Acute gastroenteritis in children
BMJ 2007; 334 doi: https://doi.org/10.1136/bmj.39036.406169.80 (Published 04 January 2007) Cite this as: BMJ 2007;334:35
- Elizabeth Jane Elliott, professor in paediatrics and child health
- Correspondence to: E Elliott, c/o Children's Hospital at Westmead, Westmead 2145, NSW, Australia elizabe2{at}chw.edu.au
- Accepted 9 November 2006
Acute gastroenteritis accounts for millions of deaths each year in young children, mostly in developing communities. In developed countries it is a common reason for presentation to general practice or emergency departments and for admission to hospital. Dehydration, which may be associated with electrolyte disturbance and metabolic acidosis, is the most frequent and dangerous complication. Optimal management with oral or intravenous fluids minimises the risk of dehydration and its adverse outcomes. Routine use of antibiotics, antidiarrhoeal agents, and antiemetics is not recommended and may cause harm. Prevention is the key to controlling gastroenteritis, and recently licensed, highly effective rotavirus vaccines will have a major effect on public health.
Sources and selection criteria
I searched the Cochrane Library database using the keywords “acute gastroenteritis” (all text), “acute disease”, “gastroenteritis”, and “child”. I searched Medline via PubMed clinical queries using the keywords “gastroenteritis” together with “oral rehydration”, “antidiarrheal”, “antiemetic”, “probiotic”, and “zinc” with the options “find systematic reviews” and “search by study category—therapy.” The options of “aetiology” and “diagnosis” were also applied using the term “gastroenteritis”. I also searched the child health section of Clinical Evidence and reviewed the reference lists of publications found during searches for other relevant manuscripts
What is the epidemiology and impact of gastroenteritis?
Acute gastroenteritis—diarrhoea or vomiting (or both) of more than seven days duration—may be accompanied by fever, abdominal pain, and anorexia. Diarrhoea is the passage of excessively liquid or frequent stools with increased water content. Patterns of stooling vary widely in young children, and diarrhoea represents a change from the norm.1 Worldwide, 3-5 billion cases of acute gastroenteritis and nearly 2 million deaths occur each year in children under 5 years.2 In the United States, gastroenteritis accounts for about ∼10% (220 000) of admissions to hospital, more than 1.5 million outpatient visits, and around 300 deaths in children under 5 annually, with a cost of around $1bn (£0.5bn; €0.8bn).2 In the same age group in Australia, about 10 000 hospital admissions, 22 000 visits to emergency departments, and 115 000 general practice consultations occur annually for rotavirus alone, with an estimated cost of $A30m (£12m; €18m; $23m).3 In the United Kingdom, 204 of 1000 consultations with general practitioners in children under 5 are for gastroenteritis, and the annual hospital admission rate in this group is about seven per 1000 children.4 Children in childcare settings are often infected but asymptomatic and may unwittingly transmit infection.
Children with poor nutrition are at increased risk of complications. In the north end of Australia, Aboriginal and Torres Strait Islander children have increased rates of admission for gastroenteritis, malnutrition, comorbidity, and electrolyte disturbance (especially hypokalaemia) and a longer hospital stay than their non-indigenous counterparts.5 The cost of gastroenteritis to the community is huge but often underestimated if costs to the family, including lost time at work, are not considered.
Summary points
-
Rotavirus is the most common cause of acute gastroenteritis worldwide and vaccination will have a major impact on disease rates, morbidity, and mortality
-
Most children are not dehydrated and can be managed at home
-
Dehydration, metabolic acidosis, and electrolyte disturbance can be prevented and treated by fluid therapy
-
Most children with mild-moderate dehydration can be treated with oral or enteral rehydration using low osmolality oral rehydration solutions
-
Severely dehydrated or shocked children usually need intravenous fluids and hospital admission
-
Drugs are usually unnecessary and may do harm
-
General practitioners have an important role in prevention, through encouraging breastfeeding, recommending and advocating free access to rotavirus vaccination, and educating carers about personal and food hygiene
What are the causes and clinical characteristics?
