Article Text

Abstract
Background Anticipatory prescribing (AP) of injectable medications in advance of clinical need is established practice in community end-of-life care. Changes to prescribing guidelines and practice have been reported during the COVID-19 pandemic.
Aims and objectives To investigate UK and Ireland clinicians’ experiences concerning changes in AP during the COVID-19 pandemic and their recommendations for change.
Methods Online survey of participants at previous AP national workshops, members of the Association for Palliative Medicine of Great Britain and Ireland and other professional organisations, with snowball sampling.
Results Two hundred and sixty-one replies were received between 9 and 19 April 2020 from clinicians in community, hospice and hospital settings across all areas of the UK and Ireland. Changes to AP local guidance and practice were reported: route of administration (47%), drugs prescribed (38%), total quantities prescribed (35%), doses and ranges (29%). Concerns over shortages of nurses and doctors to administer subcutaneous injections led 37% to consider drug administration by family or social caregivers, often by buccal, sublingual and transdermal routes. Clinical contact and patient assessment were more often remote via telephone or video (63%). Recommendations for regulatory changes to permit drug repurposing and easier community access were made.
Conclusions The challenges of the COVID-19 pandemic for UK community palliative care has stimulated rapid innovation in AP. The extent to which these are implemented and their clinical efficacy need further examination.
- end of life care
- drug administration
- home care
- terminal care
- supportive care
- nursing home care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Anticipatory prescribing (AP) is the prescribing and dispensing of injectable medications in advance of clinical need, for visiting nurses or doctors to give as required if symptoms (pain, nausea and vomiting, agitation and respiratory tract secretions and breathlessness) arise in the final days of life.1–3 AP may optimise symptom control for deaths in the community1 4–8: it is well established and widely recommended in the UK, New Zealand and Australia,1–3 9–12 and less commonly in the USA, Singapore and Norway.13–16
The number of people dying in care homes and at home has risen dramatically during the COVID-19 pandemic in the UK and in many other countries.17 18 AP guidance and practice has changed in response.1 5–7 19 There is alarm about depleted drug stocks and that nurses and doctors may not be readily available to give injections.5 20 Recent UK guidance proposed both family caregiver administration and use of different drug formulations via the buccal, rectal or sublingual routes along with traditional subcutaneous injections.5–7 21
The evidence base for current AP practice is sparse,2 3 9 16 22–26 even more so for the buccal or sublingual routes, which are based primarily on professional experience and within paediatric palliative care.13–15 27
Family caregivers have rarely administered AP medications in the UK.27–29 Australian experience suggests family caregivers appreciate being able to provide symptom relief: some struggle with the responsibility10 30 31 and/or worry it is a form of euthanasia.10 Media concerns have focused on family caregivers having a great responsibility but without adequate training or oversight.20
To support practitioners and policy-makers, we surveyed UK/Ireland professionals and investigated how AP practice has changed in response to revised national guidance and local demands during the COVID-19 pandemic.
Aims and research questions
With regard to AP practice during the COVID-19 pandemic, what do practitioners report in relation to
Changes in drug prescription?
Changes in drug administration?
Changes in support structures for AP?
Suggestions for further changes?
Methods
An online survey (see online supplementary appendix) was developed in Survey Monkey based on the literature, our own clinical experience and SB’s recent correspondence with palliative care and primary care colleagues across the UK. The study was reviewed by the University of Cambridge Psychology Research Ethics Committee (PRE.2019.013)
Supplemental material
After a local pilot, an email with the survey link was sent between 8 and 13 April 2020 to delegates who attended AP workshops in 2019 for doctors, nurses and pharmacists in palliative and primary care; members of the Association for Palliative Medicine of Great Britain and Ireland, the National Institute for Health and Social Care Excellence Medicines Associate Programme and Resilient GP Facebook Group, UK Queen’s Nursing Institute. Colleagues were encouraged to forward the survey link to interested colleagues, seeking a snowball sample of practitioners.32
All fields were mandatory and responses were anonymous unless respondents supplied their name and email address in the optional final field to indicate interest in a follow-up telephone interview.
Questions 1–4 sought demographic data concerning respondents’ geographical areas of work, professional roles, clinical work settings and involvement in AP. Question 5 addressed changes in AP practice (if any) during the COVID-19 pandemic. These included drug types prescribed, total quantities dispensed, drug doses/ranges, drugs and support documents in home/care home, route of administration especially sublingual/buccal, persons administering AP drugs (especially family or social care colleagues), advice and support for non-clinical administration, phone or video support, prescribing in non-COVID-related illness and syringe driver use. Reasons for any changes in practice were invited in free text. Question 6 invited comments and suggestions for changes in practice, policy and legislation to optimise AP.
