Article Text

Navigate this article
Statistics from Altmetric.com
- Joint British Societies
- cardiovascular disease prevention
- Joint British Societies’ guidelines
- prevention of cardiovascular disease
- clinical practice
PREFACE
The Joint British Societies’ guidelines (JBS 2) on cardiovascular disease prevention in clinical practice were developed by a Working Party (see table) with nominated representatives from six professional societies. All members contributed to the text and those from the specialist societies of hypertension, lipids, and diabetes were specifically responsible for developing the sections on blood pressure, lipids, and glucose. All sections of the document represent an evidence based consensus by all professional societies involved. The scientific literature which informs the recommendations is referenced throughout the text and Dr Kornelia Kotseva is thanked for all her help in searches for systematic reviews and meta-analyses, and checking the referencing of all sections. We are grateful to both Mr Harry Heyes of the Department of Medical Illustration, University of Manchester, for the cardiovascular risk prediction charts artwork, and Mr Daniel Prais of Crawford’s Business Services, Salford, for the computer programming. Dr Paola Primatesta is thanked for providing prevalence estimates of total CVD risk in the adult population from the Health Survey for England. Mr Tim Collier (Statistician, London School of Hygiene and Tropical Medicine) is also thanked for preparing the figures on lipid trials. Despoina Xenikaki provided the Working Party with invaluable administrative support. This guideline was reviewed and approved by the boards of all the professional societies.
JBS 2 Working Party
GUIDELINES
SUMMARY
The aim of these new Joint British Societies’ guidelines (JBS 2) developed by the British Cardiac Society, British Hypertension Society, Diabetes UK, HEART UK, Primary Care Cardiovascular Society, and The Stroke Association is to promote a consistent multidisciplinary approach to the management of people with established atherosclerotic cardiovascular disease (CVD) and those at high risk of developing symptomatic atherosclerotic disease.
We recommend that CVD prevention in clinical practice should focus equally on (i) people with established atherosclerotic CVD, (ii) people with diabetes, and (iii) apparently healthy individuals at high risk (CVD risk of ⩾ 20% over 10 years) of developing symptomatic atherosclerotic disease. This is because they are all people at high risk of CVD. The object of CVD prevention in these high risk people is the same—namely, to reduce the risk of a non-fatal or fatal atherosclerotic cardiovascular event and to improve both quality and length of life. This can be achieved through lifestyle and risk factor interventions and appropriate drug therapies to lower blood pressure, modify lipids, and reduce glycaemia. We have set targets (see below) for lifestyle, blood pressure, lipids, and glucose for these high risk people. Cardiovascular protective drug therapies have specific clinical indications. For all high risk people a number of drugs from different classes will reduce the risk of recurrent disease and increase life expectancy: antithrombotic, blood pressure, lipid, and glucose lowering therapies.
(I) OBJECTIVE OF CVD PREVENTION IN CLINICAL PRACTICE
The specific objective of CVD prevention for all high risk people in clinical practice is to reduce the risk of CVD and its complications, including the need for percutaneous or surgical revascularisation procedures in any arterial territory, and to improve quality of life and life expectancy.
(II) PRIORITIES FOR CVD PREVENTION IN CLINICAL PRACTICE
CVD prevention in clinical practice should focus on all those people who are at high risk, and the following groups of people have equal priority for CVD prevention in clinical practice.
-
People with any form of established atherosclerotic CVD
-
Asymptomatic people without established CVD but who have a combination of risk factors which puts them at high total risk (estimated multifactorial CVD risk ⩾ 20% over 10 years) of developing atherosclerotic CVD for the first time
-
People with diabetes mellitus (type 1 or 2)
These three groups all require professional lifestyle and multifactorial risk factor management to defined lifestyle and risk factor targets.
In addition, other people with particularly elevated single risk factors also require CVD prevention because they too are at high cardiovascular risk, regardless of the presence of other risk factors:
-
elevated blood pressure ⩾ 160 mm Hg systolic or ⩾ 100 mm Hg diastolic, or lesser degrees of blood pressure elevation with target organ damage
-
elevated total cholesterol to high density lipoprotein (HDL) cholesterol ratio ⩾ 6.0
-
familial dyslipidaemia, such as familial hypercholesterolaemia or familial combined hyperlipidaemia.
Finally, people with a family history of premature CVD should be assessed for their cardiovascular risk and then managed appropriately
(III) CARDIOVASCULAR RISK ESTIMATION
All adults from 40 years onwards, who have no history of CVD or diabetes, and who are not already on treatment for blood pressure or lipids, should be considered for an opportunistic comprehensive CVD risk assessment in primary care. Younger adults (< 40 years) with a family history of premature atherosclerotic disease should also have their cardiovascular risk factors measured.
Risk assessment should include ethnicity, smoking habit history, family history of CVD, and measurements of weight, waist circumference, blood pressure, non-fasting lipids (total cholesterol and HDL cholesterol), and non-fasting glucose. The new Joint British Societies’ CVD risk prediction chart (figs 1 and 2—see inside front and back covers) should be used to estimate total risk of developing CVD (coronary heart disease (CHD) and stroke) over 10 years based on five risk factors: age, sex, smoking habit, systolic blood pressure, and the ratio of total cholesterol to HDL cholesterol. This is the estimated probability (percentage chance) of developing CVD over the next 10 years. We refer to this as total CVD risk in this document. Total CVD risk should be estimated for the person’s current age group: < 50 years, 50–59 years, or ⩾ 60 years. A total CVD risk of ⩾ 20% over 10 years is defined as “high risk” and requires professional lifestyle intervention and, where appropriate, drug therapies to achieve the lifestyle and risk factor targets.

Joint British Societies’ cardiovascular disease (CVD) risk prediction chart: non-diabetic men.

Joint British Societies’ CVD risk prediction chart: non-diabetic women.
Other risk factors not included in the CVD risk prediction charts should be taken account of in assessing and managing a person’s overall CVD risk. In some ethnic groups the risk charts can underestimate, or sometimes overestimate, CVD risk because they have not been derived from these populations. For example, in people originating from the Indian subcontinent it is reasonable to assume that CVD risk is about 1.4 times higher than predicted from the charts. Abdominal obesity (waist circumference: men ≥ 102 cm, women ≥ 88 cm, and in Asians ≥ 90 cm in men and ≥ 80 cm in women) increases the risk of diabetes and CVD. Impaired glucose regulation is defined as impaired fasting glucose (IFG) or impaired glucose tolerance (IGT) and both are associated with an increased risk of developing diabetes and CVD. If non-fasting glucose is ⩾ 6.1 mmol/l then measure fasting glucose for evidence of impaired glucose regulation or new diabetes (see section II (iii) “Blood glucose and diabetes”). Raised fasting triglyceride (> 1.7 mmol/l) increases the risk of CVD. A family history of premature CVD, and especially CHD (men < 55 years and women < 65 years) in a first degree relative increases the risk of developing CVD by about 1.3.
Those who are not found at this comprehensive cardiovascular risk assessment to be at high total CVD risk based on the Joint British Societies’ charts, or started for other reasons on drug therapy to lower blood pressure, lipids, or glucose, should have their risk assessment repeated, ideally within five years. Under the age of 40 years the 10 year total CVD risk will usually be low but the risk in the coming years, assuming risk factors do not change, can be tracked forward to older age groups. Over the age of 70 years CVD risk is usually ⩾ 20% over 10 years, especially for men, but total CVD risk should still be formally estimated using the charts. However, this will underestimate the true total CVD risk of a person older than 70 years.
For people with established atherosclerotic CVD, hypertension with target organ damage, familial dyslipidaemias such as familial hypercholesterolaemia, or diabetes, formal risk estimation is not necessary; all these people are at high total CVD risk.
(IV) THRESHOLDS FOR THERAPEUTIC TREATMENT IN HIGH RISK PEOPLE
The following thresholds are recommended for more intensive lifestyle intervention and the appropriate use of antihypertensive, lipid lowering, glucose lowering and other cardiovascular protective therapies in order to reduce the overall cardiovascular risk:
-
(i) Clinical evidence of atherosclerotic CVD
or
-
(ii) Diabetes mellitus (type 1 or 2)
or
-
(iii) A total CVD risk ⩾ 20% over 10 years
or
-
(iv) Elevated blood pressure ⩾ 160 mm Hg systolic or ⩾ 100 mm Hg diastolic, or lesser degrees of blood pressure elevation with target organ damage
or
-
(v) Elevated total cholesterol to HDL cholesterol ratio ⩾ 6.0
or
-
(vi) Diagnosis of a familial dyslipidaemia—for example, familial hypercholesterolaemia or familial combined hyperlipidaemia
(V) LIFESTYLE, RISK FACTOR, AND THERAPEUTIC TARGETS IN HIGH RISK PEOPLE
Lifestyle targets
Lifestyle intervention in all high risk people to discontinue smoking, make healthier food choices, increase aerobic physical activity, and achieve optimal weight and weight distribution is central to CVD prevention. Involvement of the whole family may be helpful together with community resources.
Other risk factor targets
(i) Blood pressure and hypertension
In all high risk people rigorous control of blood pressure (BP) is recommended with the following treatment targets:
The optimal BP target is < 140 mm Hg systolic and < 85 mm Hg diastolic. In selected higher risk people (established atherosclerotic disease, diabetes, and chronic renal failure) a lower BP target of < 130 mm Hg and < 80 mm Hg may be more appropriate. These targets can usually be achieved with antihypertensive drugs prescribed at doses, and in combinations, whose efficacy and safety have been shown in trials.
An “audit standard” of < 150 mm Hg systolic and < 90 mm Hg diastolic is also recommended. For the higher risk people with atherosclerotic disease, diabetes, or renal failure the recommended audit standard is < 140 mm Hg systolic and < 80 mm Hg diastolic. However, these audit standards are considered to be the minimum standard of care for such high risk people. Wherever possible, the optimal treatment targets should be achieved.
(ii) Blood lipids and dyslipidaemia
In all high risk people rigorous control of blood cholesterol is recommended with the following treatment targets:
The optimal total cholesterol target is < 4.0 mmol/l and low density lipoprotein (LDL) cholesterol < 2.0 mmol/l, or a 25% reduction in total cholesterol and a 30% reduction in LDL cholesterol, whichever gets the person to the lowest absolute value. HDL cholesterol and triglyceride values should also be considered in overall lipid management. The total and LDL cholesterol targets can usually be achieved with lipid lowering drugs prescribed at doses whose efficacy and safety have been shown in trials.
An “audit standard” for total cholesterol of < 5.0 mmol/l (or a 25% reduction in total cholesterol) and for LDL cholesterol of < 3.0 mmol/l (or a 30% reduction in LDL cholesterol), whichever gets the person to the lowest absolute level, is also recommended. This audit standard is considered to be the minimum standard of care for all high risk people. Wherever possible, the optimal treatment targets should be achieved.
(iii) Blood glucose and diabetes
In all high risk people the optimal fasting glucose is ⩽ 6.0 mmol/l.
If the non-fasting glucose is < 6.1 mmol/l it does not need to be repeated. If non-fasting glucose is ⩾ 6.1 mmol/l then measure fasting glucose for evidence of impaired glucose regulation or new diabetes. If this fasting glucose measurement is normal (⩽ 6.0 mmol/l) there is no need to repeat it. If the fasting glucose is abnormal (6.1–6.9 mmol/l) but not indicative of diabetes (⩾ 7.0 mmol/l) this should be repeated on a separate occasion, or an oral glucose tolerance test (OGTT) performed. If the second fasting glucose is still abnormal (6.1–6.9 mmol/l) the person has impaired fasting glycaemia (IFG). If fasting glucose values are both ⩾ 7.0 mmol/l, on separate occasions, the diagnosis of diabetes is made regardless of symptoms. In the presence of diabetic symptoms (thirst, polyuria, and weight loss) a fasting glucose ⩾ 7 mmol/l on one occasion is considered diagnostic of diabetes. An OGTT is the only way to diagnose impaired glucose tolerance (IGT) (2 hour glucose ⩾ 7.8 mmol/l but < 11.1 mmol/l) and is the conventional standard for the diagnosis of diabetes mellitus (2 hour glucose ⩾ 11.1 mmol/l).
For people with impaired glucose regulation (either IFG or IGT) the aim is to prevent progression to diabetes and CVD through lifestyle intervention and, where appropriate, drug therapies. These people should be followed up annually to reassess glucose regulation and all other cardiovascular risk factors.
For people with type 1 and 2 diabetes mellitus rigorous control of glycaemia is recommended with the following treatment targets:
The optimal target for glycaemic control in diabetes is a fasting or pre-prandial glucose value of 4.0–6.0 mmol/l and a HbA1c < 6.5%. An audit standard for HbAlc of < 7.5% is recommended.
Cardiovascular protective drug therapy
Cardiovascular protective drug therapy should be considered in all high risk people and prescribed selectively at the doses whose efficacy and safety have been shown in clinical trials as described below.
(i) Antithrombotic therapy
Coronary and peripheral atherosclerotic disease
Aspirin 75 mg daily is recommended for life for all people with coronary or peripheral atherosclerotic disease. If aspirin is contraindicated, or there are side effects, then clopidogrel 75 mg daily is appropriate.
Anticoagulation (for example, warfarin with an international normalised ratio (INR) in the range of 2.0–3.0) should be considered for selected people at risk of systemic embolisation from large myocardial infarctions, heart failure, left ventricular aneurysm, or paroxysmal tachyarrhythmias.