Box 1 lists some causes of acute gastroenteritis in children. Worldwide, most cases are due to viral infection (fig 1⇓; box 2), with rotaviruses and noroviruses being most common. Viral infections damage small bowel enterocytes and cause low grade fever and watery diarrhoea without blood. Rotavirus infection is seasonal in temperate climates, peaking in late winter, but occurs throughout the year in the tropics. Rotavirus strains vary by season and geographically within countries.6 The peak age for infection is between 6 months and 2 years, and the mode of spread is by the faecal-oral or respiratory route.
Box 1 Causes of acute gastroenteritis in children
Viruses (∼70%)
-
Rotaviruses
-
Noroviruses (Norwalk-like viruses)
-
Enteric adenoviruses
-
Caliciviruses
-
Astroviruses
-
Enteroviruses
Protozoa (<10%)
-
Cryptosporidium
-
Giardia lamblia
-
Entamoeba histolytica
Bacteria (10-20%)
-
Campylobacter jejuni
-
Non-typhoid Salmonella spp
-
Enteropathogenic Escherichia coli
-
Shigella spp
-
Yersinia enterocolitica
-
Shiga toxin producing E coli
-
Salmonella typhi and S paratyphi
-
Vibrio cholerae
Helminths
-
Strongyloides stercoralis

Fig 1 Rotavirus particles seen under the electron microscope. Courtesy of Alan Philips
{kind=link}
Box 2 Fictitious clinical case
Presentation
Tina is a 6 month old bottle fed infant, brought to your general practice surgery with a 12 hour history of diarrhoea (10 watery green stools without blood) and vomiting (eight yellow non-bilious vomits). Her mother is worried because she is irritable with fever (38°C). Her brother, who attends nursery, has just got over a bout of “gastro.” She is an active baby with perianal excoriation and a weight of 5.5 kg. She has a sunken fontanelle and decreased skin turgor (pinch test 3 sec). She passes urine during the examination. On review of her health record you note she has lost 0.5 kg since last weighed two weeks ago. You diagnose viral gastroenteritis and refer the child to the local paediatric unit.
Diagnosis
Rotavirus infection is confirmed by commercial enzyme linked immunosorbent assay and she is assessed as having moderate (8%) dehydration (on the basis of recent weight loss, decreased skin turgor, raised serum urea, and mild metabolic acidosis).
Management
The child is reluctant to drink so you give an oral rehydration solution by nasogastric tube to rehydrate her over six hours in the emergency department. She is observed overnight to ensure that she is drinking an adequate amount and passing urine.