Data analysis
The Checklist for Reporting Results of Internet E-Surveys was followed.33 Descriptive statistics were used for demographic and categorical response data. For free-text replies to Questions 5 and 6, BA, BB, IW and SB developed themes inductively from the data, allocating responses to themes developed for each subquestion.34 These are presented with illustrative quotations.
Results
Respondents
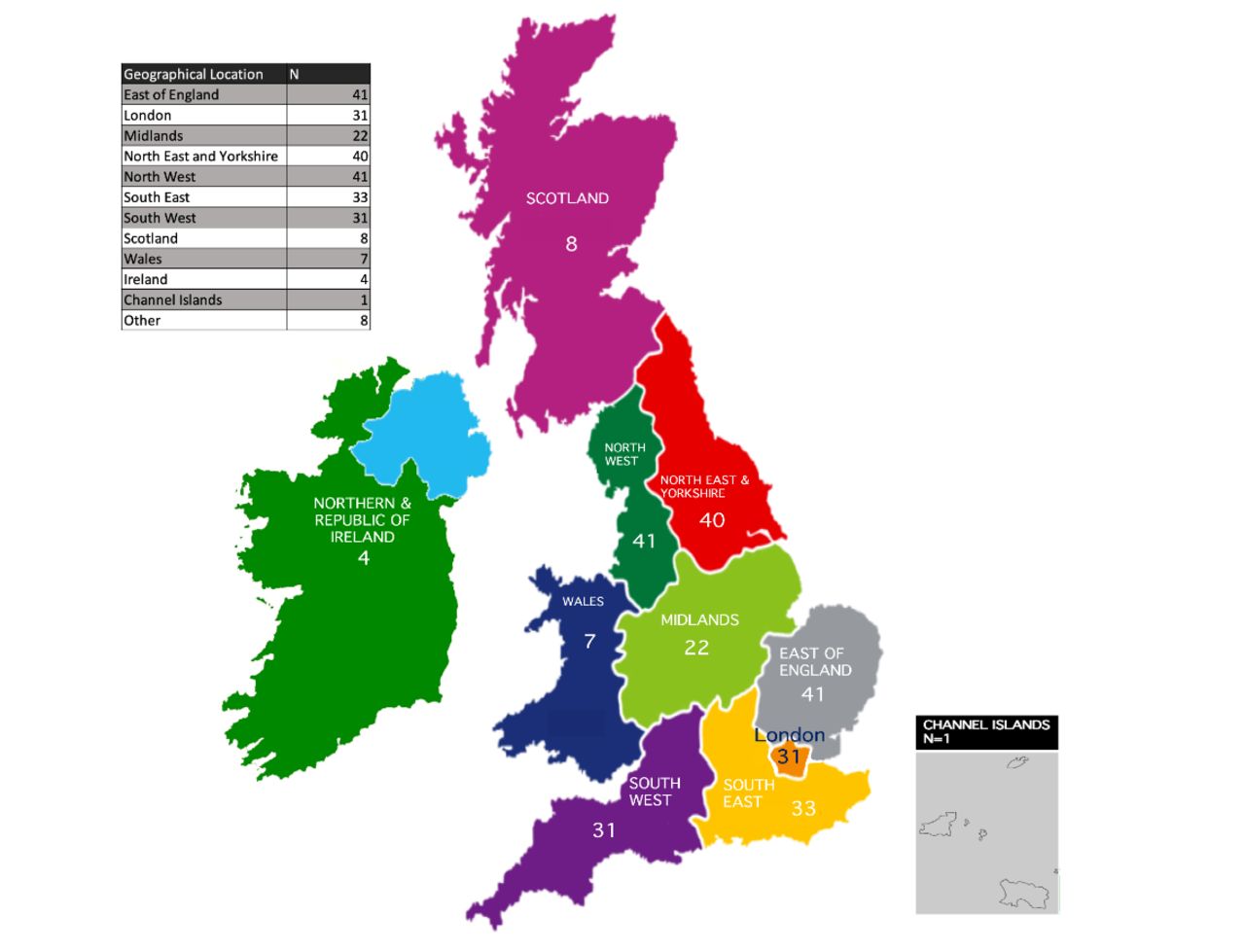
Two hundred and sixty-one replies were received between 9 and 19 April 2020, from palliative medicine consultants (CONS 97, 37%), general practitioners (GP 63, 24%), palliative care specialist nurses (CNS 31, 12%), general community nurses (8, 7%), palliative medicine trainees (15, 6%), other doctors (12, 5%), pharmacists (5, 2%), other nurses (4, 2%) and other professional group (16, 6%). The geographical distribution of respondents is shown in figure 1.
