing 35% of the total reported STI/HIV consultations and diagnosing 50% of the new HIV infections found in Dutch STI clinics.5 6 Sociodemographic data on all visitors are registered in an electronic patient database. After registration, a distinction between high and low-risk visitors is made by asking six triage questions. Visitors are accordingly assigned to a standard or short STI screening protocol.7 All MSM are defined as high risk and are assigned to a standard protocol, as are heterosexual individuals with STI-related complaints or a warning of STI exposure by a sexual partner, commercial sex workers, individuals from sub-Saharan Africa without health insurance and women reporting anal sex (see fig 1). Visitors are informed about the screening procedures. Since January 2007 the main reason for actively refusing the HIV test is recorded in the electronic patient database.

Number of visitors and HIV opt-out/opt-in results in 2007 at the sexually transmitted infections (STI) outpatient clinic, Health Service of Amsterdam. MSM, men who have sex with men.
The standard screening protocol includes taking a detailed sexual history and giving pre and post-test counselling. During physical examination, material for STI and HIV diagnostics is collected. The short screening protocol includes taking a short sexual history, sampling blood and instructing patients in the self-collection of urine (men) or a vaginal swab (women).
Visitors assigned to the standard protocol receive their rapid HIV test result after 30–45 minutes, with a preliminary STI diagnosis. Those assigned to the short protocol receive their results after one week. Visitors in both groups obtain their definite STI/HIV results after 7 days.
All newly HIV-diagnosed patients receive post-test counselling and are immediately referred to their general practitioner or to an HIV treatment centre for further diagnosis, treatment and care.
Laboratory procedures
Each visitor was tested for hepatitis B, syphilis, Chlamydia trachomatis and gonorrhoea. In addition, in the standard protocol, direct microscopy on Gram stain and wet mounts is performed for gonorrhoea, non-specific urethritis and trichomoniasis. In the case of ulcerative diseases, microscopy and PCR are performed for the detection of Treponema pallidum and herpes simplex virus (HSV) types 1 and 2. Laboratory procedures for STI are detailed elsewhere.8
In the standard protocol, a rapid HIV immunoassay (Abbott Determine HIV 1/2; Abbott Diagnostic Division, Hoofddorp, The Netherlands) is used, with a result after 15 minutes. Before March 2007, positive rapid HIV immunoassays were confirmed by the ELISA test (HIV 1/2, Abbott Diagnostics) and from March 2007 onwards using the HIV Ag/Ab Combo test (Axsym; Abbott Laboratories, North Chicago, Illinois, USA; Abbott Determine HIV 1/2, Abbott Diagnostics). If the rapid HIV test is negative but the visitor recently experienced high-risk sexual contact or presents with HIV-related symptoms, the HIV Ag/Ab Combo test is also performed in order to identify early infection. In the short protocol all visitors are tested by ELISA (HIV 1/2, Abbott Diagnostics) until March 2007, and from March 2007 onwards by the HIV Ag/Ab Combo test (Axsym; Abbott Laboratories). Reactive samples are confirmed by immunoblot (Line Immuno Assay, Inno-Lia HIV I/II Score; Innogenetics NV, Ghent, Belgium).
Statistics
First we described the number of new consultations and the uptake of HIV testing, separately for MSM and heterosexuals, using routinely collected data from all clinic visitors from 1995 to 2007.
Second, we calculated the proportion HIV-positive diagnoses among all visitors with a previous negative test result or unknown HIV status in 2006 and 2007. Results were compared using the χ2 test.
Logistic regression analysis was used to examine factors associated with opting out in 2007. This was done separately for MSM and heterosexuals in the standard protocol, and for heterosexuals in the short protocol. Sociodemographic variables examined included gender, sexual orientation, ethnicity and age. For the visitors in the standard protocol, variables related to STI/HIV screening included: being notified of exposure by a partner; STI-related complaints; working as a commercial sex worker; HIV test history; current STI diagnosis and sexual risk behaviour. Sexual risk was categorised as: (1) no or only protected vaginal/anal intercourse; (2) vaginal/anal intercourse without a condom with a steady partner; (3) vaginal/anal intercourse without a condom with a casual partner; or (4) vaginal/anal intercourse without a condom with both types of partners. Heterosexuals in the short protocol are not queried on sexual behaviour.
A multivariate logistic regression model was constructed by a stepwise backward procedure including all variables and checking for confounding. In addition, we evaluated reasons for opting out. For the reasons “fear” and “low risk perception” a multivariate logistic regression model was also constructed by a stepwise backward procedure that considered the same variables mentioned earlier. In general, a p value of less than 0.05 was considered statistically significant. In the final model, we examined interactions between variables. All analyses were conducted using the statistical package SPSS 15.0.
