Article Text

Abstract
We report baseline results of a community-based, targeted, low-dose CT (LDCT) lung cancer screening pilot in deprived areas of Manchester. Ever smokers, aged 55–74 years, were invited to ‘lung health checks’ (LHCs) next to local shopping centres, with immediate access to LDCT for those at high risk (6-year risk ≥1.51%, PLCOM2012 calculator). 75% of attendees (n=1893/2541) were ranked in the lowest deprivation quintile; 56% were high risk and of 1384 individuals screened, 3% (95% CI 2.3% to 4.1%) had lung cancer (80% early stage) of whom 65% had surgical resection. Taking lung cancer screening into communities, with an LHC approach, is effective and engages populations in deprived areas.
- lung cancer
Statistics from Altmetric.com
Introduction
The symptomatic presentation of lung cancer is typically associated with advanced disease and poor survival. Screening asymptomatic at-risk subjects with low-dose CT (LDCT) reduces lung cancer specific mortality by 20%.1 However, current smoking and low socioeconomic status (SES) are associated with reduced participation in lung cancer screening trials.2–4 Reducing barriers to participation in those at greatest risk is a critical challenge to screening implementation.5 To address this and the high burden of lung cancer in our local community, we designed and piloted a community-based, lung cancer screening service. The screening programme was developed around the concept of a one-stop ‘lung health check’ (LHC), which incorporated a holistic lung health programme and was located next to local shopping centres. The service was designed to minimise barriers to participation by reducing travel and increasing convenience/service accessibility. We selected screening participants according to individualised risk, using the PLCOM2012 model, at a 6-year lung cancer risk threshold of ≥1.51%.6 A similar approach was used in the UK Lung Cancer Screening Trial (UKLS), which selected participants based on 5-year risk ≥5% (Liverpool Lung Project model), this was cost-effective and resulted in a high prevalence of lung cancer.7
Methods