{kind=link}
Distribution of responders across Great Britain and Ireland.
Clinical work settings were community specialist palliative care (144, 55%), hospice inpatient unit (104, 40%), community primary care (96, 37%), hospital (87, 33%), care home (29, 11%) and other settings (7, 3%). All respondents were working clinically. Participants’ involvement in the AP process were decision to prescribe (239, 92%), prescribing (225, 86%), dispensing (12, 5%), monitoring before drug administration (99, 38%), medication administration (53, 20%) and medication disposal after death (13, 5%).
Changes in AP practice
Respondents’ reports of any changes in AP practice in their area, with examples from thematic analysis of the explanatory free text, are listed in table 1.
AP practice changes during COVID-19
Marked changes in AP were reported by about one-third in most domains. Changes in route of administration (47%) and drugs prescribed (38%) were associated with consideration of buccal, sublingual and transdermal routes and avoidance of subcutaneous injections. These related to possible administration by family or social caregivers (37%) and drug availability. Changes in quantities prescribed (35%) and doses/ranges (29%) reflected the reported needs of some dying with COVID-19 for higher doses and more frequent administration to control symptoms than previously (and to protect limited medication supplies). Changes were under way to facilitate drug delivery and relevant paperwork to the home (36%).
At the same time, clinical contact and patient assessment were changing to telephone or video rather than in person (63%). Telephone advice was more available (49%). Changes in prescribing for non-COVID-19 terminal illness (24%) reflected moves towards non-injectable routes and concern that they might develop COVID-19 and associated severe agitation. Planned reductions in syringe driver use (30%) reflected perceptions that the COVID-19 terminal phase is brief and best managed with ‘as needed’ individual doses and that both district nurses and syringe drivers might be in short supply.
Practitioners’ comments and suggestions for change
The dominant themes were calls for three changes in pharmaceutical legislation.
Permit repurposing of prescribed AP drugs in care homes
Allowing care homes to re-use AP medications when the patient has died and the drugs have not been used. Such a waste of meds. #209 CONS
COVID outbreak in nursing home we care for. Would be very useful if could re-use Anticipatory subcutaneous medications and also if the nursing home could hold a small supply. #227 GP
Enable wider ready access to drugs in the community
Nursing homes have asked for spare sets of anticipatory medications should patients unexpectedly become unwell, but this is not within the law. #142 GP
It would be really helpful to have a centralised stock of AP drugs (maybe with community nursing teams) so that each patient just has what they need dispensed when they need it. #170 GP
Having access 24 hours for anticipatory meds: prescription and meds in key localities to enable rapid response and symptom control. #119 CNS
Permit recycling of drugs returned to pharmacies
Enable unused vials to be taken back to pharmacy and reused. Fear of waste and cost are factors that limit the amount of AP in the community. #245 CONS
This is our opportunity to secure legislative change for the establishment of centralised supplies, the ability for clinical staff to have sensible safe boxes and for the return of safe, unused drugs to pharmacies … This is a known and appalling waste that must stop now and be permanent. There has never been a cogent justification. #100 CONS
Discussion
This study revealed rapid change in AP practice is under consideration in many areas of the UK/Ireland: increased use of alternative routes, changes in drugs prescribed to address stock shortages, new routes of administration, family caregiver administration; later prescribing of AP drugs and smaller quantities. There were calls to new pharmaceutical regulations to permit repurposing of AP medications in care homes, wider community drug access and recycling unused medications returned to pharmacies. Reflecting broader changes in community end-of-life-care during the pandemic, more end-of-life care in general and AP in particular is undertaken remotely and electronically, with increased 24 hours availability. These changes will potentially significantly affect care during the pandemic and in the future.
The main strengths of this study were the large number of responses, the broad distribution of replies from across the UK and Ireland and the contemporaneous data. Anonymity encouraged candid responses. It is not possible to calculate a response rate due to the snowball sampling.