Bacterial pathogens such as Campylobacter jejuni and Salmonella spp invade the lining of the small and large intestine and trigger inflammation.7 Children with bacterial gastroenteritis are more likely to have high fever and may have blood and white blood cells in the stool. Bacterial pathogens occasionally spread systemically, especially in young children. Infection with Shiga toxin producing Escherichia coli or Shigella dysenteriae may cause haemorrhagic colitis (with severe bloody diarrhoea), which may be complicated by haemolytic uraemic syndrome. This syndrome is endemic worldwide and characterised by acute onset of microangiopathic haemolytic anaemia (fig 2⇓), thrombocytopenia, acute renal impairment, and multisystem involvement (see appendix on bmj.com).8
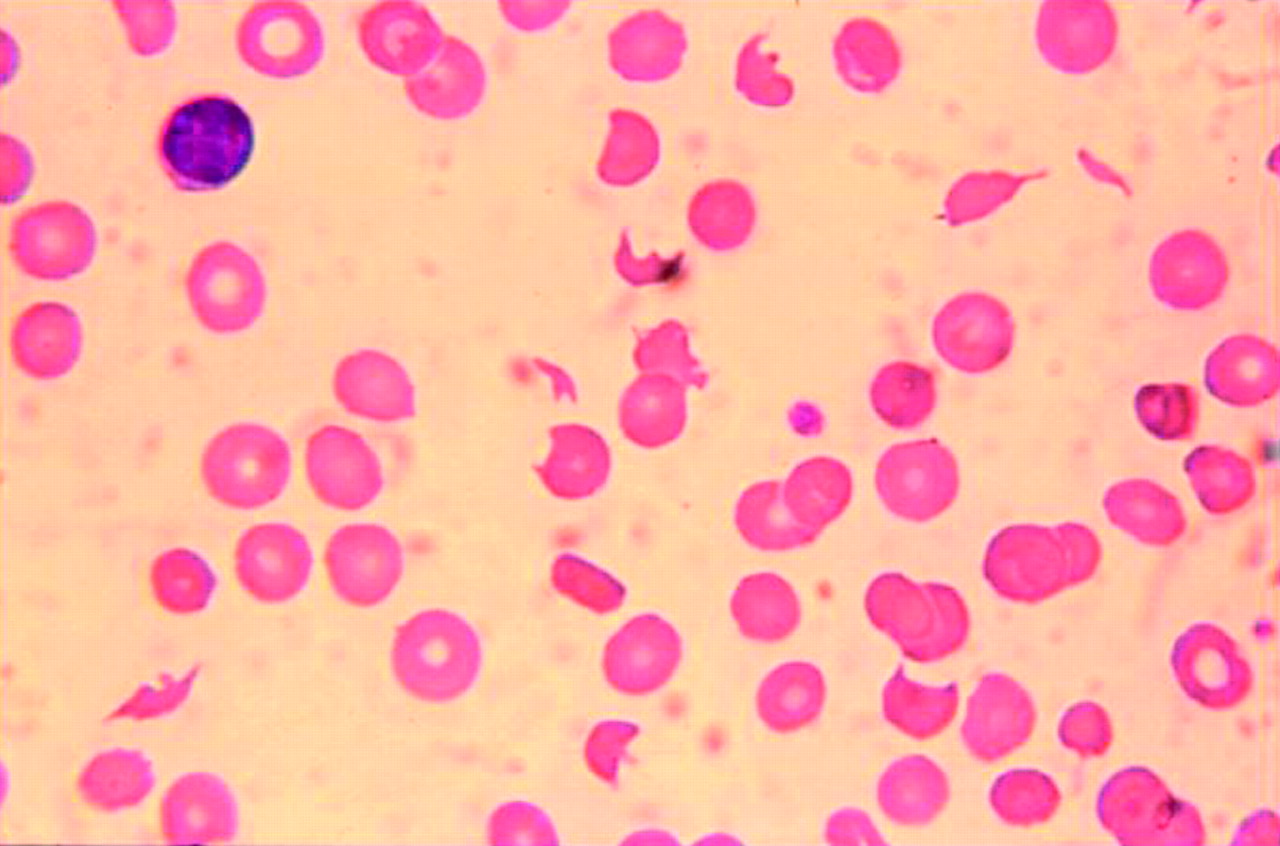
Fig 2 Typical peripheral blood film in a patient with haemolytic uraemic syndrome, microangiopathic haemolytic anaemia, and thrombocytopenia. It shows irregular, fragmented, and helmet shaped red blood cells (schistocytes) and an immature platelet
{kind=link}
The enteric fevers (due to Salmonella typhi and S paratyphi) cause severe illness in young children, characterised by high swinging fever, diarrhoea or constipation, leucopenia, and sometimes central nervous system involvement, including encephalopathy.7 Encephalopathy is a rare complication of non-typhoid Salmonella infection. Vibrio cholera toxin causes chloride and water secretion from the small bowel but does not damage the intestinal mucosa; it results in “rice water” stools that have a high sodium content but do not contain blood or white blood cells.7
Gastroenteritis is acquired by person to person spread or ingestion of contaminated food and drink (“food poisoning”).7 Undercooked, or inappropriately stored cooked or processed meats (chicken, beef, pork) and seafood are common sources of bacterial pathogens. Ingestion of food containing toxins produced by bacterial contaminants (for example, Staphylococcus aureus in ice cream or Bacillus cerus in reheated rice) causes rapid onset of vomiting or diarrhoea (or both). Water may be contaminated with bacteria, viruses, or protozoa including Giardia lamblia, cryptosporidium, V cholera, and Entamoeba histolytica, which causes amoebic dysentery. With increasing rates of overseas travel and immigration, clinicians in developed countries increasingly see children with “traveller's diarrhoea” caused by a range of organisms not normally seen in that environment.
Unanswered research questions in acute gastroenteritis
-
How safe and effective is home based care for children with mild-moderate dehydration?
-
What role do food based oral rehydration solutions have in developed communities?