Ever smokers, aged 55–74 years, registered at participating general practitioner practices (n=14), were invited to a community-based LHC, where respiratory symptoms, spirometry and 6-year lung cancer risk (PLCOM2012) were assessed alongside smoking cessation advice8; anyone with a risk ≥1.51% was offered annual screening, over two screening rounds, including an immediate LDCT scan (online supplementary document for more detailed methodology). CT scans were reported by the National Health Service (NHS) Consultant Radiologists with an interest in thoracic radiology. Pulmonary nodules were managed in accordance with the British Thoracic Society guidelines adapted for an annual screening programme.9 Scan reports were categorised as negative, indeterminate or positive. Indeterminate results required a 3-month surveillance scan and positives immediate assessment in the rapid access lung cancer clinic. A false positive was any screened individual referred to the cancer clinic who was not diagnosed with lung cancer.
Supplementary file 1
Results
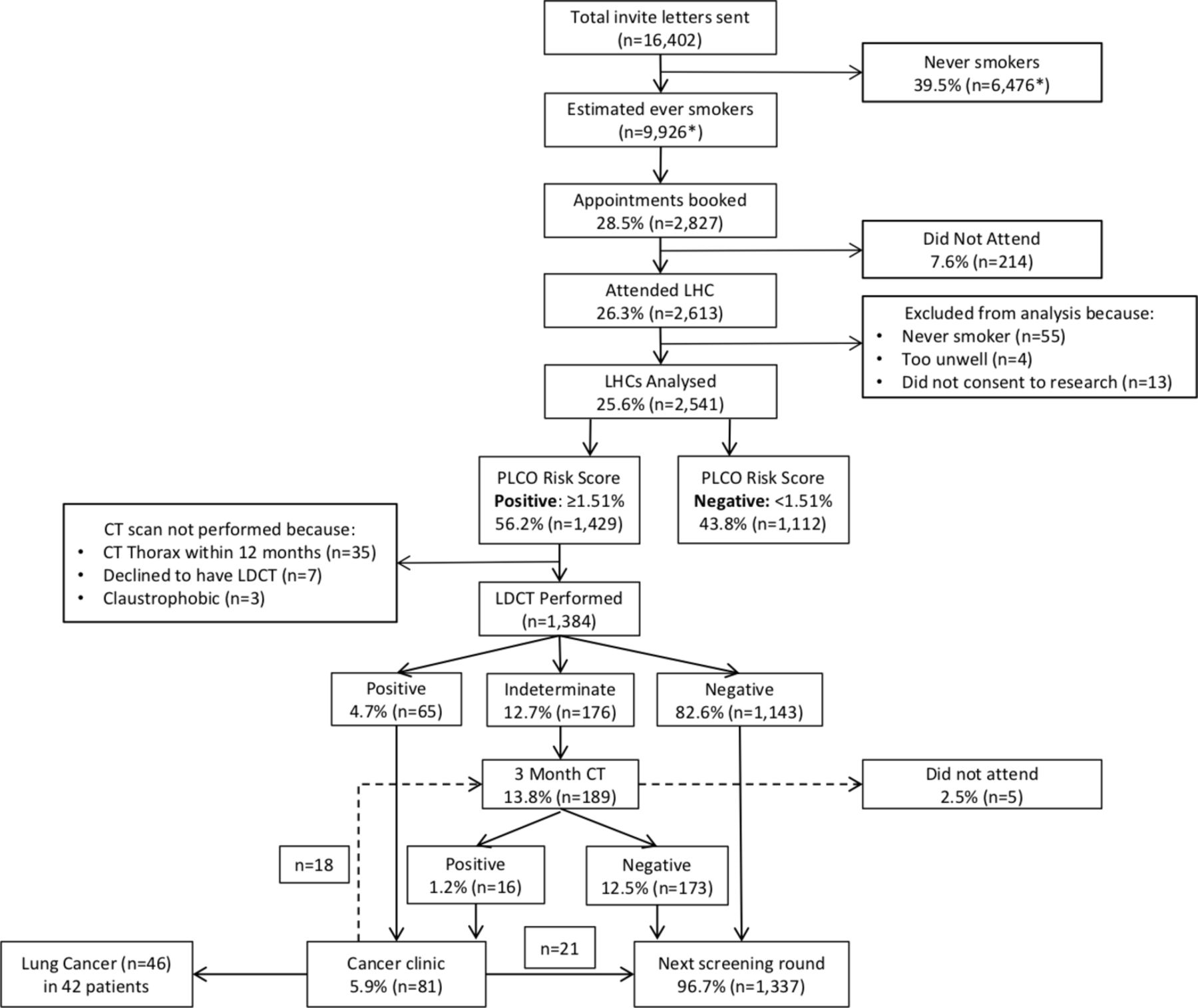
Demand was extremely high, and all LHC appointments were booked within a few days; 99.5% consented to the research database (n=2541). Baseline characteristics are detailed in table 1. Overall, 56.2% (n=1429) of attendees qualified for screening, and 1384 had an LDCT scan (35 excluded because CT thorax <12 months, 7 declined and 3 unable—claustrophobia); 82.6% of baseline scans were classified as negative (n=1143), 12.7% indeterminate (n=176) and 4.7% positive (n=65) (figure 1). Negative scans had no nodules (73.8%; n=844), nodules <6 mm (24.9%; n=284) or larger stable/benign nodules (1.3%; n=15). Three-month scans were performed for either nodule (87.8%; n=166) or non-nodule surveillance (12.2%; n=23). The dominant nodule at baseline was solid (54.2%; n=90), part solid (12%; n=20) or a pure ground-glass opacity (pGGO) (33.7%; n=56).
{kind=link}
Diagram showing flow of participants through the screening service. *Based on general practitioner-recorded smoking status for 15 072 invitees. LDCT, low-dose CT scan; LHC, lung health check.
Characteristics of individuals who attended the LHC, stratified by lung cancer risk
Of 81 (5.9%) individuals assessed in the cancer clinic, 42 were confirmed to have lung cancer. The false positive rate was 48.1% (n=39/81) as a proportion of cancer clinic referrals, or 2.8% of everyone screened. Patients who ultimately did not have cancer had the following investigations: positron-emission tomography (PET)–CT (n=17), bronchoscopy (n=9), endobronchial ultrasound (n=3), staging CT (n=6) and percutaneous biopsy (n=4). No surgical interventions were required for benign disease; one patient had a pneumothorax post-CT-guided biopsy.