RESULTS
HIV test uptake and proportion of HIV-positive diagnoses
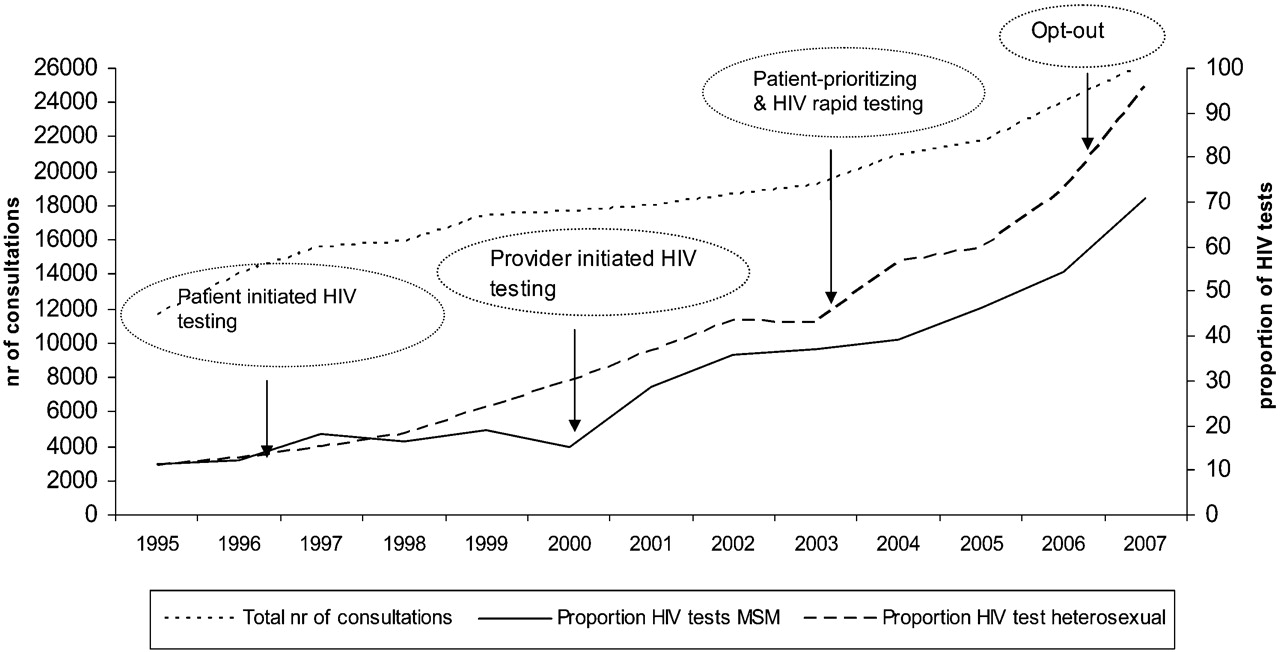
From 1995 to 2007, the annual number of new consultations increased from 11 656 to 26 217. The proportion of consultations including an HIV test increased from 11% to 71% among MSM and from 11% to 96% among heterosexuals (fig 2).

Number of new consultations and proportion of HIV testing among men who have sex with men (MSM) and heterosexual visitors, 1995–2007, sexually transmitted infections outpatient clinic, Amsterdam and its various HIV testing policies.
Excluding individuals already aware of their positive HIV status, the overall HIV test proportion was 95% in 2007.
In 2007, of the 26 217 consultations, 957 (3.7%) were of patients already aware of being HIV positive (935 MSM and 22 heterosexuals). Of the remaining 25 221 new consultations, 3927 (16%) were made by MSM and 21 332 (85%) by heterosexuals (fig 1).
Among MSM, uptake in 2006 was 62% (2535/4116) versus 88% (3442/3927) in 2007. According to risk assessment based on the triage questions, 50% (10 707 new consultations) of the heterosexuals (48% men, 52% women) were assigned to the standard protocol. Among heterosexuals in the standard protocol, 64% (6452/10 130) tested for HIV in 2006 versus 94% (10 034/10 689) in 2007. Among heterosexuals in the short protocol 83% (7615/9211) tested for HIV in 2006 versus 98% (10 434/10 641) in 2007.
The increase in HIV test uptake was observed in both MSM and heterosexuals, regardless of age. In the first month of the new strategy, testing increased sharply, then continued to rise more gradually until the year end. Among MSM, it rose from 82% in January 2007 to 93% in December 2007 and among heterosexuals, from 94% to 98% (fig 3).

{kind=link}
{kind=link}
{kind=link}
Proportion of consultations including an HIV test for men who have sex with men (MSM) and heterosexuals, 2006–7, sexually transmitted infections outpatient clinic, Amsterdam.