Cerebral atherosclerotic disease (non-haemorrhagic)
For all people with a history of cerebral infarction, or transient ischaemic attack (TIA), and who are in sinus rhythm, aspirin 75–150 mg daily plus dipyridamole M/R (modified release) 200 mg twice daily is recommended for two years following the initial event to prevent stroke recurrence as well as other vascular events. If aspirin is contraindicated, or there are side effects, clopidogrel 75 mg daily is an alternative. For those who have a further ischaemic cerebrovascular event while taking aspirin and dipyridamole M/R, then changing aspirin for clopidogrel 75 mg daily should be considered.
Anticoagulation should be considered for all people with atrial fibrillation who are at moderate (aged 60–75 years without additional risk factors) to high risk (> 75 years, or > 60 years with other risk factors such as hypertension, diabetes, or left ventricular dysfunction) to reduce the risk of a further stroke. If oral anticoagulation is contraindicated, or cannot be tolerated, antiplatelet therapy should be considered instead.
There is no evidence of benefit for anticoagulation in people with ischaemic stroke who are in sinus rhythm.
High risk people without established CVD
Aspirin 75 mg daily is recommended for all people over the age of 50 years who have a total CVD risk ⩾ 20%, and in selected people with diabetes (≥ 50 years, or who are younger but have had the disease for more than 10 years, or who are already receiving treatment for hypertension), once the blood pressure has been controlled to at least the audit standard of < 150mm Hg systolic and < 90 mm Hg diastolic.
(ii) Blood pressure lowering therapy
(a) β Blockers
A β blocker is recommended for all people following myocardial infarction unless there are contraindications. The evidence for β blockade is strongest for those people with a large myocardial infarction, or infarction complicated by heart failure or ventricular arrhythmias.
(b) ACE inhibitors
An angiotensin converting enzyme (ACE) inhibitor is recommended for people with symptoms or signs of heart failure at the time of myocardial infarction, or those with persistent left ventricular (LV) systolic dysfunction (ejection fraction < 40%) following infarction. An ACE inhibitor should be considered for others with coronary artery disease, especially if the blood pressure is not below the target of < 130 mm Hg systolic and < 80 mm Hg diastolic. An angiotensin II receptor blocker (ARB) is an alternative to an ACE inhibitor if the latter is associated with side effects.
An ACE inhibitor should be considered in combination with a thiazide/thiazide-like diuretic in all people with an established stroke, especially if the blood pressure is not below the target of < 130 mm Hg systolic and < 80 mmHg diastolic.
(c) Calcium channel blockers
A calcium channel blocker should be considered in all high risk people if the blood pressure is not below the target.
(d) Diuretics
A diuretic should be considered in all high risk people if the blood pressure is not below target.
(iii) Lipid lowering therapy
(a) Statins
A statin is recommended for all high risk people with established atherosclerotic disease, and in most people with diabetes (see below), and others at high total risk of developing CVD.
In people with an acute coronary syndrome, cerebral infarction or TIA a statin should, for practical reasons, be prescribed during the inpatient stay. For people with cerebral atherosclerotic disease a statin is indicated to reduce the risk of a further major cardiovascular event. Fasting lipids should be estimated at least eight weeks after the acute cardiovascular event and, if necessary, the dose of statin up-titrated to achieve the total and LDL cholesterol targets. HDL cholesterol and fasting triglycerides should be measured and considered at the same time.
In people with diabetes statin therapy is recommended for:
(1) all those who are aged 40 years or more with either type 1 or 2 diabetes, and
(2) for people aged 18–39 years with either type 1 or 2 diabetes and who have at least one of the following:
(a) retinopathy (pre-proliferative, proliferative, maculopathy)
(b) nephropathy, including persistent microalbuminuria
(c) poor glycaemic control (HbA1c > 9%)
(d) elevated blood pressure requiring antihypertensive therapy
(e) raised total blood cholesterol (⩾ 6.0 mmol/l)
(f) features of metabolic syndrome (central obesity and fasting triglyceride > 1.7 mmol/l (non-fasting > 2.0 mmol/l) and/or HDL cholesterol < 1.0 mmol/l in men or < 1.2 mmol/l in women)
(g) family history of premature CVD in a first degree relative.
In asymptomatic people who are at high total risk of developing CVD a statin is recommended if the total cholesterol and LDL cholesterol targets have not been achieved.
(b) Other lipid lowering drugs
Other classes of lipid lowering drugs (fibrates, bile acid sequestrants, cholesterol absorption inhibitors, nicotinic acid, omega-3 (n-3) fatty acids) should be considered in addition to a statin if the total and LDL cholesterol targets have not been achieved, or if other lipid parameters such as HDL cholesterol or triglycerides need to be addressed.
(VI) ORGANISATION OF PREVENTIVE CARE IN HOSPITAL
The care of people with CVD and those at high risk of developing this disease ideally requires cardiovascular physicians with a special interest in prevention and rehabilitation. All people with atherosclerotic disease should have access to a comprehensive cardiovascular prevention and rehabilitation programme. Such a service should be available for these people and their families through the specialities of cardiology, neurology, vascular surgery, renal medicine, general internal medicine, diabetes, care of the elderly and others. This service should start during the inpatient stay and continue following discharge to the community. Similarly, the care of asymptomatic high risk people in hypertension, lipid, and diabetes clinics requires coordination between specialists to ensure a common clinical approach to preventive cardiovascular care.
Common protocols
Care of people with CVD should be integrated between hospital and general practice through the use of agreed protocols designed to ensure optimal long term lifestyle, risk factor, and therapeutic management. Similarly, the care of high risk people treated in specialist hospital clinics should be integrated with general practice to ensure, through agreed protocols, optimal long term management.
Screening of first degree relatives
Screening of first degree blood relatives (principally siblings and offspring) of people with premature CVD (men < 55 years and women < 65 years) is encouraged through primary care, and is essential in the context of familial dyslipidaemias. All first degree relatives, of any age, of those affected by familial dyslipidaemia should also be screened and specialist care provided through a lipid clinic.
Audit
Auditing the care received by all high risk people admitted to hospital or seen in specialist outpatient clinics will enhance improved care.
(VII) ORGANISATION OF PREVENTIVE CARE IN GENERAL PRACTICE
In primary care the continuing care of people with CVD and their families should also embrace all aspects of cardiovascular prevention.
Identification of high risk people
Primary care is responsible for the identification and management of apparently healthy individuals at high total risk of developing CVD.
In apparently healthy individuals the decision to introduce drug therapy for blood pressure, lipids, or glucose should be strongly influenced by the estimation of total risk of developing CVD. As a general guide a total CVD risk of ⩾ 20% of developing CVD over the next 10 years is sufficiently high to justify drug treatment if targets have not been achieved. However, a final decision about using drug therapy will also be influenced by other factors, not included in the risk estimation model, such as co-existent non-vascular disease and life expectancy.
For apparently healthy individuals with a 10 year total CVD risk of < 20%, appropriate lifestyle advice—for example, to stop smoking—should still be given but drug treatment by physicians is usually not required.
Common protocols
The care of such high risk people in general practice should be based on agreed protocols with hospital specialists, and there should be appropriate follow up to ensure optimal long term management.
Audit
Auditing the care that high risk people receive in general practice will enhance improved care, and is a requirement of the new General Medical Services contract.
(I) INTRODUCTION
The Joint British Societies—British Cardiac Society, British Hypertension Society, British Hyperlipidaemia Association, and British Diabetes Association—published recommendations on coronary prevention in clinical practice in 1998 (JBS 1).1,2 This professional collaboration provided the leadership for a more unified, and hence effective, multidisciplinary approach to CVD prevention in clinical practice. In these recommendations we called for:
-
patient priorities for atherosclerotic disease prevention
-
a multifactorial approach to risk assessment and management in the asymptomatic population without CVD
-
enhanced integration of preventive care between hospital and general practice
-
the development of common clinical protocols
-
auditing the impact of such protocols on the management of people with CHD and other atherosclerotic vascular disease and asymptomatic individuals at high risk of developing CHD.
The British Heart Foundation distributed the 1998 recommendations as Fact Files, together with a poster version of the coronary risk prediction charts, to all general practitioners. The British National Formulary also published the risk charts as a guide to prescribing thresholds for antihypertensive and lipid lowering therapies, and these charts continue to be part of each new edition.
National Service Framework for CHD
In 2000 the National Service Framework (NSF) for CHD set standards for the prevention and treatment of CHD.3 The NSF adopted the same priorities defined in JBS 1 for CHD prevention—namely, (1) people with established CHD, and (2) apparently healthy individuals at high multifactorial risk of developing CHD. The NSF recommended the Joint British Societies’ coronary risk prediction charts (and software program) for total CHD (and cardiovascular (CVD)) risk estimation in the asymptomatic population without CVD. We had recommended that individuals whose total CHD risk was ⩾ 15% (equivalent to a CVD risk of ⩾ 20%) over 10 years were eligible for both lifestyle and appropriate therapeutic interventions. We considered this risk threshold sufficiently high to justify prescribing for both antihypertensive and lipid lowering therapies. Given the scale of the task in identifying and managing all such high risk people in primary care we advocated a staged approach to risk reduction. The starting point was those at highest total CHD risk (⩾ 30%) and then, as resources allowed, targeting those at the next level of risk, namely ⩾ 15%. Although the NSF endorsed the CHD risk threshold of ⩾ 15% for all classes of antihypertensive therapies, it made the pragmatic recommendation that statins be targeted only at those asymptomatic individuals with a total CHD risk of ⩾ 30%. This policy of targeting only those at very high risk for lipid lowering therapy fell far short of the scientific evidence base in 2000. The results of randomised control trials of lipid lowering therapy had already shown evidence of clinical benefit at total CHD risk thresholds down to 6% (approximately 8% CVD risk) over 10 years by that time. A total risk of ⩾ 30% in asymptomatic individuals is higher than the risk of a further coronary event for many people with established coronary disease. At this level of CHD risk virtually no asymptomatic women under 60 years of age are eligible for lipid lowering medication. Hence, this NSF policy on lipid prescribing was too conservative in relation to the scientific evidence. With the publication of new major clinical trial data on lipid lowering since 2000 this restrictive policy on statins cannot be justified. The scientific evidence base for lipid lowering therapy is now even stronger, and this has now been recognised by recent NICE (National Institute for Health and Clinical Excellence) appraisal of statins for the prevention of cardiovascular events (www.nice.org.uk). Statin therapy is recommended for adults with clinical evidence of CVD, and for the primary prevention of CVD for adults who have a 20% or greater 10 year risk of developing CVD.
The challenge for preventive cardiovascular medicine
The NSF for England endorsed the lifestyle and risk factor targets defined in JBS 1 for people with established CHD, and for asymptomatic individuals whose total CHD risk was ⩾ 15% (CVD risk ⩾ 20%) over 10 years.
The NSF put in place national audit standards and these are currently being reinforced and expanded by the new General Medical Services (GMS) contract for primary care in the UK.4 These standards are intended to assist clinical practice to achieve the lifestyle, risk factor, and therapeutic goals for high risk people. The challenge facing the care of people with atherosclerotic disease is considerable and there is a pressing need for a comprehensive prevention and rehabilitation strategy. In the Health Survey for England in 2003 the prevalence of CHD (angina and heart attack) was 7.4% in men and 4.5% in women.5 With stroke added the CVD prevalence was 9.1% and 6.3%, respectively. From age 65 onwards between a quarter and a third of men reported having had coronary disease or a stroke, the prevalence rising with age: 26% (65–74 years) and 34% (⩾ 75 years) in men, and 14% and 25%, respectively, for women. The prevalence of cerebrovascular disease is also increasing. Between 1994, 1998 and 2003 it rose from 7.1% to 8.5% and 9.1% in men (the increase between 1998 and 2003 in men was seen only among the older age groups, 65–74 and 75+) and in women to a lesser extent, from 5.2% to 6.2% and 6.3%. Yet, the EUROASPIRE surveys show a majority of these cases are still not achieving the recommended lifestyle, blood pressure, and lipid targets6 despite an increase in prescribing of antihypertensive and lipid lowering therapies in the second survey compared to the first survey in the mid 1990s.7 Unfortunately, the second survey found an adverse trend for smoking, particularly among younger females. Obesity had also increased notably, with a corresponding increase in diabetes (a third of which was not medically detected). Half of all people in the second survey had not achieved the blood pressure target and over half had not achieved the cholesterol target.6
For apparently healthy individuals with a combination of risk factors which puts them at high risk of developing CVD—elevated blood pressure, dyslipidaemia, impaired glucose regulation—the standard of clinical management is also a cause for concern. In the Health Survey for England (2003) the prevalence of smoking in those without CVD was 28% in men and 25% in women5; 64% of men and 55% of women were overweight (body mass index (BMI) > 25 kg/m2); 29% of men and 27% of women had hypertension (BP ≥ 140/90 mm Hg); 68% of men and 67% of women had an elevated cholesterol (> 5.0 mmol/l). The overall prevalence of diabetes, including those with established CVD, was 4.3% of men and 3.4% of women. Audits of clinical practice have shown many such high risk individuals are not detected in the community.8 Among those found to be at high risk there are still many who are not being managed effectively to contemporary risk factor targets. However, this picture is likely to improve under the new GMS contract with increasing emphasis on the importance of preventive medicine in primary care.4
Joint British Societies
Since JBS 1, new scientific evidence has been published on blood pressure management, lipid lowering in atherosclerotic and high risk people, risk factor control in medically diagnosed diabetes, and prevention of diabetes. There is also new evidence for some prophylactic drug therapies, both in people with atherosclerotic disease and those at high risk of developing CVD. Therefore, a second joint working party was convened to revise the 1998 recommendations. The original four professional societies (the British Hyperlipidaemia Association and the Family Heart Association have now amalgamated to form HEART UK (Hyperlipidaemia Education And Research Trust UK), and the British Diabetes Association is now renamed Diabetes UK) have now been joined by the Stroke Association, because of the importance of addressing all aspects of atherosclerotic disease, and the Primary Care Cardiovascular Society. The latter society is particularly important because general practitioners and other health care professionals working in primary care organisations have the lead responsibility, and best clinical opportunity, for delivering preventive strategies for all priority groups.
Scope of new guidelines
The scope of these new Joint British Societies’ (JBS 2) guidelines now encompasses the whole of atherosclerotic CVD—that is, acute coronary syndromes, exertional angina, cerebrovascular disease (transient cerebral ischaemia and non-haemorrhagic atherosclerotic stroke and haemorrhagic stroke) and peripheral atherosclerotic disease—rather than highlighting CHD. Our original recommendations addressed both coronary atherosclerotic disease and other atherosclerotic disease, but coronary disease was given top priority. It is now even more appropriate to address atherosclerotic CVD as a whole because new scientific evidence since 1998 provides greater justification for the prevention of other forms of atherosclerotic disease. Any symptomatic manifestation of atherosclerosis in any vascular territory puts a person at high risk of dying from CVD, mainly from coronary artery disease. Therefore it is appropriate to offer the same lifestyle and risk factor management to all people with atherosclerotic disease. Cardioprotective drug therapies are selected according to the affected vascular territory, such as β blockers following a myocardial infarction. Similarly, for asymptomatic individuals at high total risk of developing symptomatic CVD the objective is the same, namely to reduce the risk of developing coronary disease, stroke (including transient cerebral ischaemia), aneurysm of a major artery, or lower limb claudication.
Evaluation of scientific evidence
Evidence based medicine is defined as the integration of individual clinical expertise with the best available clinical evidence from systematic research.9 It involves defining important clinical questions, searching for best evidence, critically appraising the evidence, applying the evidence to individual patient care, and evaluating the process.
The hierarchy of evidence places meta-analyses of clinical trials at the top and case reports at the bottom. In the context of CVD prevention this hierarchy gives greater weight to controlled trials of drug therapies rather than epidemiological studies of smoking, diet, and physical activity. For example, the epidemiology of smoking and risk of developing CVD is compelling, and observational data show the substantial benefits of stopping smoking for both people with coronary or other atherosclerotic disease and for asymptomatic individuals. While a clinical trial is well suited to evaluating a single drug treatment against placebo there are inherent limitations in the methodology of clinical trials when evaluating complex interrelated lifestyle changes in a free living population. Hence, if only clinical trial evidence is followed, drug treatments will always take precedence over other interventions; principally those related to lifestyle change.
Therefore, in these guidelines we have taken account of scientific evidence from both observational (epidemiology) and experimental (randomised controlled trials) studies and, wherever possible, such evidence is based on systematic reviews or meta-analyses rather than single observational studies or trials. Although we have given prominence to systematic reviews and meta-analyses of both observational and experimental data, single studies are also cited when they give a clear answer to a clinical question.
General Medical Services contract
The new GMS contract for primary care in England and Wales defines quality indicators which will be an incentive to more effective CVD prevention.4 Practices are required to produce a register of people with CHD, stroke, hypertension, and diabetes mellitus to ensure they receive appropriate preventive advice and treatment over the long term. Although the concept of people at high total CVD risk is not embraced in the GMS contract it does set thresholds and targets for all the major risk factors. In each high risk group there are thresholds for recording and controlling risk factors—smoking status, a blood pressure < 150/90 mm Hg (< 145/85 mm Hg in diabetes), a total cholesterol < 5.0 mmol/l, and a HbA1c < 7.4%—and for prescribing various cardioprotective drug therapies with specific clinical indications. Each of these quality indicators attracts points. There is a minimum threshold for each standard and beyond this point funding increases, proportionally to achievement, until the maximum threshold is reached. Better quality preventive care will result in fewer CVD events for people and greater financial rewards for the practices. The thresholds and standards in the GMS contract for recording and controlling risk factors represent the minimum standard of preventive cardiovascular care in relation to the scientific evidence.
Over the counter statins
While the JBS 2 guidelines were being developed a national policy authorising pharmacists to provide low dose simvastatin (10 mg) to individuals at moderate CVD risk was adopted in this country.10 This policy applies to all men aged 55 years and over without other risk factors, and to men aged 45–54 or women aged ⩾ 55 years with one or more risk factors (current smoker, obese, family history of premature CHD or of Asian origin). It does not apply to people who have CVD, diabetes, familial dyslipidaemias, or who are already taking lipid lowering medication or other therapies that might interact with a statin. Our clinical guidelines focus exclusively on the management of high risk people, who remain the sole responsibility of clinicians in hospital and general practice, and this new approach to providing low dose statin through pharmacies has no bearing on our recommendations. Prescribing appropriate doses of statins whose efficacy and safety has been evaluated in clinical trials is the ongoing responsibility of clinicians. Clinicians should continue to manage high risk people, prescribe statins at appropriate doses, monitor their therapeutic effect, up-titrate as necessary to achieve lipid targets, and address all other risk factors as required.
Managing high risk people in clinical practice
The biology of atherosclerotic disease and its complications makes the traditional separation of “secondary” from “primary” prevention illogical. People with established CVD and those at high risk of developing CVD are all considered to be high risk people who have some degree of atherosclerosis or vascular dysfunction, whether symptomatic or not; in other words they all have the same underlying disease process.
So we now recommend that CVD prevention in clinical practice should focus equally on people with established atherosclerotic CVD, people with diabetes, and asymptomatic individuals at high total risk (CVD risk of ⩾ 20% over 10 years) of developing symptomatic atherosclerotic disease, because they are all at high risk. People with diabetes are not only at higher risk of developing atherosclerotic disease but also have a higher case fatality. Waiting until people have sustained tissue damage and then focusing preventive efforts on them, while giving lower priority to the many at high risk of developing symptomatic atherosclerotic disease, is counter intuitive, particularly when the initial clinical presentation can be sudden death. The focus of preventive cardiovascular care must therefore be to prevent both the development of atherosclerotic disease as well as recurrent disease.
So the object of CVD prevention in all these high risk people is the same; namely, to reduce the risk of a non-fatal or fatal atherosclerotic cardiovascular event and to improve both quality and length of life. This can be achieved through lifestyle and risk factor interventions and appropriate drug therapies to lower blood pressure, modify lipids, and reduce glycaemia. In clinical practice it is appropriate to manage people with established CVD, and those at high total CVD risk, to the same lifestyle targets and to achieve specific targets for blood pressure, lipids, and glucose. Cardioprotective protective drug therapies all have specific clinical indications. For all high risk people a number of drugs from different classes (antithrombotic, blood pressure, and lipid lowering therapies) will reduce the risk of disease and increase life expectancy. High risk people should be managed by physicians supported by clinical teams who are able to address all aspects of CVD prevention. Health professionals such as nurses, dieticians, physiotherapists, and others have a central role in team delivery of professional preventive care in hospital and general practice.
Overall aim of JBS 2
The overall aim of JBS 2 is to continue to promote a consistent multidisciplinary approach to the personalised management of people with established atherosclerotic CVD, diabetes, and others at high risk of developing symptomatic CVD; to emphasise a total risk approach to CVD risk assessment in the asymptomatic population; and to define lifestyle and risk factor interventions with thresholds and targets which reflect the growing scientific evidence base for managing high risk people.
REFERENCES
1
2
3
4
5
6
7
8
9
10
(II) OBJECTIVES AND PRIORITIES FOR CARDIOVASCULAR DISEASE PREVENTION IN CLINICAL PRACTICE
Objective for CVD prevention in clinical practice
The objective of CVD prevention for all high risk people in clinical practice is to reduce the risk of cardiovascular disease and its complications, including the need for percutaneous or surgical revascularisation procedures in any arterial territory, and to improve quality of life and life expectancy.
Priorities for CVD prevention in clinical practice
CVD prevention in clinical practice should focus on all those people who are at high risk, and the following groups of people have equal priority for CVD prevention in clinical practice.
-
People with any form of established atherosclerotic CVD
-
Asymptomatic people without established CVD but who have a combination of risk factors which puts them at high total risk (estimated multifactorial CVD risk ⩾ 20% over 10 years) of developing atherosclerotic CVD for the first time
-
People with diabetes mellitus (type 1 or 2)
These three groups all require professional lifestyle and multifactorial risk factor management to defined lifestyle and risk factor targets:
In addition, other people with particularly elevated single risk factors also require CVD prevention because they too are at high cardiovascular risk, regardless of the presence of other risk factors:
-
elevated blood pressure ⩾ 160 mm Hg systolic or ⩾ 100 mm Hg diastolic, or lesser degrees of blood pressure elevation with target organ damage
-
elevated total to HDL cholesterol ratio of ⩾ 6.0
-
familial dyslipidaemia, such as familial hypercholesterolaemia or familial combined hyperlipidaemia.
Finally, people with a family history of premature CVD should be assessed for their cardiovascular risk and then managed appropriately.
(III) CONCEPT AND ESTIMATION OF TOTAL CARDIOVASCULAR RISK
The concept of medical intervention based on estimated total coronary or CVD risk in the asymptomatic population without CVD is now widely advocated in this country,1–4 the European continent,5 the USA,6 and internationally.7 Since 1998 the Joint British Societies’ coronary risk prediction charts have become widely available, and have subsequently been published in every edition of the British National Formulary. Therefore, it has been easy for physicians to estimate total CHD risk (or CVD risk using a software program) as a basis for prescribing antiplatelet, antihypertensive, or lipid lowering therapy in the context of CVD prevention in the asymptomatic population.
The rationale for estimating total CVD risk based on the major risk factors is that (i) CVD is multifactorial in origin; (ii) risk factors tend to cluster; and (iii) co-existent risk factors tend to have a multiplicative effect on CVD risk.8 Therefore in assessing CVD risk of an individual it is important to take account of all risk factors. The level of any one risk factor taken in isolation, such as tobacco exposure, blood pressure, or blood cholesterol, is an inadequate guide to overall cardiovascular risk, and the potential benefit from lifestyle and therapeutic interventions. Thus, for example, for a given level of blood pressure the total risk of a major CVD event may vary several fold depending on the presence of other risk factors. Although at any level of total CVD risk the relative benefits of blood pressure lowering will be the same, the absolute benefits of such treatment will be greatest in those at highest total CVD risk. However, exceptions to this concept of treatment on the basis of total CVD risk exist. For example, when blood pressure is particularly high treatment is required regardless of total CVD risk.
Total CVD risk for an asymptomatic individual is estimated from several risk factors (age, sex, smoking habit, systolic blood pressure, and the ratio of total to HDL cholesterol) and is expressed as a probability (percentage chance) of developing CVD over a defined period of time which in this guideline is calculated over 10 years. This is the number of cardiovascular events which would be expected over 10 years in 100 men or women with the same risk factors as those in the person being assessed. In clinical practice we prefer the term “total risk” which is synonymous with the epidemiological term “absolute risk”. So when a person asks the doctor what are his or her chances of developing CVD the answer is an estimate of that person’s “total CVD risk”—for example, 20% over 10 years—in other words a one in five chance. The relative CVD risk for one individual compared to another is the ratio of their respective total or absolute risks. So when a person asks what are his or her chances of developing CVD compared to someone of the same age who has no risk factors for CVD, the answer is that person’s relative risk—for example, three times the chance of developing CVD compared to someone with no risk factors.
Therefore, in assessing the potential impact of a risk factor, such as blood pressure or cholesterol, on the chances of an asymptomatic person developing CVD it is important to first estimate their total CVD risk. This is done by taking simultaneous account of all their major cardiovascular risk factors. Those who are at highest total CVD risk are then identified and the management of their blood pressure or lipids can be addressed in this overall context. For the same cholesterol value—for example, 5.6 mmol/l—some individuals will be eligible for lipid lowering therapy and others not, depending on their total CVD risk. As a general rule clinicians should use total CVD risk, rather than any one risk factor alone, when making a clinical decision to start drug treatment to lower blood pressure or lipids, or inhibit platelet aggregation. However, if any one risk factor is particularly high it may require treatment in its own right.
The advantages of a multifactorial approach to identification and treatment of high risk individuals are:
-
The concept of total CVD risk replaces the traditional dichotomous classification of risk factors in most people. The physician asks the question “What is this person’s CVD risk?” rather than does this person have “hypertension” or “hypercholesterolaemia”. In other words, the physician considers the person’s blood pressure and lipid values in the context of overall CVD risk. Even in people with very high single risk factors, the levels of other factors will still influence their total CVD risk.
-
The threshold of total CVD risk at which drug treatments are given is based on an integral of scientific evidence and practical considerations in relation to the delivery of care. A high risk person was defined in the JBS 1 report as one whose 10 year CHD risk was 15% or more (equivalent to a cardiovascular risk of ⩾ 20% over the same period) or that the risk will be ⩾ 15% (or ⩾ 20% CVD risk) when projected to age 60 years. A staged approach was advocated starting with those with a total CHD risk ⩾ 30% over 10 years, and then progressing to those with a total CHD risk ⩾ 15% over 10 years as resources allowed. This initial CHD risk level of ⩾ 30% over 10 years was recommended primarily to reflect the ability of the health service to detect and care for these high risk individuals, rather than the strength of scientific evidence for therapeutic interventions in asymptomatic people to prevent CVD.
-
Whatever threshold of total CVD risk is chosen for drug treatments, they will by definition always be targeted at those at highest total CVD risk. Hence the absolute benefits of such treatments will always be greatest.
-
Inappropriate treatment of single risk factors in those at low total CVD risk is avoided.
-
It is consonant with clinical practice whereby physicians deal with the whole person rather than just one aspect of cardiovascular risk.
One disadvantage of this approach to prevention of CVD in the asymptomatic population is that treatments will tend to be concentrated in older people, and especially those > 70 years, unless the potential effect of lifetime risk factor exposure is taken into account. A younger individual will always be at low total CVD risk over the short term, although they may be at very high risk relative to peers of the same age. Considering only short term total CVD risk for a younger individual ignores the potential life-years to be gained by treating someone earlier when they are on track to become high risk in later life. In 1998 JBS 1 recommended projecting total CHD risk for younger individuals to age 60 years in order to identify those who will become high risk (CHD risk ⩾ 15%) in later years, and could therefore benefit from lifestyle and therapeutic interventions at an earlier age.
The Joint British Societies’ coronary risk prediction charts produced in 1998, and the associated “cardiac risk assessor” software program (which estimated both CHD risk and cardiovascular risk (including stroke) over a 10 year period) were based on age, sex, smoking, systolic blood pressure, and the ratio of total to HDL cholesterol. There was a separate chart for people with diabetes mellitus which included the same risk factors. CHD risk was classified into three categories (< 15%, 15–29% and ⩾ 30%). High risk individuals were defined as those whose 10 year risk of CHD was estimated to be ⩾ 15% (equivalent to a cardiovascular risk of ⩾ 20% over the same period) or whose risk would be ⩾ 15% (or ⩾ 20% CVD risk) if projected to age 60 years.
The new Joint British Societies’ cardiovascular risk assessment charts (figs 1 and 2—see inside front and back covers) differ in several important respects from these earlier charts, although both estimate risk based on the equations published from the Framingham study in 1991.1 The most important change is that CHD risk is now replaced by CVD risk. This is a combined end point of CHD (fatal and non-fatal myocardial infarction and new angina) plus stroke (fatal and non-fatal stroke and cerebral haemorrhage) and transient cerebral ischaemia. Some primary cardiovascular events, such as aortic aneurysm or lower limb ischaemia, are not included. However, on their own these represent a small proportion of all CVD events. The stroke end point is based on occlusive cerebral infarction (related both to blood pressure and lipids) but also includes intracerebral haemorrhage (related to blood pressure, but not to lipids) as well.
Charts provided are for three age ranges: < 50 years, 50–59 years, and ⩾ 60 years. However, the risks given for these three age ranges are based on the actual ages of 49, 59, and 69 years, respectively. Therefore, the charts will tend to overestimate risk within the two younger age bands (except in people aged exactly 49 or 59 years) and in the older age band overestimate risk for those aged < 69 years and underestimate risk for people aged 70 years or more.
Projecting risk in people aged < 50 years to their risk at 49 years takes account of the fact that using total CVD risk tends to target treatments away from younger people to older ages. Although the short term total CVD risk of younger people may not be great, their total lifetime risk may be exceptionally high. For example, a 34 year old woman who smokes, has a systolic pressure of 158 mm Hg, and a total to HDL cholesterol ratio of 5.9, has an absolute CVD risk over 10 years well below 20%. Therefore, on the basis of short term total risk she is not eligible for either antihypertensive or lipid lowering therapy. By contrast, most men over 70 years will qualify for both treatments simply because their age and sex takes them above the 20% threshold. Waiting until a person is old enough to reach the total CVD risk threshold for drug treatment means that a large proportion of potentially preventable clinical events will have happened, and for some vascular damage will be irreversible or death will have occurred. So projecting CVD risk to the age of 49 years in younger people will direct more antihypertensive and lipid lowering medication towards those at highest risk among this younger age group. Projecting risk in those < 50 years to that at age 49 is consistent with the policy of projecting that in 50 year olds to age 59 years, and that at 60 years to 69 years of age. By contrast, many people aged 70 years or older, and particularly men, are at a CVD risk ⩾ 20% over the next decade and their total CVD risk will be underestimated by the chart. Therefore, a decision to intervene in older persons requires individual clinical judgement based on clinical trial evidence where available. While looking at the potential risk of a younger person at age 60 years is still of interest, projecting risk to age 60 (as advocated in JBSL 1) should no longer be used as a basis for initiating drug treatments because these new charts contain a built in projection within each decade.
Younger people (< 40 years) should always be screened for cardiovascular risk factors if they have a strong family history of CHD or stroke early in life. This is arbitrarily defined in relation to CHD as the development of coronary disease in a male first degree relative < 55 years and a female first degree relative < 65 years. The first degree relatives of such people are at increased risk of developing CVD, and in some cases these families will have a genetic dyslipidaemia such as familial hypercholesterolaemia. CVD risk estimation is not appropriate in people with familial dyslipidaemias as they all require specialist treatment regardless of other risk factors.
Younger people may also come to medical attention because of a high blood pressure reading, or elevated cholesterol, from an occupational or insurance medical examination. In such cases projection of risk forward to age 49 years may be appropriate, although such a projection should not form the sole basis of any treatment decisions. Individual clinical judgement is required for the younger population. In younger people with an adverse risk factor profile their total CVD risk by the time they reach 49 years of age will be even higher than that shown on the charts on the basis of their current risk factor levels. This is because blood pressure, cholesterol and glucose all rise, and HDL cholesterol falls, with age which will increase total CVD risk.
In the JBS 2 cardiovascular risk charts, CVD risks of ⩾ 10%, ⩾ 20%, and ⩾ 30% over 10 years are highlighted. These are equivalent to CHD risks of about ⩾ 8%, ⩾ 15%, and ⩾ 23%, respectively. Although CVD risk is now used, the risk threshold for treatment with antihypertensive and lipid lowering therapies remains the same as recommended in 1998—namely, a CVD risk ⩾ 20% (red) over 10 years. This is equivalent to a CHD risk of ⩾ 15% over the same time period. The same risk threshold is still appropriate in 2005 for prescribing antihypertensive and lipid lowering medication in asymptomatic people. People at this high level of cardiovascular risk are a medical responsibility and all drugs, including statins, should be prescribed and monitored by physicians. As the general public require some guidance on whether a statin is of any value at moderate cardiovascular risk—namely, between 20% and 10% (orange) over 10 years—this risk band is also shown on the charts. There is clinical trial evidence that, at levels of cardiovascular risk as low as 8% over 10 years, individuals will on average benefit from statin treatment. So taking a statin in the range of CVD risk ⩾ 10% to < 20% (orange) is appropriate on the basis of scientific evidence, although absolute benefits will be small. When the cardiovascular risk is less than 10% (green) over the next 10 years, the benefit of treatment is not established and may be too small in absolute terms to justify drug treatment. However, recommendations for a healthy lifestyle are still as important.
The choice of risk assessment method will impact on the use of drug therapies in asymptomatic people.9 Although new risk assessment methods have become available since 1998 we decided to continue using the Framingham algorithm for the JBS 2 charts because the current alternatives do not offer sufficient advantage over Framingham to justify a change. The principal reason is that the JBS risk charts have been widely adopted and physicians in both hospital and primary care are familiar with a CHD risk threshold of ⩾ 15%, equivalent to a CVD risk threshold of ⩾ 20%, and to change this threshold could cause confusion. The alternative risk scores which were considered for JBS 2 are as follows. The first is a scoring system based on the Framingham offspring study used in conjunction with the US National Cholesterol Education Program ATP III recommendations.6 It predicts only fatal and non-fatal myocardial infarction because this is closer to the end points used in the statin trials. However, we consider it important to include cerebrovascular disease in risk estimation. While excluding angina as an end point in a clinical trial may be reasonable because of imprecision in its clinical diagnosis, it is not appropriate to exclude this diagnosis in cardiovascular risk estimation. This is because people who develop angina are at a much higher than average risk of future cardiovascular events. A second method of CVD risk estimation (HEARTSCORE) based on the SCORE project10 has been adopted by the Joint European Societies’ guidelines on CVD prevention.5 This has the major advantage of being based on European epidemiological studies and HEARTSCORE also predicts cardiovascular risk, not coronary risk alone. However, it can only predict fatal CVD which underestimates the true burden of total cardiovascular risk based on non-fatal and fatal cardiovascular events together. The risk threshold for treatment is therefore defined as fatal CVD ⩾ 5% over the next 10 years at current age, or when projected to age 60 years. This is considered to be the equivalent of a CVD risk ⩾ 20% based on Framingham. Although HDL cholesterol is included in the model it makes little contribution to risk prediction which could disadvantage certain groups, especially women. The most likely reason for this loss of predictive power for HDL cholesterol is a lack of standardisation in its measurement in the pooled epidemiological studies used for the SCORE project.
So we have decided to continue using the Framingham equation while recognising that it also has limitations. When applied to men aged 40–59 years at entry to the British regional heart study, a rate of fatal and non-fatal coronary events of 16% over 10 years was predicted whereas the observed rate was 10.2%.11 However, another recent study in the British population contrasting Framingham risk with hospital admission rates and other estimates of CHD prevalence found that the Framingham equation predicted lower than observed rates.12 The UK prospective diabetes study (UKPDS) risk engine based on a British diabetes trial population also predicts higher rates of CHD than those predicted by the Framingham equation for this group.13 However, before substituting Framingham with another algorithm for this country it is important to interrogate epidemiological databases derived from UK populations, and formally compare different risk assessment methods and then develop the optimal model for our population. Such a model will also have to take into account the range of CVD risks for different ethnic groups in our society.
In these new guidelines we have not produced a chart for estimating cardiovascular risk for people with diabetes mellitus. That is because we have recommended that all people with diabetes mellitus be considered “high risk” and managed to the same lifestyle and defined risk factor targets as people with established CVD and others at high total risk of developing CVD. This recommendation is made because most people with diabetes have a 10 year CVD risk ⩾ 20% and all have a risk greater than the population without diabetes. A computer program based on the UKPDS study—the UKPDS risk engine—is available for stratifying CVD risk in people with type 2 diabetes mellitus.13,14 This risk engine takes into account other risk factors including ethnicity, the HbA1c value after diagnosis, and duration of diabetes.
So for asymptomatic individuals without CVD the total CVD risk threshold defined in these guidelines for professional lifestyle intervention and appropriate drug therapies is ⩾ 20% over 10 years, which is equivalent to a CHD risk of ⩾ 15% over the same period. This threshold for drug treatment in terms of total CVD risk cannot be based directly on evidence from clinical trials. This is because most clinical trials, and especially those evaluating drug therapies, are unifactorial in their design. Therefore extrapolating from clinical trial results in hypertension or dyslipidaemia to an intervention threshold based on multifactorial risk is not possible. Nevertheless, absolute CVD event rates ⩾ 20% were common in most of the unifactorial intervention trials on which our recommendations are based. However, choosing a risk threshold for drug treatments is still a matter for clinical judgement. Clinicians should take account of the total CVD risk of people included in clinical trials, trial evidence on the efficacy and safety of drugs tested, and the practical translation of that trial evidence in selected people into effective medical care for all high risk populations.
The size of the population potentially eligible for preventive care needs to be defined for different levels of CVD risk. Using the Health Survey for England (2003) it has been estimated that at 20% CVD risk or higher, about 23% of men and 8% of women aged 40–74 years are potentially eligible for treatment (table 1). However, these prevalence estimates are based on single risk factor measurements. In clinical practice the actual numbers requiring drug treatment will be lower given the effects of lifestyle intervention and regression to the mean with repeat measurements of blood pressure and lipids over time. There are important resource implications for the NHS in the detection, assessment, and management of high risk individuals—organisation of opportunistic screening, laboratory and other investigations, lifestyle and therapeutic management, and life long follow up—which impact on general practice and specialised hospital clinics for hypertension, dyslipidaemia, and diabetes. All of these elements need to be taken into account in the development of the most cost effective delivery of preventive cardiovascular care.
Prevalence of total cardiovascular disease (CVD) (over 10 years) risk in adults aged 40–74 in England, by age and sex
In summary, the total CVD risk threshold for more intensive lifestyle and therapeutic intervention remains the same as that recommended in 1998 (total CHD risk ⩾ 15% over 10 years), but the emphasis is now on CVD (total CVD risk ⩾ 20% over 10 years) rather than CHD, and the risks calculated for each of the three decades (’40s, ’50s, and ’60s) are calculated for age 49, 59, and 69 years.
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
(IV) CLINICAL ASSESSMENT OF CARDIOVASCULAR RISK
All adults from 40 years onwards, who have no history of CVD or diabetes, and who are not already on treatment for blood pressure or lipids, should be considered for an opportunistic comprehensive CVD risk assessment in primary care once every five years. Those who are not found at this assessment to be at high total CVD risk based on the Joint British Societies’ charts, or started for other reasons on drug therapy to lower blood pressure, lipids, or glucose, should have their risk assessment repeated, ideally within five years. A short history, focused clinical examination, and a blood sample provide a simple, quick, practical assessment of total cardiovascular risk for asymptomatic individuals (table 2).
Identification of asymptomatic people at high total risk of developing CVD
CVD risk assessment should include ethnicity, smoking habit, family history of CVD, and measurements of weight, waist circumference, blood pressure, non-fasting lipids (total and HDL cholesterol) and non-fasting glucose. The new Joint British Societies’ CVD risk prediction chart (figs 1 and 2—see inside front and back covers) should be used to estimate total risk of developing CVD (CHD and stroke) over 10 years. If diabetes mellitus is diagnosed for the first time at this cardiovascular risk assessment, formal estimation of total CVD risk is not necessary as these people are all considered to be at high risk. All people with established atherosclerotic CVD, or an existing diagnosis of diabetes, do not require formal risk assessment. They should all receive professional lifestyle intervention and appropriate drug therapies to achieve all the risk factor targets defined in this guideline.
Joint British Societies’ CVD risk prediction chart
The clinician can estimate from the Joint British Societies’ CVD risk prediction charts (figs 1 and 2) the total risk of developing CVD over 10 years based on age, sex, lifetime smoking habit, systolic blood pressure before treatment, and the ratio of non-fasting total cholesterol to HDL cholesterol before treatment. However, this simple risk assessment can be subjectively refined by the physician by taking into account other risk factors such as family history, obesity, and especially central obesity, glucose for impaired glucose regulation (either impaired fasting glycaemia (IFG) or impaired glucose tolerance (IGT)) or diabetes, hypertriglyceridaemia, and evidence of any target organ damage—for example, retinopathy, renal impairment, or left ventricular hypertrophy. The assessment of all cardiovascular risk factors used in CVD risk estimation is described in detail below.
-
Age group—CVD risk should be estimated for the person’s current age group: < 50, 50–59, or ⩾ 60 years. For people under 40 years CVD risk will be overestimated because the chart is based on risk at age 49 years. For people aged 70 and over CVD risk will be underestimated because it is based on age 69 years. However, measurement of cardiovascular risk factors is still necessary and in younger (< 40 years) and older (> 70 years) people the physician needs to use both the chart and clinical judgement in making a decision about drug management of blood pressure, lipids, and antithrombotic therapy.
-
Sex—There are separate charts for men and women.
-
Lifetime smoking habit—An assessment of life time tobacco exposure is required. Classifying people solely on the basis of their current habit into cigarette smokers and non-smokers (which includes ex-smokers) is not sufficiently precise. A current cigarette smoker may have less lifetime exposure to tobacco, and therefore less associated cardiovascular damage, than an ex-smoker. For example, a current smoker who has smoked five cigarettes per day for eight years has a lower tobacco exposure than an ex-smoker who smoked 40 cigarettes per day for 20 years until six years ago. Their total exposure is 2 pack years versus 40 pack years, respectively. Therefore to classify the latter as a “non-smoker” would underestimate the real CVD risk. For an ex-smoker the real CVD risk will usually lie somewhere between that of a life long non-smoker and a current cigarette smoker. Therefore it is important to use clinical judgement in estimating CVD risk in ex-smokers. A cigarette smoker who has smoked heavily since the age of 16 years and recently quit at the age of 64 years will have a total risk of CVD almost identical to that of a current cigarette smoker. In contrast a person of 64 years who smoked 10 cigarettes a day for 10 years between the ages of 18 and 28 years will have a total risk of CVD much closer to that of a life long non-smoker.
-
Weight (and height for body mass index) and waist circumference—Weight (kg) and waist circumference (cm) should always be measured. Waist circumference is measured midway between the lower rib margin and the iliac crest. From the front apply the tape, measure horizontally on the skin midway between these two points, and measure the circumference. Central obesity is present if the waist circumference is ≥ 102 cm in men and ≥ 88 cm in women. In Asian populations lower values of waist circumference are more appropriate: ≥ 90 cm in men and ≥ 80 cm in women. When available weight and height (m) measurements can be used together to calculate body mass index (BMI): weight (kg)/height (m)2. A BMI of ⩾ 25 kg/m2 is defined as overweight, and ⩾ 30 kg/m2 is defined as obese.
-
Blood pressure—Systolic blood pressure should be measured according to the British Hypertension Society guidelines.1 At the initial assessment to estimate CVD risk blood pressure should be measured twice and the mean systolic pressure used to calculate risk. For people already taking antihypertensive therapy see below.
-
Non-fasting total cholesterol and HDL cholesterol—A non-fasting (random) sample of blood should be drawn for both total and HDL cholesterol measurements. The ratio of this single measure of total cholesterol to HDL cholesterol is used to calculate CVD risk. If an HDL cholesterol result is not available then use the total cholesterol value alone on the same scale by assuming the HDL cholesterol is 1.0. For people already on lipid lowering therapy see below.
-
Glucose—A non-fasting (random) glucose should be measured on the same sample drawn for lipid measurements. If this random glucose value is ⩽ 6.0 mmol/l there is no need to repeat this measurement. If it is ⩾ 6.1 mmol/l but < 7.0 mmol/l this should be repeated fasting. If it is ⩾ 7.0 mmol/l this should either be repeated fasting, or an oral glucose tolerance test (OGTT) performed.
People already on antihypertensive and/or lipid lowering therapies
CVD risk estimation is more complicated for people already on drug treatments for hypertension or dyslipidaemia. This is because the treated risk factor level will be lower than pre-treatment values. Using an “on-treatment” value for, say, blood pressure will underestimate true CVD risk. For example, a man of 49 years, who smokes, has a blood pressure 106/76 mm Hg on antihypertensive therapy, total cholesterol 5.8 mmol/l, HDL cholesterol 0.9 mmol/l, and is not diabetic has a CVD risk of 18%. The pre-treatment blood pressure was 158/98 mm Hg and using this value gives a CVD risk of 27%. Using the risk estimate based on treated blood pressure could lead to a decision not to use lipid lowering therapy, whereas using the pre-treatment blood pressure to estimate risk would result in a statin prescription because the CVD risk is ⩾ 20% and the total cholesterol has not been reduced to target. Therefore, it is important to try and estimate CVD risk retrospectively, by using the pre-treatment value of a risk factor, whenever this can be found in the person’s medical record. If there is no record of the pre-treatment value then as a rule of thumb assume for blood pressure that it was at least 160 mm Hg, and for the total cholesterol to HDL cholesterol ratio assume that it was at least 6. These values will give a pragmatic but conservative retrospective estimate of CVD risk.
Other risk factors
A person’s CVD risk estimation can be further improved by taking account of other CVD risk factors not included in the chart. Those with a family history of premature CVD, especially CHD (men < 55 years and women < 65 years) will have a higher CVD risk than estimated from the chart—approximately 1.3 times higher. Similarly, obese people, and particularly those with central obesity (waist circumference ≥ 102 cm in men and ≥ 88 cm in women in caucasians, and for Asians ≥ 90 cm in men and ≥ 80 cm in women), are at higher risk. In addition to measuring non-fasting total and HDL cholesterol and non-fasting glucose, a fasting blood sample can be taken to measure glucose and triglycerides and to calculate LDL cholesterol. Impaired fasting glycaemia (IFG is defined as fasting plasma glucose ⩾ 6.1 mmol/l and < 7.0 mmol/l on two separate occasions) is associated with increased CVD risk. An OGTT may also reveal impaired glucose tolerance (IGT is defined as two hour plasma glucose ⩾ 7.8 and < 11.1 mmol/l) which is also associated with increased CVD risk. Elevated fasting triglycerides (> 1.7 mmol/l) are also associated with increased CVD risk.
Target organ damage
Where there is evidence of target organ damage (TOD)—retinopathy (hypertensive grade 3 or 4), raised creatinine, micro/macroalbuminuria or proteinuria, or left ventricular hypertrophy (LVH) on ECG or echocardiography—the risk of CVD will be substantially higher than shown by the chart. Therefore people with raised blood pressure who also have evidence of TOD should all be considered high risk and managed accordingly. This is because the true total risk of CVD is most likely to be > 20% over 10 years.
Summary
The first step in assessing a person’s CVD risk is to measure the major cardiovascular risk factors—smoking habit, blood pressure, and non-fasting lipids (total and HDL cholesterol)—and then use the Joint British Societies’ cardiovascular risk prediction chart (or computer program) to estimate total CVD risk according to age and sex. This estimated risk of developing CVD then needs to be subjectively refined by the physician to take account of other historical, clinical, and test results—for example, ethnicity, family history of CVD, obesity and central obesity, raised triglycerides, impaired glucose regulation, evidence of target organ damage, and so on (table 3). The physician can then make an overall clinical judgement about a person’s total CVD risk and the need for drug therapy. A total CVD risk ⩾ 20% over 10 years is considered sufficiently high to justify the use of antihypertensive and lipid lowering therapies, and for some people antiplatelet therapies as well. Assessing total cardiovascular risk in this way is an essential prelude to decisions on all of these drug treatments. People who are found to be at high total CVD risk as defined, or with newly diagnosed impaired glucose regulation or diabetes, will then require further cardiovascular investigations (which might include for example, an OGTT, electrocardiography, echocardiography, and so on) to inform the subsequent management of their cardiovascular risk. People with known diabetes should also have all their cardiovascular risk factors measured (table 3).
Cardiovascular risk assessment in people at high risk of developing CVD and their families
People with atherosclerotic disease should also have all their cardiovascular risk factors measured while taking account of the effects of the acute phase of the disease on blood presure, lipid, and glucose levels (table 4).
Cardiovascular risk assessment in people with atherosclerotic cardiovascular disease and their families
REFERENCE
1
(V) ASSESSMENT AND MANAGEMENT OF RISK FACTORS FOR PEOPLE WITH ESTABLISHED CVD AND PERSONS AT HIGH TOTAL RISK OF DEVELOPING CVD
(A) LIFESTYLE: SMOKING, DIET, ALCOHOL, PHYSICAL ACTIVITY, WEIGHT, AND BODY FAT DISTRIBUTION
Using scientific evidence from both epidemiology and clinical trials, several lifestyle measures which can improve cardiovascular risk factor profiles and reduce the incidence of CV events are recommended—whether in the context of asymptomatic people or those with established CVD (table 5). These general lifestyle changes are suitable for the whole adult population. For people with atherosclerotic disease or diabetes, and those at high total risk of developing CVD, additional risk factor and therapeutic targets are defined (table 6). The involvement of the person’s partner and all family members living in the same household may be helpful in making these lifestyle changes.
Lifestyle targets
Lifestyle, risk factor, and therapeutic targets for cardiovascular disease prevention in all high risk people and families
(i) Smoking
Smoking increases the risk of coronary, cerebral, and peripheral arterial disease and this adverse effect is related to the amount of tobacco smoked daily and the duration of smoking.1–5 The impact of smoking on atherosclerosis progression is greater for individuals with hypertension or diabetes.6 Passive smoking also increases the risk of CHD.7 Stopping smoking can be followed by a rapid decline in the risk of CHD. In people with CHD the risk falls within 2–3 years to the level of those people with CHD who never smoked.5 A meta-analysis of smoking cessation after myocardial infarction showed a relative odds of 0.54 (95% confidence interval (CI) 0.46 to 0.62) for coronary mortality in those who stopped smoking compared to those who continued to smoke.8 In asymptomatic people up to 10 years are needed to reach the risk level of those people who have never smoked.9–12
All cigarette smokers should receive the advice of a physician to stop smoking completely and this advice should be reiterated and reinforced by all health professionals.13,14 A meta-analysis of brief advice versus no advice shows an increase in the odds of quitting for those receiving advice (odds ratio 1.69, 95% CI 1.45 to 1.98), and the more intensive interventions were more effective than minimal ones.13 The advice should include a description of the cardiovascular risks (and other disease risks) of smoking, providing appropriate information on approaches to stopping, assessing readiness to stop, and agreeing a specific plan with a follow up arrangement. Assessing the degree of addiction (for example, Fagerstrom test for nicotine dependence) is also appropriate in guiding the use of nicotine replacement therapies.15 In the initial period of stopping smoking nicotine replacement therapy (for example, chewing gum or transdermal patches) can help. A review of different forms of nicotine replacement therapy showed cessation rates increased by up to twofold with such treatments.16 Nicotine patches have also been tested in people with coronary disease without any adverse effects.15 Antidepressant medications in the form of bupropion and nortriptyline are also helpful in smoking cessation.17 Selective cannabinoid receptor (CB1) blockers and other therapeutic approaches may have a role in the future.
(ii) Diet
There are complex relationships between diets and CVD. The epidemiological evidence started with the Seven Countries Study, which showed that total fat, and specifically saturated fat, are both positively associated in these populations with 25 year coronary mortality.18 At the level of individuals within each population in this international study, saturated fatty acids (SFAs) were also related to coronary mortality. As consumption of saturated fatty acids increases so does LDL cholesterol. A decrease in fat intake results in a decrease in LDL and HDL cholesterol, but the overall effect on lipoproteins depends on which nutrients replace the saturated fat.19 A meta-analysis of randomised controlled trials of reducing saturated fat (using monounsaturated or polyunsaturated fats as replacement) with at least two years follow up has shown a risk reduction for cardiovascular events: 0.76 (95% CI 0.65 to 0.90).20
In epidemiological studies polyunsaturated fatty acids of both n-6 and n-3 classes are inversely related to risk of CHD.21–24 Linoleic acid is the principal fatty acid in the n-6 group and is mainly found in vegetable oils. Alpha-linolenic acid is the precursor of the n-3 group and the main source is certain vegetable oils: soybean, safflower, and linseed oils. A randomised controlled trial of a diet enriched with alpha-linolenic acid in high risk people has shown reductions in coronary and all cause mortality.25 Eicosapentaenoic acid (EPA) and docosahexaenoic (DHA) of the n-3 class are principally obtained from fish and some vegetable oils—for example, soybean oil.
Plant stenols or sterols that have been esterified to increase their lipid solubility can be incorporated into food, and will reduce the absorption of cholesterol from the gut and lower blood cholesterol values. Two grams of plant stenol or sterol added to an average portion of margarine reduces LDL cholesterol by an average of 0.54 mmol/l in middle aged people. A reduction in LDL cholesterol of about 0.5 mmol/l would be expected to reduce the risk of CHD by about 25% over two years.26
Epidemiological studies show regular fish consumers to be at lower risk of fatal CHD, including sudden death.27,28 Randomised controlled trials in people with established coronary disease of increased fish consumption and supplementation with EPA/DHA have shown reductions in coronary and total mortality.29–31 In a systematic review of these trials the risk of all cause mortality was reduced to 0.8 (95% CI 0.7 to 0.9).32
Trans fatty acids are usually derived from industrial hydrogenation of monounsaturated or polyunsaturated fats and in some epidemiological studies dietary intake is positively related to the risk of CVD.21,33 Dietary cholesterol has relatively little effect on blood lipid values but in metabolic studies there is considerable variation in response between individuals34 and dietary cholesterol intake has been related to the development of CHD in some epidemiological studies.
Fruit and vegetable consumption in a meta-analysis of epidemiological studies is inversely related to risk of CHD35 but, apart from one trial in hypertension,36 there is no other randomised controlled trial evidence. In the DASH (dietary approaches to stop hypertension) trial a diet rich in fruit, vegetables, and low fat diary products with reduced content of both total and saturated fat, reduced blood pressure.36
A reduction of sodium intake, especially in the form of sodium chloride, will also reduce blood pressure37 and is additive to the more comprehensive dietary intervention used in DASH.36,38
Randomised controlled trials of vitamin supplementation (alpha-tocopherol or vitamin E), vitamin C, and beta-carotene (retinol) in coronary, stroke, and others at high cardiovascular risk have shown no benefit on CVD mortality or total mortality.39,40 Beta-carotene alone, or in combination with either alpha-tocopherol or retinol, increased the risk of CV death.41 At present there is no clinical trial evidence to support the use of folate supplements to lower homocysteine in relation to CVD events.42
A professional dietary intervention should be offered to all high risk people. The key elements of a cardiovascular protective diet are shown in table 5.
(iii) Alcohol
Alcohol consumption ranging between 1–3 alcohol units per day (a unit equates to about 80 ml of wine, 250 ml of normal strength beer, and 30–50 ml of spirits) is associated with the lowest all cause mortality.43,44 This is largely due to lower coronary mortality. Optimum consumption is lower for women than men. There is no evidence of any difference in cardiovascular benefit of any one source of alcohol compared with another.45 The pattern of alcohol use also has an effect on cardiovascular risk; binge drinking is associated with a higher risk of sudden death46 and stroke.47,48 There is an increased risk of haemorrhagic stroke, and to a lesser extent ischaemic stroke, above 3 units per day.46 As alcohol consumption increases above 3 units per day so does systolic and diastolic blood pressure, the risk of cardiac arrhythmias, cardiomyopathy, and sudden death.44,46,49,50 Although there is no clinical trial evidence on alcohol consumption and CVD, 1–3 units of alcohol per day may be considered safe.51
(iv) Physical activity
A sedentary lifestyle is associated with an increased risk of CVD.52–66
In asymptomatic people aerobic physical activity and cardiorespiratory fitness are associated, in a dose response fashion, with a significant reduction in cardiovascular and all cause mortality. Physical activity, either at work or in leisure time, is associated with a lower risk of CHD in men and women. The largest reduction in risk is between sedentary and moderately active individuals, with a more modest reduction between moderate and vigorous activity. This cardiovascular benefit is lost when physical activity is discontinued. Physical activity has a beneficial effect on other cardiovascular risk factors.61 It is important in controlling body weight—both in losing weight and preventing weight gain. Physical activity can prevent or delay the development of high blood pressure,67–69 increases HDL cholesterol concentration, and lowers the risk of developing diabetes.
In people with established CHD the most recent meta-analysis of randomised controlled trials of cardiac rehabilitation (either exercise only or a more comprehensive lifestyle intervention which included physical activity) showed a 20% reduction in all cause mortality (0.80, 95% CI 0.68 to 0.93) and a 26% reduction in cardiac mortality, (0.74 95% CI 0.61 to 0.96).70 There were no significant differences in disease outcomes between exercise only and comprehensive rehabilitation, but this comparison may be confounded by those taking exercise changing other aspects of their lifestyle. So an organised programme of cardiovascular prevention and rehabilitation for people with CHD which addresses smoking, diet and physical activity, together with the management of other risk factors, and use of cardioprotective drug therapies, will reduce cardiac mortality and all cause mortality.71,72
(v) Body weight and abdominal fat
As body weight (defined as body mass index (BMI)) increases so does the risk of CVD.73–76 In addition to total adiposity, the distribution of fat, particularly visceral fat,77 increases CVD risk.78 Although there are several markers of abdominal obesity, the waist circumference is the most practical in clinical practice.77 Overweight and abdominal obesity are associated with other risk factors including small and dense atherogenic LDL cholesterol, low HDL cholesterol, raised triglycerides, elevated blood pressure, insulin resistance, and impaired glucose regulation including diabetes.79 This clustering of risk factors, usually found in centrally obese individuals, is commonly referred to as the metabolic syndrome.79 Weight reduction results in a lower blood pressure,80 lower LDL cholesterol and triglycerides, higher HDL cholesterol,81 and an improvement in other elements of the metabolic syndrome such as hyperinsulinaemia and hyperglycaemia.82,83
Weight reduction interventions include dietary modification, increased physical activity, and some drug treatments, all of which are effective over the short term, especially when used together.84 Weight reduction is appropriate for those who are overweight (BMI ≥ 25 kg/m2) and especially the obese (BMI ≥ 30 kg/m2), and for those with increased abdominal fat (waist circumference ≥ 102 cm in men and ≥ 88 cm in women in caucasians). Caloric intake can be most efficiently reduced by reducing the consumption of high energy dense foods, especially saturated fats, refined carbohydrates, and some alcoholic drinks, and for the obese it will be necessary to restrict calories as well. Fat intake should be less than 30% of total energy intake. Foods with a high fat content should be replaced with vegetables, fruit, and cereal products. Increasing physical activity can make an important contribution to weight loss, in preserving a stable weight and in preventing weight gain. A sustained weight loss of around 0.5 kg per week is a realistic objective until target weight is achieved.84 However, most people begin to gain weight a few months after their initial treatment.84 Therefore, successful weight reduction requires sustained personal and family motivation and long term professional support.
Approved anti-obesity medications include: (i) inhibitors of intestinal fat absorption; and (ii) those acting on the central nervous system to suppress appetite, to reduce food intake, to increase satiety, or increase thermogenesis. Obesity guidelines currently recommend drug therapy be considered in obese people (BMI ≥ 30 kg/m2), or a BMI of 27–30 kg/m2 with one or more obesity related disorders.84 Clinical trials of such medications have been of short duration and the impact of these drugs on CVD and total mortality has not been assessed. In a meta-analysis, orlistat, an inhibitor of fat absorption, reduced weight by 2.7 kg (95% CI 2.3 to 3.1 kg) compared to placebo.85 In one trial intensive lifestyle change supplemented with orlistat over four years reduced the progression to diabetes by 39% compared to placebo. Gastrointestinal side effects were the most common side effect. In another meta-analysis sibutramine, a centrally acting drug, reduced weight by 4.3 kg (95% CI 3.6 to 4.9 kg) compared to placebo, but was associated with increases in pulse rate, and systolic and diastolic blood pressure.85 In a separate meta-analysis of sibutramine on blood pressure the overall effect on change in systolic blood pressure was +0.16 mm Hg (95% CI 0.08 to 0.24) and +0.26 mm Hg (95% CI 0.18 to 0.33) for diastolic pressure.86 Weight re-gain is common when all these drug therapies are stopped.
Summary
All high risk people—people with established atherosclerotic disease, people with diabetes, and asymptomatic people at high total risk of developing CVD—should be given professional support to make lifestyle changes to prevent first or recurrent atherosclerotic events. In asymptomatic people without a history of CVD priority should be given to lifestyle (table 5). Indeed, for many people whose total CVD risk is not sufficiently high to justify pharmacotherapy at their present age, lifestyle intervention can be the only approach offered for CVD prevention. However, where the total risk of CVD is sufficiently high to justify more intensive intervention, or when the level of any one risk factor is already associated with target organ damage, lifestyle measures alone are usually not sufficient and drugs will be required to achieve targets (table 6).
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
(B) BLOOD PRESSURE AND HYPERTENSION
Epidemiology and clinical trial evidence
As blood pressure increases so does the risk of stroke, CHD, and heart failure.1–4 Elevated blood pressure is also associated with an accelerated rate of decline of cognitive and renal function.5–7 The epidemiological relationship between systolic and diastolic blood pressure and the risk of developing CVD is continuous whereas the definition of hypertension is based on the benefits of blood pressure lowering in clinical trials. A recent meta-analysis suggests that the relationship between systolic and/or diastolic blood pressure and cardiovascular risk is steeper than previously recognised.1 Although the relationship between blood pressure and cardiovascular risk is continuous, blood pressure thresholds for intervention with drug therapy and recommended blood pressure treatment targets are set pragmatically to guide clinical practice. Lower intervention thresholds and lower optimal treatment targets are set for people at higher total CVD risk.8,9
The CVD risk associated with elevated blood pressure is determined by both the level of blood pressure and the presence of other risk factors for atherosclerotic disease.8,9 Therefore, total CVD risk management is emphasised in order to maximise CVD risk reduction, of which lowering blood pressure is one important component.8,9 Data from many randomised clinical trials provide compelling evidence of the effectiveness of antihypertensive therapy at reducing the risk of CVD. A reduction in blood pressure by an average of 12/6 mm Hg can be expected to reduce stroke by 40% and CHD by 20%.10 The absolute risk reduction will be greatest in those at highest risk. In the elderly up to 80 years the benefits of drug treatment for hypertension, including isolated systolic hypertension, have been clearly demonstrated.11–16 Cognitive impairment associated with increasing age may also be reduced by blood pressure treatment, an important consideration in this age group.6,17 In people over the age of 80 years a recent meta-analysis concluded that blood pressure treatment reduced stroke and CHD events (both fatal and non-fatal) but with no discernible effect (although statistical power was inadequate) on overall mortality.18 A study of the treatment of hypertension in the very elderly is ongoing and will better inform treatment decisions for this age group.19
Meta-analyses and systematic reviews have consistently demonstrated that no one class of blood pressure lowering drug is any more effective than another at preventing CHD in people with treated hypertension—the benefit of treatment in preventing CHD being driven by the quality of blood pressure control.10,20–24 There has been recent controversy about the effectiveness of angiotensin receptor blockers (ARBs) at reducing the risk of CHD in people with hypertension.25 In studies in which ARBs have achieved similar blood pressure control to comparator drugs,26 the rates of CHD with ARB based therapy have not differed significantly from those observed with the comparator drugs. In studies in which blood pressure control has been less effective than the comparator with ARB based therapy,27 the rates of CHD have been higher with ARB based therapy. These observations confirm the importance of blood pressure control in the prevention of CHD and do not suggest any specific advantage or disadvantage of ARBs in preventing CHD relative to other classes of drug therapy, at equivalent levels of blood pressure control.
Definition of hypertension
The results of clinical trials have determined the pragmatic definition of hypertension: “the level of blood pressure at which there is evidence that blood pressure reduction does more good (in terms of reducing CVD risk) than harm”. Hypertension based on clinical blood pressure readings is defined in adults (aged ⩾ 18 years) as a systolic blood pressure ⩾ 140 mm Hg and/or a diastolic blood pressure ⩾ 90 mm Hg. Grades of hypertension are defined in table 7. “High-normal” blood pressure is defined as systolic blood pressure 135–139 mm Hg and/or diastolic blood pressure 85–89 mm Hg.8
Grades of hypertension
It is important to note that ambulatory blood pressure monitoring (ABPM) or home blood pressure readings are usually lower than clinic readings, and therefore thresholds and targets should be adjusted downwards (for example, by 10/5 mm Hg).8 Ambulant, normotensive individuals usually have an average day time blood pressure of < 135/85 mm Hg and average nocturnal blood pressure of < 120/70 mm Hg. Average daytime ABPM pressures > 135/85 mm Hg, or 24 hour values > 125/80 mm Hg, can be considered hypertensive.28 For self measurement of blood pressure, levels ⩾ 135/85 mm Hg should be considered to be in the hypertensive range.29
Measurements should be made under standardised conditions using accurate, validated, and well maintained monitors with an appropriate cuff size.8 Further information on blood pressure monitoring and validated automated devices is available at www.bhsoc.org.
Blood pressure assessment
All adults from 40 years onwards should have their blood pressure measured as part of an opportunistic CVD risk assessment in primary care. For asymptomatic individuals with no history of CVD or diabetes, this blood pressure measurement should be viewed in the context of total CVD risk based on the Joint British Societies’ cardiovascular risk prediction chart. For people already on antihypertensive drug therapy at the time CVD risk is first estimated, the blood pressure level before drug treatment was started should always be used to estimate risk, not the blood pressure level on treatment. If this measurement is not available assume the pre-treatment systolic blood pressure was at least 160 mm Hg for the purposes of estimating total CVD risk. Those who are not found at this cardiovascular risk assessment to be at high total CVD risk, and are not started for other reasons on drug therapy to lower blood pressure, lipids or glucose, should have their blood pressure and risk assessment repeated, ideally within five years.
For people with established atherosclerotic disease or diabetes the blood pressure level should be viewed in relation to the target blood pressure for this group. The assessment of blood pressure in those with acute myocardial infarction/ischaemia and other acute vascular diseases such as stroke is addressed below.
The British Hypertension Society recommendations (www.bhsoc.org) for measuring blood pressure should be followed (box 1).8 Seated blood pressure recordings are generally sufficient, but standing blood pressure should be measured in elderly or diabetic people to exclude orthostatic hypotension. The average of two readings at each of several visits should be used to guide the decision to treat.
Box 1: Blood pressure measurement by standard mercury sphygmomanometer or semiautomated device
-
Use a properly maintained, calibrated, and validated device
-
Measure sitting blood pressure routinely: standing blood pressure should be recorded in elderly and diabetic people
-
Remove tight clothing, support arm at heart level, ensure hand relaxed, and avoid talking during the measurement procedure
-
Use cuff of appropriate size
-
Lower mercury column slowly (2 mm/s)
-
Read blood pressure to the nearest 2 mm Hg
-
Measure diastolic as disappearance of sounds (phase V)
-
Take the mean of at least two readings; more recordings are needed if notable differences between initial measurements are found
-
Do not treat on the basis of an isolated reading
For full details of methods, download references from www.bhsoc.org
The blood pressure of almost 50% of individuals initially categorised as mildly hypertensive subsequently falls into the normal range and stabilises in the first 3–4 months of observation. The period of observation is dependent on severity. In mild (stage 1) uncomplicated hypertension, at least four pairs of measurements should be repeated over a period of 3–6 months. However, in people with CVD, target organ damage, or more severe hypertension, antihypertensive drugs should be initiated after weeks rather than months of observation.8
The evaluation of blood pressure levels in older people can be more difficult. Older people show greater blood pressure variability and it is important that multiple measurements are taken on several occasions. Sitting and standing values should be taken to assess postural blood pressure changes in view of the high prevalence of orthostatic hypotension in this age group. Standing blood pressure levels may have to be used as a basis for initiating and assessing response to treatment in those with a significant (systolic blood pressure ⩾ 20 mm Hg) postural fall or who develop postural symptoms.
Blood pressure thresholds for intervention with drug therapy
All people with a persistent blood pressure ⩾ 140/90 mm Hg, high-normal blood pressures (135–139/85–89 mm Hg), or a family history of hypertension should receive lifestyle advice to help reduce their blood pressure and CVD risk.8 Lifestyle changes can reduce blood pressure and obviate the need for drug therapy in people with mild hypertension, or reduce the number of drugs required to control blood pressure in people with treated hypertension.8,30 Lifestyle advice should continue even when drug therapy is initiated.
Blood pressure thresholds for intervention with drug therapy are outlined in fig 3. People with persistent blood pressure elevation ⩾ 160 mm Hg systolic and/or ⩾ 100 mm Hg diastolic are at sufficiently high CVD risk on the basis of blood pressure levels alone to require drug therapy to reduce their blood pressure. People with sustained systolic blood pressures ⩾ 140 but < 160 mm Hg systolic and/or diastolic blood pressures ⩾ 90 but <100 mm Hg and clinical evidence of CVD or diabetes or target organ damage (see box 2) or a total CVD risk ⩾ 20% should be considered for blood pressure lowering drug therapy.8,30 People with these blood pressure levels (grade 1 hypertension) but without CVD, diabetes, target organ damage, and a total CVD risk < 20% should continue with lifestyle strategies and have their blood pressure and total CVD risk reassessed annually.8,30

Risk thresholds and targets for blood pressure in asymptomatic people without CVD
Box 2: Target organ damage
-
Heart failure
-
Established coronary heart disease
-
Stroke or transient ischaemic attack (TIA)
-
Peripheral arterial disease
-
Abnormal renal function (elevated serum creatinine or proteinuria/microalbuminuria)
-
Hypertensive or diabetic retinopathy
-
Left ventricular hypertrophy on ECG or echocardiography
Some people at very high cardiovascular risk—for example, following a myocardial infarction, stroke or TIA, or people with established chronic renal disease or those with diabetes and complications may benefit from blood pressure lowering at lower levels of pressure—that is, an intervention threshold of systolic > 130 mm Hg and/or diastolic > 80 mm Hg.8,20
We recommend that those who reach 80 years of age while on treatment should remain on therapy, especially if there is evidence of cardiovascular disease, target organ damage, or they have other cardiovascular risk factors such as diabetes.8 For those aged over 80 years at the time of diagnosis of hypertension, treatment decisions should balance potential benefits of such treatment in the context of other co-morbidities.
Blood pressure treatment targets
The benefits of blood pressure reduction are primarily driven by the degree of blood pressure control. Systolic blood pressure is generally more difficult to control than diastolic blood pressure. Recommended treatment targets are shown in table 8. Optimal blood pressure control is defined as < 140/85 mm Hg.8 This will be difficult to achieve for some people, especially for systolic blood pressure, and combinations of drugs are invariably required (see below). For people with established CVD, diabetes, or chronic renal disease, a lower blood pressure target of < 130/80 mm Hg is recommended but this level of blood pressure control can be difficult to achieve.8
Optimal and audit standard blood pressure (BP) targets
We recommend that practitioners adopt an “audit standard” of < 150/90 mm Hg as a minimum for all treated hypertensives (< 140/80 mmHg for those at higher risk), and thereafter aiming for optimal targets if possible.8 This audit standard of < 150/90 mm Hg is identical to that recommended in the General Medical Services contract.
Selection of drug therapy
Many randomised controlled clinical trials are consistent in showing that blood pressure lowering based on various classes of drug therapy is effective at reducing the complications of elevated blood pressure and reducing cardiovascular morbidity and mortality.10,21,22,30 In addition to longstanding evidence with diuretics and β blockers, recent studies have also confirmed the safety and effectiveness of angiotensin converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), and calcium channel blockers (CCBs) for the treatment of blood pressure.13–17,23,26,27,31–42 Recent meta-analyses and overviews of the major outcome trials of the treatment of hypertension have consistently concluded that the main driver of benefit from antihypertensive therapy is blood pressure lowering and that in general the various drug classes are about as effective as each other at reducing cardiovascular morbidity and mortality per unit fall in blood pressure.10,20–22,24,30 There are, however, some important caveats to this statement with regard to heterogeneity in response to different drug classes, optimal drug combinations, and specific categories of hypertension that are considered in more detail below. In general, once daily preparations that provide full 24 hour blood pressure control are preferred.
Combinations of drug therapy to optimise blood pressure control
In clinical trials of blood pressure lowering drugs, most people have received two and in many cases three or more blood pressure lowering drugs in an endeavour to achieve recommended blood pressure targets. This evidence base contrasts sharply with practice in the UK where, until recently, almost two thirds of treated hypertensive people receive monotherapy and less than 10% receive more than two drugs.43 This is reflected in the fact that less than half of treated hypertensive people across the UK have their blood pressure optimally controlled. There is an urgent need to increase recognition that monotherapy is usually insufficient therapy for hypertension and that for most people with high blood pressure, combinations of blood pressure lowering drugs will be required. In order to address this important issue, the British Hypertension Society in its most recent guideline suggested the AB/CD treatment algorithm (fig 4) to advise and assist practitioners on logical sequencing and combinations of drug therapy for the treatment of hypertension.8,44 This algorithm is currently being re-evaluated given recent trial evidence comparing drug regimens.45

Recommendations for combining blood pressure drugs/ABCD rule.
The British Hypertension Society AB/CD algorithm
The AB/CD algorithm is designed to improve blood pressure control (fig 4).8,44 It incorporates all classes of antihypertensive drugs. Although not specifically validated by a clinical trial, the recommended drug combinations and sequencing are similar to those used in many clinical trials of blood pressure lowering drugs. The theory underpinning the AB/CD algorithm is that hypertension can be broadly classified as “high renin” or “low renin” and is therefore best treated initially with one of two categories of antihypertensive drug: those that inhibit the renin–angiotensin system (ACE inhibitors or ARBs (A) or β blockers (B)), and those that do not (CCBs (C) or thiazide/thiazide-like diuretics (D)). People who are younger—that is, aged under 55 years—and white tend to have higher renin concentrations than older people—that is, aged 55 years or older or the black population (of African descent).44 A or B drugs are therefore generally more effective as initial blood pressure lowering treatment in younger white patients than C or D drugs. However C or D drugs are more effective first line agents for older white people or black people of any age.44 When there are no compelling indications for treatment with a specific class of drug, then the least expensive drugs should be used.
The AB/CD algorithm has four steps. Step 1 is a single drug: A or B or C or D, depending on age and ethnic group, titrated up to the highest recommended dose if tolerated. When the first drug is well tolerated but the response is small and insufficient, substitution of an alternative drug is appropriate if hypertension is mild (that is, grade 1) and uncomplicated. In more severe or complicated hypertension it is safer to add drugs stepwise until blood pressure is controlled. Treatment can be stepped down later if blood pressure falls substantially below the target level. Step 2 involves combining A or B with C or D. All four of the possible permutations of (A or B) + (C or D) have been approved by the regulatory authorities as fixed dose combinations, although B+D is currently under review (see below). When these drug combinations are required, and when there is no cost disadvantage, then such fixed dose combinations are recommended to improve compliance with therapy. Step 3 usually combines A with C and D. This triple therapy combination has been used in many of the clinical outcome trials and can be achieved by using only two tablets if fixed dose combinations are used—for example, AD + C. Step 4 involves the addition of an α blocker, or additional diuretic—for example, low dose (25 mg once daily) spironolactone.8,44
In the AB/CD algorithm, B (β blockers) is bracketed. This is because several trials, including the largest randomised comparison of β blocker/thiazide against CCB/ACE in primary prevention of CVD (ASCOT-BPLA), have all revealed an increased risk of developing diabetes in people treated with β blockers, especially when combined with thiazide/thiazide-like diuretics.26,45 In comparison to alternative drug combinations which avoid β blockers, the excess risk of diabetes associated with the combined use of a β blocker and thiazide/thiazide-like diuretic ranges from 20–30%. In ASCOT-BPLA the incidence of new diabetes was 1.6 per 100 patient years in the β blocker/thiazide arm compared to 1.1 per 100 patient years in the CCB/ACE arm; an excess risk of 30% of developing diabetes.45 As diabetes further increases the risk of CVD it is advisable to limit the dose of β blockers and not to combine this class with a diuretic, particularly in people at high risk of developing diabetes: (1) strong family history of diabetes; (2) obesity; (3) impaired glucose regulation and/or features of the metabolic syndrome; (4) specific ethnic groups at higher risk of developing diabetes—for example, Asians and those of African origin.8,30
For each major class of antihypertensive drug, there are compelling and possible indications for use in specific groups, and also cautions, and compelling contraindications (table 9). When none of the special considerations listed in table 9 apply, initial drug selection should follow step 1 of the AB/CD algorithm (fig 4). When there are compelling indications for a specific drug class, the AB/CD algorithm can still be used to identify optimal drug combinations with the caveat that the “drug with compelling indications” should be part of the treatment regimen, and one with “compelling contraindications” should not.
Compelling and possible indications, contraindications, and cautions for the major classes of antihypertensive drugs
Blood pressure and people with CHD
In people with raised blood pressure and symptomatic angina, a β blocker is the preferred treatment choice. In recent studies CCBs have also been shown to be effective at reducing the risk of myocardial infarction, symptoms of angina, and hospitalisation due to angina.40,46
In people with established CVD, or at high CVD risk, studies comparing ACE inhibitors with placebo based treatment and usual care showed improved outcomes with ACE inhibitor treatment.33–35 However, there has been controversy as to how much of this benefit, if any, is attributable to ACE inhibition and how much is attributable to the better blood pressure control in the ACE inhibitor treated patients.24 Recent studies in which ACE inhibition has been compared to active blood pressure lowering drugs, rather than placebo, have failed to demonstrate an advantage of ACE inhibition per se.32,39,46 Moreover, a recent study in people with CHD showed no advantage of ACE inhibition versus placebo in people who were also receiving effective CVD risk reduction with additional therapies such as statins and aspirin.47 The message from these recent studies in people with CHD (but without left ventricular dysfunction), on a background of improved CVD risk reduction strategies, is that there is no special benefit of ACE inhibition, beyond that which can be attributable to blood pressure lowering.
Blood pressure in people with cerebrovascular disease
About 80% of all strokes in the UK are due to cerebral infarction from large and small (lacunar) vessel disease as well as cardioembolic sources. Ten per cent of strokes result from cerebral haemorrhage and the rest are related to subarachnoid haemorrhage and “stroke of unknown causes”.48 Overall 20% of people die within the first few months of a stroke, and up to 35% will be dependent at one year.49 Although the majority of these early deaths are directly related to the initial event, mortality after one year is increasingly due to other CVD disease rather than stroke recurrence.34,50 Hypertension remains the most important treatable risk factor for the prevention of stroke and its recurrence, and antihypertensive therapy significantly reduces the risk.34,51
Half of all people with stroke will have a prior history of hypertension and up to 40% will be on antihypertensive treatment when their stroke occurs.51 After acute cerebral haemorrhage or infarction casual blood pressure levels are increased and often labile, with more than 80% of people having levels ⩾ 160/95 mm Hg within the first 48 hours of the event. These values decrease spontaneously in the subsequent 10–14 days, the falls being most pronounced in those who continue their antihypertensive drugs.51,52 This initial increase in BP after stroke may in part be simply due to the stress of hospitalisation, but other mechanisms also appear to be responsible.52,53 Observational studies reporting post-stroke outcome in relation to initial casual blood pressure levels are inconsistent,52–55 though studies using 24 hour blood pressure recordings have shown higher blood pressure levels to be associated with an adverse outcome.56 There is no evidence that drug therapy to reduce blood pressure in the immediate post-stroke period is of benefit, except perhaps at very high levels.57 Whether antihypertensive treatment should be continued or stopped immediately post-stroke is also unclear and there are clinical trials in progress to answer these important questions.58,59 At present it is therefore not possible to provide clear guidance on the clinical management of blood pressure in the immediate (< 48 hours) post-stroke period. It has been suggested that treatment to lower BP is appropriate when BP is persistently elevated immediately post-stroke (systolic blood pressure > 220 mm Hg or mean arterial pressure > 130 mm Hg), although there are no clinical trial outcome data to support this view.60 Others with stroke for whom immediate blood pressure reduction may be beneficial include those with cerebral haemorrhage, and also those with cardiac and vascular emergencies such as hypertensive encephalopathy, aortic or carotid dissection.