Major changes are under way in routes of AP drug administration; community adult end-of-life care practice is increasingly accepting the buccal and sublingual routes. Robust evidence is urgently needed about their pharmacokinetics to develop evidence-based guidelines on suitable drugs, preparations and doses which is currently based largely on clinical experience in paediatric palliative care. While transdermal administration is well established, it lacks the flexibility and rapidity of relief when symptoms are unstable in the dying.27 This is particularly important for those dying from COVID-19 in whom there is a need for higher drug doses and more frequent administration for effective symptom control.
Many areas are adopting proposals in national policies to consider caregiver drug administration.35 This is a big ask for family caregivers with significant risks for their psychological welfare. They may feel pressure to undertake clinical tasks; responsibility for medications heightens anxieties during an already emotional time.10 36 Nurses often worry about oversedating patients or accelerating death when they give end-of-life medications.3 23 Should a patient die shortly after family caregivers give a medication, they may have even greater concerns.10 37 Clinicians must be careful whom they approach to undertake these tasks, discuss alternative care options and ensure appropriate training and support is available for willing family caregivers.6 19 28 30 31 After death, family caregivers confront these worries while being isolated in their grief during the pandemic.19
Many palliative care services have responded to the pandemic with extended availability of telephone advice for clinical and social care colleagues, often now including patients and family members. These are welcome developments. The move of much community palliative care to remote video or telephone consultations is understandable due to the need to avoid infection risk to patient, family and clinician. However, this change risks impairing the quality of communication and clinical assessments involved. Video diagnosis of the dying phase and AP decisions, reported by participants, require remote consultation skills that may be more familiar to general practitioners than some working in palliative care services.
Pharmaceutical regulations and policies pertaining to AP in care homes arise from legitimate needs to protect residents from drug errors, particularly with controlled drugs like morphine and midazolam.38 39 The presence of suitable medications already in the homes, prescribed for one resident but then urgently needed for another, is frustrating for care home staff and visiting clinicians, as until recently they have been unable to repurpose drugs. Recent UK guidance, issued on 28 April 2020, now permits repurposing in care homes and hospices: this welcome development, called for by many participants, was introduced after data collection was complete.40 The related regulations requiring destruction of medications after death and on return to a pharmacy is as yet unresolved.39 These tensions are not new but more acute during the pandemic when many care home residents are at risk of dying from COVID-19 and drugs may be in short supply.5 A focus on preserving limited drug stocks may delay AP until an individual is close to the end of their life, but risks undermining ready drug availability, which is the essence of AP.
Respondents reported that some dying from COVID-19 have a relatively brief dying phase requiring larger than usual drug doses. This makes current guidance to prescribe drugs in small amounts and close to anticipated death problematic. Community clinicians are conflicted. Wider and more ready community drug access might ease this difficulty but presents legislative and logistical challenges.19
Conclusions
The COVID-19 pandemic is a challenge to community palliative care. It creates opportunities to innovate rapidly and learn from paediatric palliative care. Given the risk from face-to-face consultations and visits for drug administration, care is now more virtual and remote, with greater dependence on family caregivers to provide care and administer drugs, often via non-injectable routes. These changes are occurring at pace: it remains to be seen how widely they are implemented, how effective they are and how much they will persist after the pandemic. We would welcome collaborations with colleagues across the world to address these important questions.
Acknowledgments
The authors wish to express their gratitude to our colleagues across the UK and Ireland who completed the questionnaire at a time of intense time pressure. We also wish to acknowledge the support of Prof Bee Wee (NHS England National Clinical Director for End of Life Care) and Dr Amy Proffitt (Vice-President of Association for Palliative Medicine) for their support of this study.
References
Footnotes
Twitter @B_CP_Antunes, @Ben_Bowers__, @IainDr
Contributors BA and SB designed and co-led the study: MPK, RB, RR, AS, IW and BB contributed to the survey design; BB supported dissemination of the online survey; BA, IW, BB and SB conducted the data analysis; BA, BB, IW and SB drafted the paper; all the authors reviewed and commented on the draft paper and have approved this final version.
Funding BA, IW and SB are funded by the National Institute for Health Research (NIHR) Applied Research Collaboration East of England (ARC EoE) programme. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. BB is funded by the National Institute for Health Research (NIHR) School for Primary Care Research.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement No data are available. This is a preliminary analysis of the interim dataset obtained by 19 April 2020. Data collection is ongoing: a further paper is planned in the future once further responses have been received and a more detailed analysis of the dataset has been undertaken.