The proportion of HIV-positive diagnoses remained stable (0.8% in 2006 and 0.7% in 2007). The proportion among MSM was 3.7% (95/2525) in 2006 and 3.4% (117/3442) in 2007 (p = 0.47); among heterosexuals, 0.3% (36/14 067) in 2006 and 0.2% (44/20 468) in 2007 (p = 0.44). The total number of new HIV-positive diagnoses increased by 25% from 131 in 2006 to 161 in 2007 (MSM 94 to 117; women 17 to 29; heterosexual men 19 to 15). In 2007, 30% (49/161) of those newly diagnosed had not been tested for HIV before: 20% (23/117) of the MSM and 59% (26/44) of the heterosexuals.
Factors associated with opting out for HIV testing
Men who have sex with men
Table 1 shows the determinants of opting out among MSM. In multivariate analysis, variables independently associated with opting out were older age and never being tested before. Older MSM opted out 2.6–4.1 times more often than MSM under 30 years of age. Those never tested opted out four times more often than those tested before. Remarkably, MSM with STI-related complaints (odds ratio (OR) 2.08, 95% CI 1.68 to 2.57), warning of STI exposure by a sexual partner (OR 1.85, 95% CI 1.39 to 2.45), or diagnosed with gonorrhoea (OR 1.76, 95% CI 1.29 to 2.41), infectious syphilis (OR 1.73, 95% CI 1.02 to 2.93), or non-specific proctitis (OR 1.64, 95% CI 1.04 to 2.57) were likewise inclined to refuse HIV testing. MSM with bisexual contacts were less likely to opt out compared with exclusively homosexual MSM (OR 0.41, 95% CI 0.27 to 0.60). MSM who reported unprotected anal intercourse opted out less often than those reporting no risky intercourse.
Heterosexuals at increased risk (standard protocol)
Table 2 shows determinants of opting out among heterosexuals at increased risk of STI who were assigned to the standard testing protocol. In multivariate analyses, men were more likely to opt out than women (OR 1.39, 95% CI 1.16 to 1.67). Also sub-Saharan African ethnicity (OR 1.88, 95% CI 1.36 to 2.58), no previous HIV test (OR 1.53, 95% CI 1.29 to 1.80) and STI-related complaints (OR 1.66, 95% CI 1.37 to 2.0) were associated with opting out. Visitors aged 30 years or older had an odds of 1.35–2.03 to opt out compared with that of younger visitors. Those reporting unprotected vaginal or anal intercourse opted out less often than those reporting no risky intercourse.
Heterosexuals at low risk (short protocol)
Multivariate analyses among heterosexuals at low risk of STI in the short protocol showed that heterosexuals aged between 40 and 49 years (OR 2.11, 95% CI 1.29 to 3.47) were more likely to opt out than those aged 30 years or less. Also heterosexuals who never tested for HIV before were more likely to decline (OR 1.48, 95% CI 1.12 to 2.00) than those with a test history.
Barriers for HIV testing
Table 3 shows that fear is the most common reason for opting out, both among MSM (40%; 179/450) and heterosexuals (36%; 216/609 in the standard protocol, 37% 62/168 in the short protocol). Furthermore, 12% (52/450) of the MSM and 22% (133/609) of the heterosexuals considered themselves at no or low risk of HIV, and 21% (95/450) of MSM and 7% (44/609) of heterosexuals reported testing HIV negative more than 3 months ago.
MSM whose main reason for opting out was fear were more likely to be never tested before (OR 2.19, 95% CI 1.47 to 3.26) and more often warned of STI exposure by a sexual partner (OR 1.74, 95% CI 1.03 to 2.94) or presenting with STI-related symptoms (OR 2.00, 95% CI 1.32 to 3.02) compared with those opting out for other reasons. MSM opting out because of a low risk perception reported less unprotected anal intercourse with casual partners (OR 0.16, 95% CI 0.05 to 0.56), but were three times more likely to be diagnosed with a chlamydia infection during the consultation (OR 3.08, 95% CI 1.32 to 7.20).
Heterosexual visitors in the standard and short protocol who reported fear as the main reason likewise tended to be older than 30 years and never tested before. Those in the standard protocol reported more unprotected vaginal intercourse with casual partners and were more likely to be of sub-Saharan African or northern African ethnicity than those reporting other reasons. Heterosexuals in the standard protocol with a low risk perception reported no unprotected vaginal intercourse or only with a steady partner, or they were engaged in commercial sex work.
