Primary and metastatic brain tumours in adults: summary of NICE guidance
BMJ 2018; 362 doi: https://doi.org/10.1136/bmj.k2924 (Published 17 July 2018) Cite this as: BMJ 2018;362:k2924
- Alex Bates, guideline lead1,
- Eva Gonzalez-Viana, systematic reviewer1,
- Garth Cruickshank, clinical advisor, professor of neurosurgery, consultant neurosurgeon2,
- Tom Roques, chair of Guideline Committee, consultant clinical oncologist3
- on behalf of the Guideline Committee
- 1National Guideline Alliance, Royal College of Gynaecologists and Obstetricians, London NW1 4RG, UK
- 2University of Birmingham and University Hospitals Birmingham NHS Foundation Trust, Queen Elizabeth Hospital, Birmingham B15 2TH, UK
- 3Norfolk and Norwich University Hospitals NHS Foundation Trust, Norwich NR4 7UY, UK
- Correspondence to: G Cruickshank garth.cruickshank{at}uhb.nhs.uk
What you need to know
Outcomes of a brain tumour vary substantially depending on its grade, location, and other factors, with life expectancy after treatment ranging from weeks (recurrent glioblastoma) to decades (completely excised, low grade glioma)
Effects of the tumour and side effects of treatment can manifest months or years after treatment and can affect behaviour, cognition, and personality
Treat any change in neurocognitive signs and symptoms as a potential tumour recurrence requiring prompt referral for investigation
Ensure people with brain tumours have a named healthcare professional documented in their medical records who has responsibility for coordinating health and social care support
Consider whether a neurological rehabilitation assessment of physical, cognitive, and emotional function might be required for a person with a brain tumour at any time in the course of their disease
Although primary malignant brain tumours represent only 3% of all cancers, they result in the most life-years lost of any cancer.1 Survival with malignant brain tumours has remained poor despite improvements in diagnosis and management (table 1), and it was believed that survival and quality of life could be improved by standardising care across the country with a guideline. Over 60% of people with primary brain tumours present at and are diagnosed by accident and emergency services rather than by general practitioners or in specialist settings.2 Brain metastases are the most common brain tumour to present in primary care, but other forms of brain cancer are seen.
Care requirements for brain tumours by approximate median survival
Although brain tumours are usually managed by specialist teams, primary care and non-specialist teams have an important role in patients’ long term care, particularly when it comes to considering the longer term cognitive, physical, and mental health effects of the tumour and its treatment (table 1).