-
What is the role and safety of new generation antiemetics and antidiarrhoeal agents?
-
What is the role of zinc supplementation in well nourished children?
-
Do probiotics have a role as adjuvant therapy, and what type, dose, and regimen is optimal?
How is it diagnosed?
Diagnosis can be made clinically. Information should be sought about recent contact with people with gastroenteritis, nature and frequency of stool and vomitus, fluid intake and urine output, travel, and use of antibiotics and other drugs that may cause diarrhoea. Chronic constipation is common in children, and faecal overflow incontinence may present as spurious diarrhoea. Diarrhoea and vomiting are non-specific symptoms in young children, and the diagnosis of gastroenteritis should be questioned in children with high fever, prolonged symptoms, or signs suggesting a surgical cause (such as severe abdominal pain, bilious vomiting, abdominal mass). Children with diabetes mellitus and inborn errors of metabolism may present with vomiting. Children with underlying diseases may be at increased risk of complications and referral to a paediatric service should be considered.
It is not necessary or practical to take stool specimens from all children with gastroenteritis. Samples should be taken during outbreaks—especially in childcare, school, hospital, or residential settings—where there is a public health imperative to identify the pathogen and establish its source. Samples should be cultured for bacteria and tested for viral pathogens. Testing for rotavirus, norovirus, and sometimes other viruses is available in most children's hospitals using methods for rapid antigen detection (such as enzyme linked immunosorbent assay). Rapid diagnosis allows for isolation of the child to prevent nosocomial infection, which is common and is often used as a marker of the effectiveness of precautions to control contact infection. Stool samples should also be taken from children with bloody diarrhoea, a history of recent foreign travel, and from young or immunocompromised children with high fever. In many countries legislation requires clinicians to notify public health authorities about a range of viral and bacterial infections.
How is dehydration assessed?
It is important to assess hydration in gastroenteritis as hydration status determines the immediate management of this condition. The infant or child with profuse watery diarrhoea and frequent vomiting is most at risk. Clinicians often overestimate the extent of dehydration. Clinical signs are usually not present until a child has lost at least 5% of his or her body weight. Documented recent weight lost is a good indicator of the degree of dehydration, but this information is rarely available. The best clinical indicators of more than 5% dehydration are prolonged capillary refill, abnormal skin turgor, and absent tears.9 The recommendations for assessing and managing dehydration shown in table 1⇓ are adapted from the World Health Organization classification and are supported by the literature.9 10 11 Serum electrolytes are not routinely required but should be measured before and after starting intravenous fluids.
Assessment and management of dehydration
How is gastroenteritis treated?
Table 1⇑ summarises the management of dehydration2 4 10 11 12 13 14 15 16 17 18 19 20 21 22 23 and table 2⇓ lists the type of evidence supporting management decisions in gastroenteritis (a longer version of table 2 (table A) is available on bmj.com). Management aims to prevent and treat dehydration, maintain nutrition, and minimise harm.
Evidence based management of gastroenteritis
Which fluid therapy?
Children with no dehydration or mild dehydration can usually be managed at home, although children with high risk for complications or who cannot be adequately cared for at home should be considered for admission.2 11 13 Children with mild-moderate dehydration who do not tolerate oral fluids should be admitted for observation. Oral rehydration solutions are preferable to other clear fluids for preventing and treating dehydration.2 4 11 Fluids high in sugar (such as cola, apple juice, and sports drinks, which contain ≤20 mmol/l sodium and have a high osmolality of 350-750 mOsm/l) may exacerbate diarrhoea and should be avoided.11 Breast feeding should be continued during acute gastroenteritis and supplemented with an oral rehydration solution if needed.11 12
Although most children with dehydration drink readily, some refuse rehydration solutions because they dislike the taste, feel nauseated, or have profuse vomiting. Older children may be afraid of vomiting and parents may perceive fluids are the cause of vomiting. If small sips cannot be tolerated, use of a syringe can help in infants. If oral intake is inadequate, a fine bore nasogastric tube is usually well tolerated.14 15 Alternatively, fluids may be given intravenously.11 Enteral (oral or nasogastric) and intravenous fluids are equally safe and effective for mild-moderate dehydration,14 15 and rehydration can usually be achieved in four to six hours.
In developed communities children with severe dehydration are routinely admitted for intravenous therapy,2 11 although enteral rehydration has been used safely in severe dehydration with fewer adverse effects than intravenous therapy (table 2⇑).14 15 Children with shock require intravenous resuscitation before rehydration.2 10 11
The most common adverse effect of intravenous cannulation is infiltration at the cannula site, but infection, pain, bleeding, and physical and emotional trauma may also occur. Intravenous therapy is more expensive than oral rehydration therapy and requires hospital admission. Iatrogenic complications—especially electrolyte disturbance due to inappropriate composition, rate of administration, or volume of intravenous fluids—may lead to complications, including hyponatraemia with brain injury or death (box 3). If rapid intravenous rehydration is used, careful supervision is needed to avoid fluid overload (dehydration is often overestimated) and electrolyte imbalance.
Box 3 Complications of acute gastroenteritis
-
Dehydration
-
Metabolic acidosis
-
Electrolyte disturbance (hypernatraemia, hyponatraemia, hypokalaemia)
-
Carbohydrate (lactose, glucose) intolerance
-
Susceptibility to reinfection
-
Development of food (cow's milk, soy protein) intolerance
-
Haemolytic uraemic syndrome
-
Iatrogenic complications (due to inappropriate composition or amount of intravenous fluids)
-
Death
Which oral rehydration solution?
Solutions with low osmolality (200-250 mOsm/l) and sodium (60-70 mmol/l) that contain glucose, potassium, and a base (such as citrate) are recommended for developed and developing communities (table 2⇑; table B on bmj.com).16 17 18 Although cereal based oral dehydration solutions are beneficial in cholera-like diarrhoea,19 evidence of benefit in non-cholera diarrhoea is scant and further trials are needed to evaluate efficacy and cost effectiveness.
What about diet?
In a systematic review, probiotics—used as an adjunct to oral rehydration therapy—decreased the duration of diarrhoea, especially in rotavirus gastroenteritis (table 2⇑).20 Further research is needed to determine the optimal type, dosage, and regimen of probiotics before they are recommended for routine use.
Additional educational resources
Clinical resources
-
Clinical evidence (www.clinicalevidence.com/ceweb/conditions/chd/chd.jsp)
-
Cochrane Library (www.cochrane.org)
-
Evidence-based Paediatrics and Child Health (www.evidencebasedpediatrics.com)
-
Managing acute gastroenteritis among children (www.cdc.gov/mmwr/preview/mmwrhtml/rr5216al.htm)
-
Glass RI, Parashar UD. The promise of new rotavirus vaccines. N Engl J Med 2006;354:75-7
Information resources for patients
-
BUPA. Gastroenteritis in children (http://hcd2.bupa.co.uk/fact_sheets/html/gastroenteritis_children.html)
-
Cincinnati Children's Hospital Medical Centre, USA. Gastroenteritis (www.cincinnatichildrens.org/health/info/abdomen/diagnose/gastroenteritis.htm)
-
Health Institute. An Australian government initiative. Gastroenteritis in children (www.healthinsite.gov.au/topics/Gastroenteritis_in_Children)
Children should resume their normal diet once their appetite returns.2 10 11 Published guidelines recommend early reintroduction of milk and solids including complex carbohydrates, lean meats, yogurt, and vegetables, but foods high in fat and sugars should be avoided.3 Early refeeding reduces the duration of diarrhoea. In formula fed infants feeds do not need to be diluted when reintroduced.21
What is the role of drugs?
Drugs are rarely needed.3 10 11 They deal with the symptoms rather than causes of disease and may distract from the use of appropriate fluid therapy. Antibiotics are not indicated in viral or uncomplicated bacterial gastroenteritis and may cause harm. For example, in non-typhoid Salmonella infections antibiotics increase the risk of prolonged carriage and disease relapse. Treating gastroenteritis due to Shiga toxin producing E coli with antibiotics may increase the risk of haemolytic uraemic syndrome. Antibiotics are required, however, for bacterial gastroenteritis complicated by septicaemia and in cholera, shigellosis, amoebiasis, giardiasis, and enteric fever.
Antidiarrhoeal and antiemetic agents are not recommended for routine use because of the risk of adverse effects (table 2⇑; table A on bmj.com).3 10 11 Although new generation antiemetics (such as the serotonin antagonist ondansetron) do not have extrapyramidal effects and reduce the duration and frequency of vomiting, they also increase diarrhoea. Antimotility agents (such as loperamide) decrease the duration of diarrhoea, but they have potential severe adverse effects and evidence that benefits outweigh potential harms is lacking.6
In developing countries, oral zinc given at the onset of symptoms decreases the duration and severity of acute diarrhoea and is recommended by the WHO.10 Vitamin A does not influence the course of acute gastroenteritis.
Is a lactose-free diet necessary?
Carbohydrate (particularly lactose) intolerance is a common complication of viral gastroenteritis as a result of damage to and loss of mature enterocytes containing lactase. Lactose intolerance is usually mild and self limiting and does not require treatment.3 21 If lactose intolerance persists, a lactose-free formula is recommended for four to six weeks.3 21 The damaged gut is more permeable to foreign antigens and intolerance to food proteins (β lactoglobulin in cow's milk and other proteins) is occasionally seen after gastroenteritis; it can be managed by a period of dietary exclusion.3 10 11
Can gastroenteritis be prevented?
Although rotavirus may be spread in aerosols, gastroenteritis is usually spread by the faecal-oral route. Bacterial gastroenteritis can occur in young children served uncooked fermented meats, undercooked hamburgers, unwashed fruits and salads, and water contaminated by animal faeces. Gastroenteritis may also be acquired from environmental sources, such as children's animal farms, swimming pools, and beaches. Good hygiene is important to prevent spread of infection. This includes careful hand washing, nappy disposal, and preparation and storage of food and drinking water, as outlined in the WHO's five step guide to safe food (table C on bmj.com). Hygiene is particularly important in institutions, including hospitals where nosocomial infection is common.
Tips for non-specialists
Differential diagnoses
-
Other infections, such as urinary tract infection, otitis media, pneumonia, septicaemia
-
Surgical causes, such as intussusception, appendicitis, small intestinal obstruction (including malrotation)
-
Taking antibiotics or other drugs
-
Spurious diarrhoea; for example, in chronic constipation with overflow incontinence
-
Non-infectious diseases such as diabetic ketoacidosis, inborn errors of metabolism
-
Occasionally acute infectious gastroenteritis unmasks gastrointestinal disease (such as coeliac disease, chronic inflammatory bowel disease), so if diarrhoea persists beyond two weeks take a family and medical history and do appropriate investigations
When to refer to paediatric service
-
If diagnosis in doubt
-
Gastroenteritis in a young infant (<6 months)
-
High risk of dehydration—worsening diarrhoea and vomiting with significant fluid loss
-
Severe dehydration or shock
-
Severe abdominal pain, localised tenderness, or mass
-
Evidence of anaemia, thrombocytopenia, poor urine output, or hypertension (think haemolytic uraemic syndrome)
-
Increased risk of complications—underlying disease (such as diabetes), malnutrition, renal failure, high fever
-
Parent or carer unable to manage the child at home
-
Persistent diarrhoea beyond two weeks may indicate complications such as reinfection, lactose intolerance, or underlying bowel disease
A major recent advance in prevention has been the development and licensing of two oral rotavirus vaccines, whose safety and efficacy have been confirmed in recent large scale trials, each involving more than 60 000 children.24 25 Rotateq (Merck) is a three dose live human-bovine pentavalent reassortant vaccine. Rotarix (GSK) is two dose attenuated human (strain G1P) monovalent vaccine. Both vaccines are highly immunogenic. They provide cross protection against common serotypes and decrease rates of severe gastroenteritis, the need for intravenous fluids, and hospital admission. Importantly, neither is associated with appreciable adverse effects or increased risk of intussusception, which was seen with the first licensed vaccine, RotaShield. Free access to rotavirus vaccine in all communities is imperative and will have an enormous impact on childhood morbidity and mortality.
Footnotes
-
Tables A-C and an appendix are on bmj.com
-
I am grateful to Michael Fasher and Alison Kesson for useful feedback on this article before submission.
-
Competing interests: None declared.