DISCUSSION
In our large STI outpatient clinic, the opting out strategy increased the uptake of HIV testing from 71% in 2006 to 95% in 2007. The absolute number of new HIV-positive diagnoses increased by 20% and the proportion of HIV-positive diagnoses remained stable (0.8% vs 0.7%). A small group at high risk of HIV, especially MSM, continues to decline the HIV test. A previous study at our clinic observed an association between low HIV testing rates and high-risk young MSM.9 In 2007, however, this association was no longer found. MSM most likely to opt out were those with a relatively high risk of HIV exposure (aged ⩾30 years, not tested before, STI-related complaints and warned of STI exposure by a sexual partner) and those with a relatively low risk of HIV (protected anal intercourse). In addition, MSM reporting fear as the main reason for opting out were also more likely to have no previous testing, STI-related complaints and warning of STI exposure. Those opting out because of a low risk perception reported less sexual risk but were diagnosed more often with C trachomatis compared with MSM opting out for other reasons. This finding suggests we should be careful using self-reported sexual behaviour as a measure for being at risk of STI/HIV and is in favour of the opting out strategy because it avoids risk estimations based on reported behaviour either by clinic staff or visitors.
Key messages
An opt-out strategy for HIV testing is effective in increasing the uptake of testing and awareness of HIV status in a sexually transmitted infections (STI) clinic.
Identification of personal barriers for HIV testing is important in order to improve pre-test counselling to high-risk visitors still intending to opt out.
Opting out for HIV testing should be implemented in all STI screening clinics in Europe and considered for high-risk groups visiting other healthcare facilities.
Data from another study at our clinic, an unlinked biannual cross-sectional HIV prevalence survey in 2007, showed that the small group of MSM who opt out had a much higher HIV prevalence (2/27; 7.4%) than those who opt in (4/280; 1.4%; p = 0.09), indicating the public health importance of this group (data not shown). These MSM will be a challenge for counselling, but the opting out strategy frees more pre-test counselling time to explore personal barriers. Clinic staff started to discuss the practices that best support the visitors who consider opting out.
It is conceivable that high-risk MSM are avoiding the clinic due to the new opt-out strategy, or that visitors aware of their HIV-positive status might opt out to conceal it. However, if opting out has truly declined, it may show that time must pass to optimise a new HIV testing strategy. The gradual decrease in opting out, after the initial rapid drop, probably reflects normalisation of the HIV test for visitors and for staff. Similarly, we saw increased testing among visitors in the short protocol when the triage system reduced pre-HIV test counselling.5 However, at the clinic we can only partly decrease personal barriers such as fear of personal and social consequences, so some will always decline testing.10 11
Opting out is not a standard HIV testing strategy in Europe. Interestingly, in 2006 the British government strongly recommended the opt-out approach for all STI (genitourinary medicine) clinics in the UK.12 The results on uptake following the opt-out approach varied among the clinics.13–15 Last year, finding many MSM and African migrants still unaware of their HIV status, the British HIV Association recommended the approach be extended to all relevant clinic settings in the UK. Also routinely testing for patients in secondary care should be considered and recommended to all high-risk patients.16 17
In 2007 the Dutch advisory committee on active testing and counselling determined that implementation of the opt-out strategy is cost-effective if the HIV prevalence is 0.2%, based on previous Centers for Disease Control and Prevention calculations.18–20 The observed prevalence at the STI clinic of Amsterdam is 0.7%. We argue that the benefits of introducing opting out at STI outpatient clinics, by increasing HIV diagnoses, even outweigh the presumed negative consequences of testing visitors not belonging to a standard risk group. Among low-risk heterosexuals assigned to the short protocol we found a prevalence of 0.1%.
An opt-out strategy for HIV testing should be introduced in all STI clinics in Europe. Also, a more pro-active testing approach or even an opting out strategy, targeting high-risk groups should be extended to other healthcare facilities, such as general practitioners and emergency departments.21 Conditions should include guidelines for professionals and for patients a guaranteed and timely access to follow-up. Finally, at our STI outpatient clinic we will focus counselling on barriers such as fear and low risk perception among high-risk visitors to decrease opting out further and increase awareness of their HIV status.
Acknowledgments
The authors thank the personnel of the Amsterdam STI outpatient clinic for their contribution in the daily implementation of the opting out strategy and data collection; Nicole Dukers for help during implementation; Ronald Geskus for statistical advice; Maarten Schim van der Loeff for his comments and Lucy Philips for editing.
REFERENCES
Footnotes
Competing interests: None.
Contributors: RLJH analysed and interpreted the data and drafted the manuscript; JSAF and RAC contributed to the idea and the manuscript; EvL and HFJT contributed to the acquisition of data; IGS and MP supervised the study, the interpretation of data and contributed to the final manuscript.
Linked Articles
- Brief encounters