The prevalence of lung cancer was 3% (95% CI 2.3% to 4.1%; n=42/1384); 46 lung cancers were detected as three patients had >1 cancer (table 1). Cancers were 63% stage I (n=29/46), 17.4% stage II (n=8/46), 8.7% stage III (n=4/46) and 10.9% stage IV (n=5/46). While we recognise the inherent biases associated with historical controls, this represented a significant stage shift (P<0.0001) compared with lung cancers (n=399) diagnosed across the same geographical area the year before the pilot started (31% stage I+II and 48% stage IV). The characteristics of screen detected cancers are detailed in table 2; pathological types included adenocarcinoma (n=24), squamous cell (n=13), small cell (n=2), adenosquamous (n=2) and carcinoid (n=1). Four cases had a clinical diagnosis without pathological confirmation. The surgical resection rate was 65.2% (n=30/46). There was one death within 90 days of surgery. A curative intent treatment was offered for 89.1% (n=41/46) of cancers.
Clinical details of screen detected lung cancers
Discussion
In this paper, we report baseline results from the UK’s first community-based, LDCT lung cancer screening service, using mobile CT scanners. Our approach was to target high-risk individuals in deprived areas of Manchester, with an invitation to convenient community-based LHC with immediate access to CT. We selected the screened population according to individual risk scores (PLCOM2012). The prevalence of lung cancer was 3%, and most screen detected lung cancers were early stage (80.4%). The surgical resection rate was 65%, fourfold higher than the UK average. Median deprivation rank was within the lowest decile for England (2873), markedly lower than UKLS (17 374)7 and in contrast to screening trials where participation favours more affluent and better educated individuals,2 suggesting our approach engaged individuals of lower SES from deprived areas, a key demographic of the ‘hard-to-reach’.
To minimise overdiagnosis, only persistent pGGOs ≥5 mm were surveyed and subsolid lesions with a solid component ≥8 mm investigated; intervention was generally reserved for lesions with avidity on PET scan above the mediastinal blood pool or a volume doubling time <400 days. All surgically resected adenocarcinomas had ≥10% non-lepidic and invasive histology, suggesting this approach was appropriate. No surgery was performed for benign disease. One death occurred within 90 days of surgery (in a patient with two confirmed lung cancers). This mortality is below the national average, but underlines the importance of appropriate patient selection and minimising unnecessary invasive procedures.
In conclusion, our results have demonstrated that an appropriately designed service, using an LHC approach, can engage participants at high risk of lung cancer from deprived areas. This resulted in high rates of early stage lung cancer detection with minimisation of harms. It was not a clinical trial but an evidence-based pragmatic evaluation of an NHS commissioned and implemented pilot within a regional lung cancer service. Further evaluation of the Manchester LHC model will be undertaken in a roll-out of the service across the whole of North Manchester and at a number of additional sites as recently announced by NHS England.10
Footnotes
Contributors Service concept: RB, PAC, PVB, AT and JT. Service development by members of the Macmillan Cancer Improvement Partnership: JT, ZK, GH, CH, PVB, MA, VB-B, JE, DM, JF, MS, AM, MO’L, RP, JP, LY, AT, PE, DC, ST, RB, PAC, ES, DK, BT and ST. Service operation and delivery by the Manchester University NHS Foundation Trust lung cancer team: HB, ME, TE, JK, SMa, AWat, RD, MG, RS, AS, ES, PVB, PAC and RB. Radiology reporting by the radiology consortium: RD, MG, JH, KI, DK, SMe, TN, RS, NJS, AS, ES, BT, AWal and JW. Analysis of data and drafting of the manuscript: PAC, HB, LY, PVB, ME, JT and RB. Guarantors of overall content: PAC and RB. Review, revision and agreement of final manuscript: all authors.
Funding The pilot was supported by funding from Macmillan Cancer Support. The Macmillan Cancer Improvement Partnership facilitated the design and development of the pilot. The service was delivered by the lung cancer team at Wythenshawe Hospital, Manchester University NHS Foundation Trust, in partnership with Alliance Medical. LDCT reporting was performed by a consortium of NHS consultant radiologists with subspeciality interest in thoracic medicine. The pilot service was commissioned by South Manchester Clinical Commissioning Group on behalf of the three Manchester Clinical Commissioning Groups. Community engagement was delivered by multiple members of the team and was led by MCIP and the Manchester CCGs in conjunction with Manchester City Council, Macmillan Cancer Support and BHA for Equality.
Competing interests None declared.
Ethics approval North West-Greater Manchester West Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves