


Urinary tract infection (UTI) is a common bacterial infection of children, with a study published only 2 months ago showing the prevalence of UTI to be around 6% in preschool children presenting unwell to primary care.1
Accurate and timely diagnosis is important in children because appropriate treatment may alleviate suffering and help prevent long-term sequelae such as renal scarring, poor renal growth, recurrent pyelonephritis, impaired glomerular function, hypertension, end stage renal disease, and pre-eclampsia. There is evidence from NICE2 and our group3 regarding the children in whom UTI should be suspected, but much of the evidence was generated in secondary care. However, primary care generated evidence for the symptoms and signs of UTI in preschool children should be available by the end of 2013 from the Diagnosis of Urinary Tract infection in Young children (DUTY) study (see www.dutystudy.org.uk/).
In terms of management, NICE recommends all children aged over 3 months with suspected cystitis/lower UTI receive 3 days of trimethoprim, nitrofurantoin, a cephalosporin, or amoxicillin (younger children, and any child with suspected pyelonephritis, should be immediately referred to secondary care).2 But which antibiotic should primary care clinicians use first? NICE says there is no evidence for differences in effectiveness and that the choice should be based on local guidance and bacterial resistance patterns.
Step up Duffy et al4 who, in this month’s BJGP, have published an article showing that bacterial resistance to trimethoprim in children’s UTI is:
of similar order of magnitude to that seen in adults5 (it was 20% even in children never prescribed trimethoprim);
on the increase;
temporally most strongly associated when trimethoprim has been prescribed recently;
can last at least 3 months; and
is associated with recurrent UTI.
As far as we are aware, this is the first study to show that the previously described time dependent nature of primary care prescribed antibiotics and bacterial resistance in adult UTI6 also holds true for children. And the authors appropriately used a multilevel modelling technique to account for clustering within the data at the levels of the bacteria, the patient, and the patient’s residence. The authors are correct in taking this approach because these levels at least should be considered when understanding the mechanisms by which patients acquire bacteria resistant to antibiotics.
The bacteria, which are in constant competition to predominate, can inherit resistance (‘vertically’) between generations or transmit it within generations (‘horizontally’) via genetic material known as plasmids (explaining how antibiotic naïve bacteria can become resistant). Antibiotics consumed by people, like immunisations, can have ‘direct’ (to the recipient) and ‘indirect’ (to infectious contacts) effects.7 So, pressure on an individual’s susceptible bacteria allows their resistant bacteria to predominate (direct effect). Since the bacteria causing UTI usually start life as bowel flora, this mechanism can directly increase likelihood of a child’s UTI organism being resistant.8 An individual predominantly colonised by a resistant organism is more likely to transmit a resistant rather than susceptible bacterium to an infectious contact (indirect effect). Finally an antibiotic treated individual, in whom their susceptible commensal flora has been eradicated, is more likely to acquire a new (resistant) bacterium (direct and indirect effects).
Questions the Duffy et al paper do not address include:
the effects of non-trimethoprim antibiotics on bacterial resistance to trimethoprim (for example, via plasmids);
absolute bacterial resistance rates to other antibiotics (would nitrofurantoin be any better?);
the effects of total trimethoprim exposure (previously shown to be important)9 — their study investigated only the date of the most recent prescription; and
the effects of consumed versus prescribed antibiotics.
Concerns regarding the overuse of antibiotics for minor self-limiting illness, and the long-term consequences of bacterial resistance to antibiotics have never been greater. The 2012 European Antibiotic Awareness Day (annually in November) was showcased by the Chief Medical Officer for England and the December issue of the BJGP10 drew attention to the RCGP’s parent, patient, and GP Antibiotic Toolkit, known as ‘TARGET’ (see http://www.rcgp.org.uk/targetantibiotics/). This will provide primary care clinicians and their patients with all the information and evidence needed to address the ‘why’ and ‘how’ of antibiotic overuse.11
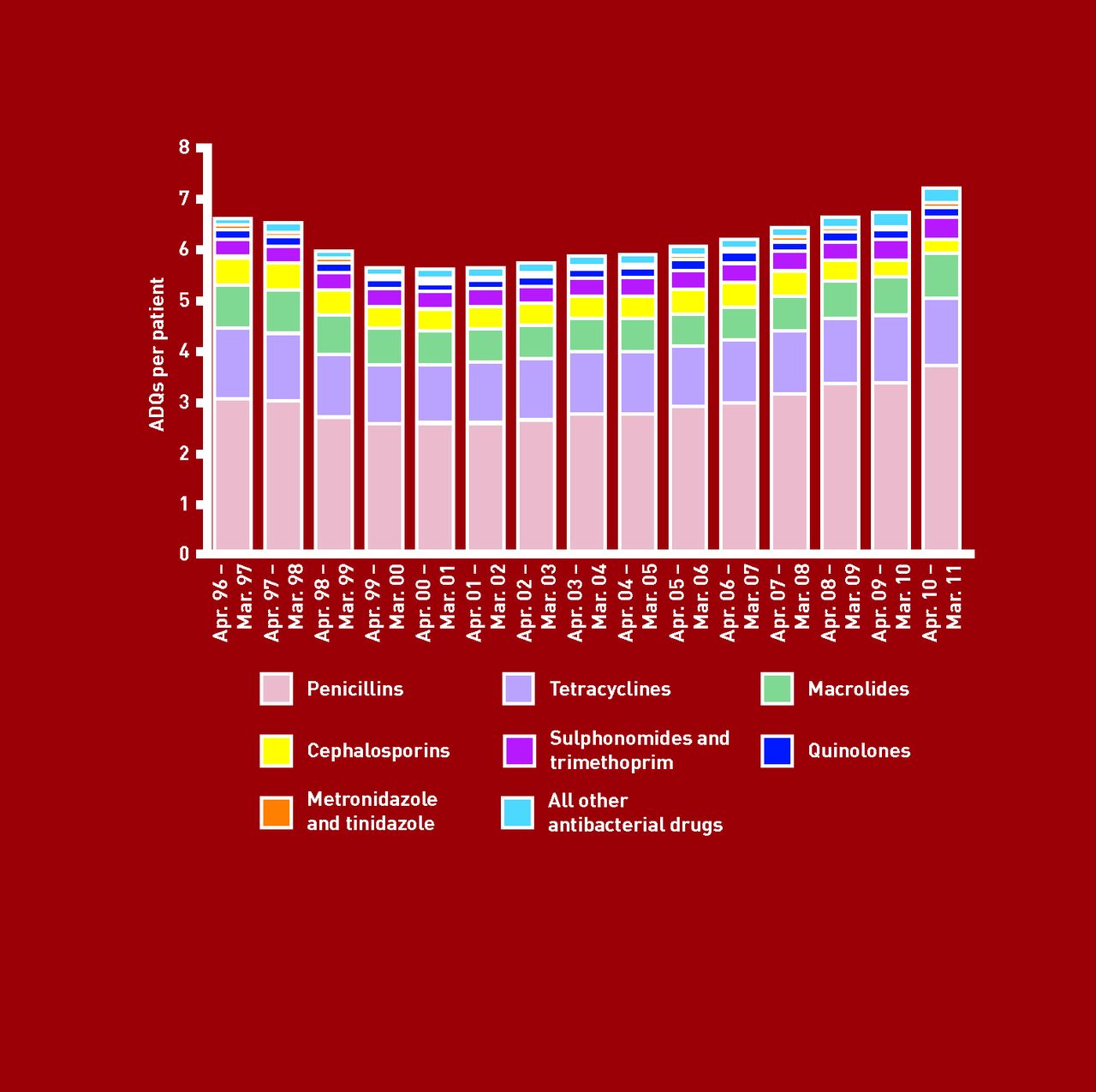
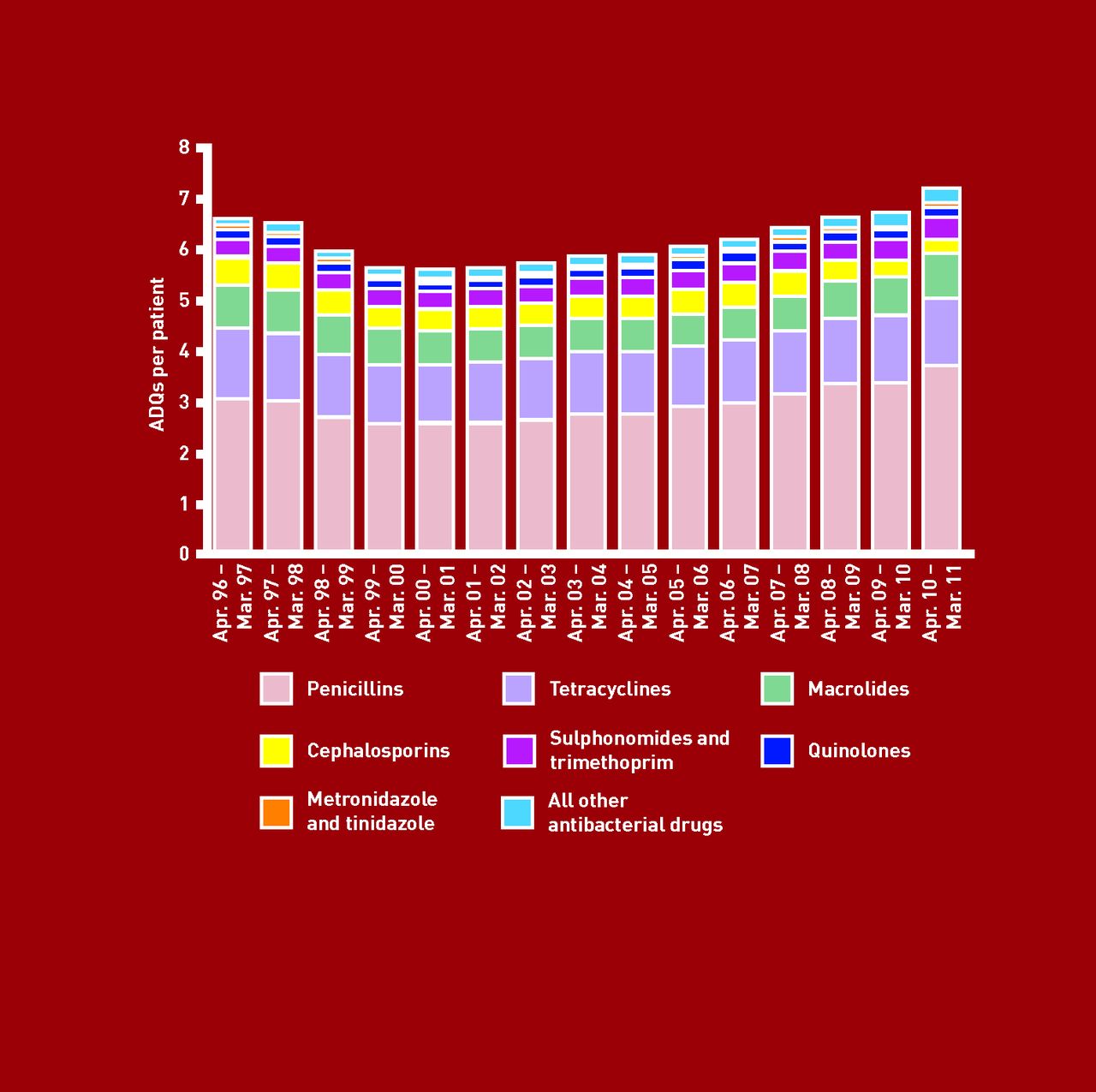
So, why are primary care antibiotic prescribing rates on the increase (Figure 1)?12 In short, we don’t know. We don’t know the relative contributions of the increasing demand for primary care,13 changes in the spectrum of illness severity, professional uncertainty, major political and organisation upheaval, or patient expectations. But each time we prescribe an antibiotic, we do a combination of both good and harm, with the balance probably tipped towards harm for many of our patients. They are ineffective for most patient groups with most infections, they cause side effects and we create the rod for our own backs of increased morbidity,14 costs, and consultations15 for patients with antibiotic resistant bacterial infections.
{kind=link}
Trends in antibiotic prescribing in English general practice April 1996 to March 2011.12
But children with UTI should be treated with antibiotics. So, what are the implications of the Duffy et al paper? As the authors state, the main clinical implication of this paper is to consider an alternative antibiotic to trimethoprim. For children aged over 3 months with suspected cystitis and/or lower UTI and without known antibiotic allergies, this means prioritising nitrofurantoin over amoxicillin or a cephalosporin as the least broad spectrum antibiotic with the lowest resistance rates.5 And, these data should make us reconsider the strength of evidence for all antibiotic use (excluding childhood UTI) since the use of antibiotics have considerable direct and indirect effects on our patients and their wider communities.
More research is urgently needed to help us understand the causes of, and reverse, the current trend for increased antibiotic prescribing. Such research will need to identify the groups of patients most likely to benefit from antibiotics, which antibiotics should be used when needed and, particularly for the large groups of patients for whom antibiotics are ineffective, alternative treatments.
In conclusion, children with UTI should be treated with antibiotics, the choice of which should be dictated by previous antibiotic exposure, with nitrofurantoin the preferred option when trimethoprim resistance is suspected.
Notes
Competing interests
The authors have declared no competing interests.
Provenance
Commissioned; not externally peer reviewed.
- © British Journal of General Practice 2013
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