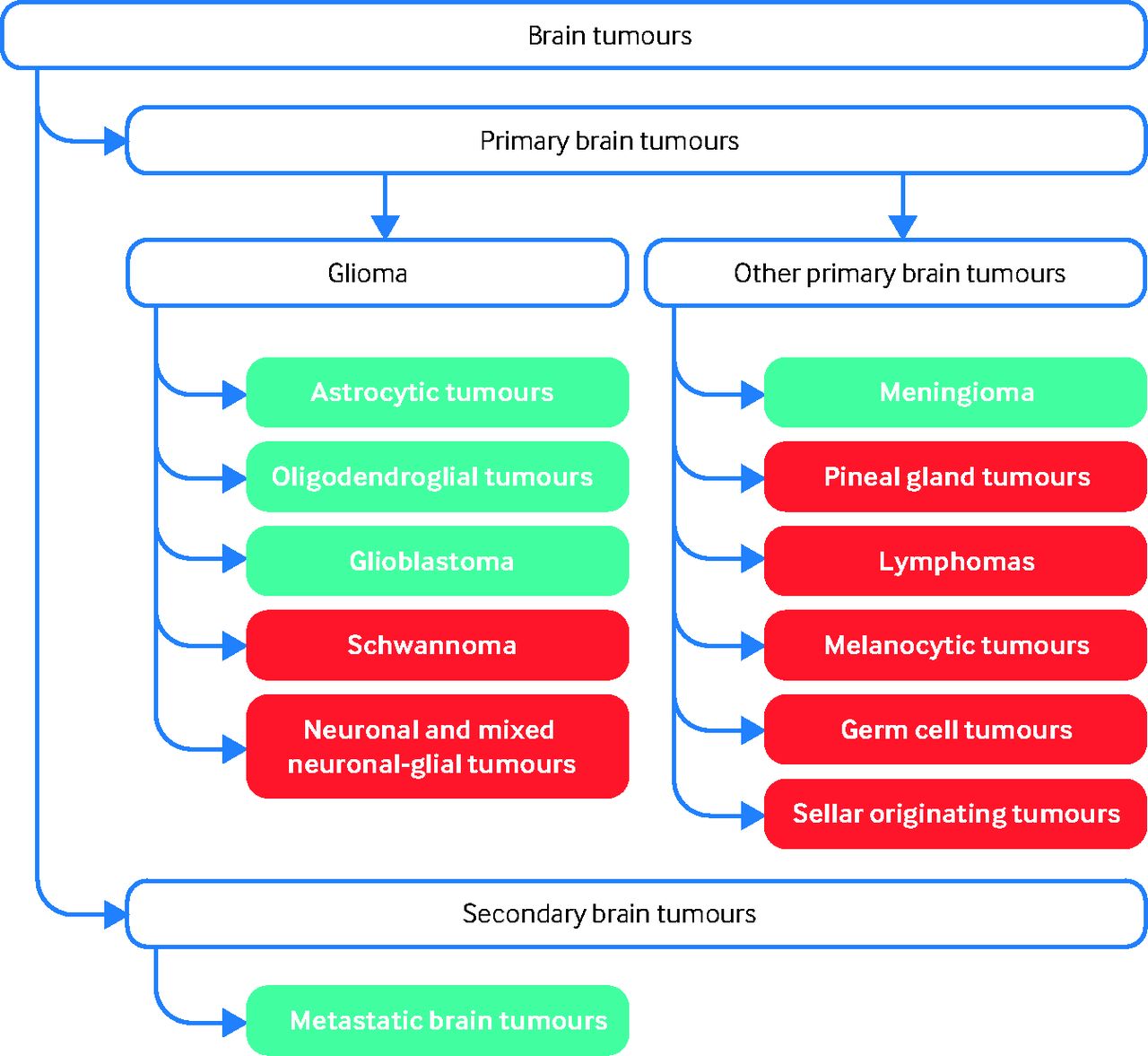
This article summarises the most recent recommendations from the National Institute for Health and Care Excellence (NICE) on the management of glioma, meningioma, and cerebral metastases (fig 1 lists the conditions covered in the guidance).3 It particularly focuses on recommendations about the longer term follow-up of patients and potential complications of treatment that are more relevant for primary care professionals, such as general practitioners.

Brain tumours included in the guideline (blue) and not included in the guideline (red)
{kind=link}
What’s new in this guidance
It is recommended not to offer tumour-treating fields (continuous application of electrical fields to the scalp) as they are not cost effective under conventional criteria
Irradiation of the surgical cavity is recommended after resection of 1-3 brain metastases
5-Aminolevulinic acid (5-ALA) is recommended, in line with a government commitment to a national roll-out of 5-ALA, to help improve resection if the multidisciplinary team thinks that surgical resection of all enhancing glioma is possible—this is likely to have a high cost impact on neurosurgical units
Recommendations
NICE recommendations are based on systematic reviews of best available evidence and explicit consideration of cost effectiveness. When minimal evidence is available, recommendations are based on the Guideline Committee’s experience and opinion of what constitutes good practice.
The four areas of the guideline most relevant to non-specialists are;
Care needs of people with brain tumours
Neurorehabilitation assessment
Late effects of tumours
Routine follow-up schedules.
Care needs of people with brain tumours
Consider complex care needs
Brain tumours are unique in that they affect a person’s sense of selfhood by physically interfering with normal brain function. The guideline emphasises the importance of addressing these areas of complex additional need.
Be aware that the care needs of people with brain tumours represent a unique challenge because, in addition to physical disability, the tumour and treatment can have affect:
Behaviour
Cognition
Personality.
Discuss health and social care support needs with the person with a brain tumour and their relatives and carers (as appropriate). Take into account the complex health and social care support needs that people with any type of brain tumour and their relatives and carers may have (psychological, cognitive, physical, spiritual, emotional).
Set aside enough time to discuss the impact of the brain tumour on the person and their relatives and carers and to elicit and discuss their health and social care support needs.
[Based on medium to high quality qualitative evidence]
Provide a named point of contact
Coordinating these complex needs is challenging, and a key requirement for people with a brain tumour is a contact with whom they can discuss their concerns, and who will usually be allocated by either secondary care centres or the tertiary neurosciences centre. Ensure this contact is clearly visible in all medical records, including primary care, so that the person with a brain tumour and their primary and secondary care teams can coordinate care and support effectively.
Provide a named healthcare professional with responsibility for coordinating health and social care support for people with brain tumours and their relatives and carers—for example, a key worker (often a clinical nurse specialist) as defined in NICE guidance on improving outcomes for people with brain and other central nervous system tumours.4 [Based on high quality qualitative evidence]
Sharing information
People with brain tumours are often dissatisfied with the way information is provided to them.5 The guideline recognises that the way information is delivered and the timing are important, but clarifies that some information is legally required and should not be forgotten. While specialists usually make and explain the diagnosis and treatment, non-specialists are often asked to interpret this further for the patient.
Give information to the person with a brain tumour and their relatives and carers (as appropriate):
In a realistic and empathetic manner
In suitable formats (written and spoken, with information available to take away) following the principles in the NICE guideline on patient experience in adult NHS services6
At appropriate times throughout their care pathway.
Provide and explain clinical results, for example imaging and pathology reports, to the person with a brain tumour and their relatives and carers as soon as possible.
Explain to the person that they have a legal obligation to notify the Driver and Vehicle Licensing Agency (DVLA) if they have a brain tumour, and that this may have implications for their driving.
[Based on medium to high quality qualitative evidence and the opinion of the Guideline Committee (GC)]
Neurorehabilitiation assessment
NICE intend to commission separate guidelines on neurological rehabilitation, and therefore the guideline only made recommendations on an assessment for such rehabilitation. Referrals to neurological rehabilitation are mostly made by secondary and tertiary care specialists, although they can also be done by primary care clinicians and non-specialists.
Consider referring the person with a brain tumour for a neurological rehabilitation assessment of physical, cognitive, and emotional function at diagnosis and at every stage of follow-up.
Offer people with brain tumours and their relatives and carers (as appropriate) information on accessing neurological rehabilitation, and on what needs it can help address.
Give people with brain tumours and their relatives and carers information on:
Neurological rehabilitation options in the community as an outpatient or as an inpatient
How to get a neurological rehabilitation assessment.
[Based on the opinion and experience of the GC]
Late effects of tumours
The treatment of brain tumours can have side effects months or years after treatment. Table 2 gives examples of these late effects, and box 1 lists recommendations made by the Guideline Committee on how to reduce risks.
Examples of early and late side effects of treatment for brain tumours
Examples of how to manage risk of late side effects of radiotherapy
After cranial radiotherapy—Encourage a healthy lifestyle, including exercise, a healthy diet, and stopping smoking (if applicable), to decrease the risk of stroke
At risk of stroke—Check blood pressure, HbA1c level, and cholesterol profile regularly (frequency not specified in guideline due to lack of consensus)
At risk of cognitive decline—Consider ongoing neuropsychology assessment
At risk of visual impairment—Consider referral for ophthalmological assessment
At risk of hearing loss—Consider referral for hearing test
At risk of hypopituitarism after radiotherapy*—Check endocrine function regularly
Asymptomatic ischaemic stroke†—Refer to stroke services
*Common if the pituitary gland receives a significant dose of radiation
†Identified by magnetic resonance imaging during active monitoring
Assess the person's individual risk of developing late effects when they finish treatment. Record these in their written treatment summary and explain them to the person (and their relatives and carers, as appropriate). [Based on the opinion and experience of the GC]
Routine follow-up schedules
The Guideline Committee discussed the many roles of follow-up, including the proactive support of people with brain tumours and early identification of disease recurrence or progression. The potential harms of too many hospital visits and scans were also acknowledged.
There is wide variation across practice in follow-up regimens. Included in the guideline are recommendations for follow-up for glioma, metastases, and meningioma (see boxes 2-4) that will allow for the first time planning of services and in particular estimations of workload for surveillance imaging.
Suggested clinical review schedule for people with glioma by tumour grade
Grade I
Scan at 12 months, then consider:
Discharge if no tumour visible on imaging, unless completely resected pilocytic astrocytoma
Imaging at increasing intervals for 15 years for completely resected pilocytic astrocytoma
If imaging needed every 1-3 years for rest of life if tumour is visible on imaging
Grade II, IDH1 mutation, 1p19q non-codeletion; Grade II, 1p19q codeletion; Grade III, 1p19q codeletion
First 2 years after treatment—Scan at 3 months, then every 6 months
Years 2-4—Scan annually
Years 5-10—Scan every 1-2 years
>10 years—Consider ongoing imaging every 1-2 years
Grade II, IDH1 wild type; Grade III, 1p19q non-codeletion; Grade IV (glioblastoma)
First 2 years after treatment—Scan every 3-6 months
Years 2-4—Scan every 6-12 months
Years 5-10—Scan annually
>10 years—Consider ongoing imaging every 1-2 years
Suggested clinical review schedule for people with meningioma by tumour grade
Grade I, no residual tumour*
First year after treatment—Scan at 3 months
Years 1-3—Scan annually
Years 4-9—Scan every 2 years
>9 years—Consider discharge
Grade I, residual tumour*
First year after treatment—Scan at 3 months
Years 1-5—Scan annually
Years 6-9—Scan every 2 years
>9 years—Consider discharge
Grade I, after radiotherapy
First year after treatment—Scan at 6 months
Years 1-3—Scan annually
Years 4-9—Scan every 2 years
>9 years—Consider discharge
Grade II
First year after treatment—Scan at 3 months, then 3-6 months later
Years 1-5—Scan annually
Years 6-9—Scan every 2 years
>9 years—Consider discharge
Grade III
First 2 years after treatment—Scan every 3-6 months
Years 3-5—Scan every 6-12 months
>6 years—Scan annually
Asymptomatic incidental meningioma
Scan at 12 months. If no change, consider discharge or scan at 5 years
*Presence of residual tumour can be established only after the first scan at 3 months
Suggested clinical review schedule for people with metastases
First year after treatment—Every 3 months
Second years—Every 4-6 months
>2 years—Annually
The Guideline Committee discussed the advantages and disadvantages of more frequent follow-up (except for patients with active symptoms). These are described in table 3 and could form the basis of a conversation with someone worried about their follow-up.
Pros and cons of more frequent follow-up for people with brain metastases
The critical recommendation of importance to the non-specialist clinical population is to treat changes in neurological signs and symptoms as potential signals of recurrent cancer and to contact the original treatment centre or tertiary centre if concerned:
Arrange a clinical review, including appropriate imaging, for people with brain metastases who develop new or changing neurological symptoms or signs at any time. [Based on the opinion and experience of the GC]
Implementation
The committee recognised that the care of people with brain tumours and those surviving requires both health and social programmes and is concerned that continuity between these services is supported.
Future research
The Guideline Committee identified several areas where they were unable to make recommendations because of a lack of high quality evidence, and therefore prioritised five areas for research (box 5). Of these, one is specifically relevant for primary care providers: “Does early detection of recurrence after treatment improve overall survival/outcomes in molecularly stratified glioma?” The committee decided to prioritise glioma research as it is the most common type of primary brain tumour. Research is needed to establish at what point the value of identifying recurrence early is outweighed by the harms of increasing burden to patients and increasing the burden on primary care providers of screening more extensively for changing neurological symptoms and signs. Box 6 provides details of this suggested trial.
Recommendations for further research
Does the addition of concurrent and adjuvant temozolomide to radiotherapy improve overall survival in patients with IDH wild type grade II glioma?
Does a dedicated supportive care clinic in addition to standard care improve outcomes for people with low-grade glioma?
Does early referral to palliative care improve outcomes for people with glioblastomas in comparison with standard oncology care?
Does early detection of recurrence after treatment improve overall survival/outcomes in molecularly stratified glioma?
Is immediate or deferred radiotherapy better for incompletely excised grade I meningioma?
Possible design for primary care trial
Population—Adults (≥18 years old) with newly treated glioma stratified by molecular subtypes
Prognostic or risk factor—Routine imaging (as per guideline recommendations) with intervention when needed
Comparator (without the risk factor)—Imaging on symptoms only with immediate intervention
Outcomes—Overall survival (primary outcome), neurological function, cost effectiveness
Study design—Prospective multicentre study collecting prospective data from community (GP) service, imaging service, and hospital
Timeframe—Will vary by subgroup, but in some groups the timeframe will be ≥10 years
Guidelines into practice
Could I discuss the advantages and disadvantages of more frequent follow-up of people with brain tumours with someone asking for my advice?
Do I have a written copy of the risk of late effects of treatment for every person who has been treated for a brain tumour at my practice?
How would I refer someone with new or changing neurological symptoms for a specialist clinic review?
How patients were involved in the creation of this article
Patients were not directly involved in this article. Committee members involved in this guideline included three patient representatives, who contributed to the formulation of the recommendations summarised here.
Further information on the guidance
Methods
This guidance was developed by the National Guideline Alliance in accordance with NICE guideline development methods (www.nice.org.uk/media/default/about/what-we-do/our-programmes/developing-nice-guidelines-the-manual.pdf).
A guideline committee was established by the National Guideline Alliance, which incorporated healthcare professionals with expertise in managing brain tumours (three neurosurgeons, one neurologist, four oncologists, one neuropsychologist, one diagnostic radiologist, two neuro-oncology clinical nurse specialists, one brain and central nervous system tumour rehabilitation specialist, one neuropathologist) and three lay members.
The committee identified relevant clinical questions, collected and appraised clinical evidence, and evaluated the cost effectiveness of proposed interventions where possible. Qualitative reviews were undertaken to explore aspects related to information and neurological rehabilitation.
Quality ratings of the evidence were based on GRADE methodology (www.gradeworkinggroup.org/). These relate to the quality of the available evidence for assessed outcomes or themes rather than the quality of the study.
The scope and the draft of the guideline went through a rigorous reviewing process, in which stakeholder organisations were invited to comment; the group took all comments into consideration when producing the final version of the guideline.
All versions of the guideline are available from the NICE website (www.nice.org.uk/ng99).
A formal review of the need to update a guideline is usually undertaken by NICE after its publication. NICE will conduct a review to determine whether the evidence base has progressed significantly to alter the guideline recommendations and warrants an update.
Acknowledgments
The members of the guideline committee were Tom Roques, Garth Cruickshank, Alison Cameron, Catherine Derbyshire, Colin Watts, David Summers, Eileen Andrews, Helen Bulbeck, Ingela Oberg, Isabella Robbins, Jeremy Rees, Sara Erridge, Sara Robson, Sarah Jefferies, Sebastian Brandner, Stuart Smith, and Zoe Faulkner.
The members of the National Guideline Alliance technical team were Alex Bates, Eva Gonzalez-Viana (from September 2016), Huayi Huang (from September 2017 to January 2018), James Hawkins, John Graham, Katherine Andrea (from October 2017), Katrina Blears (until September 2016), Kelly Williams (from November 2016 until March 2017), Leanne Saxon (from September 2016 until April 2017), Mia Schmidt-Hansen (from February 2017), Natasha Pillai (until November 2016), Sabrina Naqvi (from September 2016 until November 2016), Stephanie Arnold, Victoria Rowlands (from November 2016 until October 2017), with additional support from Angela Bennett, Annabel Flint, Jennifer Francis, Matthew Prettyjohns, Méleshah Brown and Sally Humphreys.
Footnotes
Contributors: All authors contributed to the initial draft of this article, helped revise the manuscript, and approved the final version for publication.
The views expressed in this article are those of the authors and not necessarily those of NICE.
Funding: AB and EG are employees of the National Guideline Alliance, which is commissioned and funded by NICE to develop clinical guidelines and write this BMJ summary. No authors received special funding from any other source to write this summary.
Competing interests: We declare the following interests based on NICE's policy on conflicts of interests (available at www.nice.org.uk/Media/Default/About/Who-we-are/Policies-and-procedures/code-of-practice-for-declaring-and-managing-conflicts-of-interest.pdf): TR is local principle investigator for several trials funded by CRUK, and local principal investigator of the PLATFORM trial on oesophago-gastric cancer, funded by MedImmune. GC is local investigator on DCVax trial on glioblastoma, funded by North west Biotherapeutics and IDEB trial on glioblastoma, funded by BTG International. GC has also given evidence on brain tumour research in parliament. The authors’ full statements can be viewed at www.nice.org.uk/guidance/ng99/documents/committee-member-list-2.