Almost half of all stroke survivors will have a raised blood pressure 1–6 months after stroke onset; most observational studies have shown that increasing blood pressure levels at this stage are associated with an increased risk of stroke recurrence and the subsequent development of CHD events.61
The benefits of blood pressure lowering in reducing major cardiovascular events following a stroke or TIA outside the acute post-stroke period are apparent, even in people whose blood pressure has been considered “normal”—that is, < 140/90 mm Hg.6,34,61,62 Recent studies and a previous meta-analysis have shown that blood pressure lowering significantly reduces the odds ratio by approximately 25% for both fatal and non-fatal stroke recurrence and for all major cardiovascular events.34,53 Consequently, such patients would benefit from blood pressure lowering, aiming for a treated blood pressure of < 130/80 mm Hg.8 Other cardiovascular risk factors must also be assessed and managed appropriately. People with an ischaemic stroke or TIA should receive a statin and low dose aspirin (75–150 mg/day) unless contraindicated.8
Other groups with hypertension
Specific issues relating to hypertension management in particular hypertensive groups, including younger people, ethnic minorities, and those with renal disease, are addressed in the British Hypertension Society guidelines.8
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
(C) BLOOD LIPIDS AND DYSLIPIDAEMIA
Epidemiology and clinical trial evidence
As concentrations of blood total cholesterol (and LDL cholesterol) increase so does the risk of CVD.1–4 The relation between blood cholesterol and cardiovascular risk is continuous. In the context of lipids, cardiovascular risk is principally determined by the concentrations of LDL cholesterol, and of HDL cholesterol (inversely), and to a lesser extent by the concentration of triglycerides. While the cholesterol to HDL cholesterol ratio is an appropriate measure for risk assessment, the preferred target for lipid lowering is LDL cholesterol. However, lipoproteins are only one part of cardiovascular risk, which is determined overall by the presence of other risk factors. As the concentration of blood cholesterol increases so can the prevalence of these other risk factors which, taken together, determine overall CVD risk. Therefore, total cardiovascular risk management is emphasised in order to maximise CV risk reduction, of which modifying lipids is one essential component.
The relations between total cholesterol, LDL cholesterol, and HDL cholesterol and the relative risk of CVD are similar in people with and without CVD.1–4 Blood cholesterol and HDL cholesterol continue to be risk factors for recurrent CHD events after myocardial infarction. Therefore, the effects of cholesterol lowering in people with established atherosclerotic disease, and asymptomatic individuals at high risk of developing CVD, is largely explicable in terms of their total risk rather than therapeutic responsiveness induced by clinically overt CHD. People with existing cardiovascular disease tend to have higher overall total risks than those without CVD, but the relative benefits of cholesterol lowering are similar. In other words the absolute benefit of cholesterol reduction is a function of total baseline cardiovascular risk.
The lowering of cholesterol, whether by diet, drugs, or other means, decreases CVD risk.5–13 A meta-analysis of 28 early pre-statin randomised controlled trials of cholesterol lowering showed that a 10% reduction in plasma cholesterol resulted in a 25% reduction in incidence of CHD after five years.5
In a systematic review and meta-analysis quantifying the effect of cholesterol lowering on CHD and stroke, 58 randomised trials of cholesterol lowering by any means were included.14 Reduction in coronary death and non-fatal myocardial infarction for a 1.0 mmol/l decrease in LDL cholesterol was 11% (95% CI 4% to 18%) in the first year, 24% (95% CI 17% to 30%) in the second, 33% (95% CI 28% to 37%) in the third to fifth, and 36% (95% CI 26% to 45%) in the sixth and subsequent year. After standardisation for reduction in LDL cholesterol and duration of treatment, risk reduction was similar for fatal and non-fatal events, for different methods of reducing cholesterol by diet or drugs, and for people with and without known CHD on entry. In the same meta-analysis the reduction in LDL cholesterol and duration of treatment was related to the reduction in CHD. With a reduction in LDL cholesterol of around 1.6 mmol/l, the reduction in CHD events after two or more years of treatment was 51%. So the greater the reduction in LDL cholesterol, and the longer the duration of treatment, the greater was the reduction in CHD events.
The most compelling evidence for cholesterol lowering comes from trials using statins with non-fatal and fatal clinical events as end points.12–39 The early major statin trials in people with established CVD using simvastatin and pravastatin (4S,15,21 CARE,22 LIPID16,23) and in asymptomatic individuals at risk of developing CVD using pravastatin and lovastatin (WOSCOPS,24 AFCAPS/TEXCAPS25) have shown significant reductions in coronary events and coronary mortality and, where statistical power was sufficient, in all cause mortality. A meta-analysis of these five trials showed significant reductions in major coronary events by 31% (95% CI 26% to 36%), coronary mortality by 29% (95% CI 20% to 36%), and all cause mortality by 21% (95% CI 14% to 28%). There was no difference in non-CVD mortality.20 The more recent statin randomised clinical trials with atorvastatin (GREACE,26 ASCOT,27 CARDS,28 PROVE-IT,29 TNT,30,31 IDEAL,32 4D33), fluvastatin (LIPS,34 ALERT35), pravastatin (ALLHAT,36 PROSPER,37 PROVE-IT29), and simvastatin (HPS,38 A-to-Z,39 IDEAL32) have extended the evidence base for this drug class into many populations, including women, the elderly, acute coronary disease, people with diabetes, in renal transplantation (ALERT35), but not in haemodialysis (4D33), and importantly in populations previously considered to have low total cholesterol and LDL cholesterol values. The Heart Protection Study (HPS)38 randomised people with total cholesterol > 3.5 mmol/l and showed convincing evidence of benefit.
In the recent Cholesterol Trialists’ Collaboration, a meta-analysis of data from 90 056 participants in 14 randomised trials of statins, has shown that statin therapy can safely reduce the five year incidence of major coronary events, coronary revascularisation, and stroke by about one fifth per mmol/l reduction in LDL cholesterol.40 There was a 12% proportional reduction in all cause mortality per mmol/l reduction in LDL cholesterol (rate ratio 0.88, 95% CI 0.84 to 0.91). This reflected a 19% reduction in coronary mortality (0.81, 95% CI 0.76 to 0.85) and non-significant reductions in non-coronary vascular mortality and non-vascular mortality. There were reductions in myocardial infarction or coronary death (0.77, 95% CI 0.74 to 0.80), in the need for coronary revascularisation (0.76, 95% CI 0.73 to 0.80), in fatal or non-fatal stroke (0.83, 95% CI 0.78 to 0.88) and, combining these, of 21% in any such major vascular event (0.79, 95% CI 0.77 to 0.81). The reduction in cardiovascular events per mmol/l reduction in LDL cholesterol was largely independent of the presenting LDL level or other characteristics.
A similar proportionate reduction in risk is seen for all people with atherosclerotic disease, regardless of the vascular territory. Women have a similar proportionate reduction in risk to men, and people with diabetes without CVD also have the same proportionate reduction in risk as other groups. There is no age at which these benefits have not been shown, with older people, who are at higher absolute risk, having similar relative reductions in risk as younger people. The absolute benefit of statin therapy is related chiefly to an individual’s absolute risk of such events and to the absolute reduction in LDL cholesterol achieved.
A meta-analysis41 of 53 trials (16 802 subjects) using fibrates (but excluding the WHO Clofibrate Trial) and 30 trials (4749 subjects) using nicotinic acid reported a 25% (95% CI 10% to 38%) reduction in the risk of major coronary events for fibrates (principally the VA-HIT study42 and Helsinki Heart Study43), and for nicotinic acid a 27% reduction (based on only one study, the Coronary Drug Project) for the same end points. However, there was no reduction in total mortality. The largest study of fibrates to date, the FIELD trial44 of 9795 people with type 2 diabetes mellitus, showed that fenofibrate reduced the risk of a coronary event by 11% (hazard ratio 0.89, 95% CI 0.75 to 1.05), which was not statistically significant. In this combined end point there was a 24% reduction in non-fatal myocardial infarction (0.76, 95% CI 0.62 to 0.94) and a non-significant increase in CHD mortality. Total CVD events including revascularisation were significantly reduced by 11% (0.89, 95% CI 0.80 to 0.99). There was no difference in total mortality. So the place of fibrates in people with type 2 diabetes has not been firmly established by this trial. The results of the ACCORD trial in diabetes, which is comparing a statin with and without a fibrate, will be available in 2010.
Comparing earlier trials of statins, and other treatment modalities (such as bile acid sequestrant resins (LRC-CPPT)45 and ileal bypass46), with more recent statin trials it appears that the benefit of absolute LDL reduction is present across a wide range of baseline LDL cholesterol values. This is illustrated by the statin trials in fig 5 which shows the achieved reduction in major cardiac events plotted against the achieved fall in LDL cholesterol (the mean LDL difference between the placebo and active groups) for the major LDL cholesterol lowering trials. As quantified in the meta-analyses described above this illustrates the approximate linear relationship, with greater CVD risk reductions for greater LDL reductions, from baseline LDL values up to 5.0 mmol/l to achieved LDL cholesterol values below 2.0 mmol/l. These observations are not just true for the statin trials but also trials using dietary modification, anion exchange resins, or indeed surgery (ileal bypass). The relation is present whether individuals had either established CVD or were at high risk of developing CVD, or whether they had initially higher or lower LDL cholesterol values. The baseline LDL cholesterol values in the more recent statin trials were around 3 mmol/l and fell with treatment to 2 mmol/l and below.
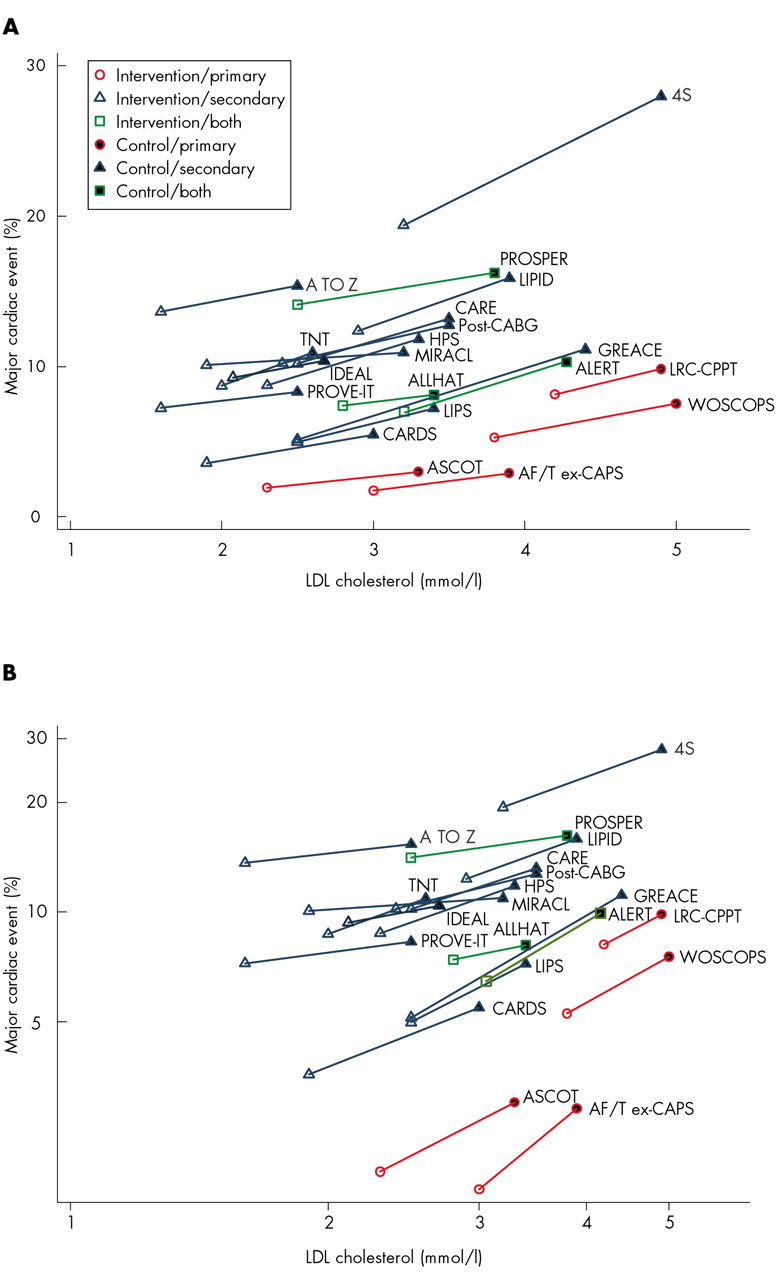
(A) Absolute reduction in LDL cholesterol (mmol/l) and absolute reduction in risk of major cardiac event (MCE). (B) Both axes are on a log scale showing relative reduction in LDL cholesterol (mmol/l) and relative reduction in risk of MCE.
Statins and stroke
The relation between cholesterol and stroke in epidemiological studies is less clear than that for CHD. Meta-analyses of observational studies have either not shown any relation with all strokes combined, or have reported a positive relation with ischaemic stroke and an inverse relation with haemorrhagic stroke.47,48 The effects of lipid lowering therapy on the incidence and recurrence of stroke has been uncertain in individual trials with some showing benefit and others not, but an early meta-analysis of statin trials reported significant reductions in stroke events of about 15–30%.49 In a more recent systematic review and meta-analysis of 58 trials of cholesterol reduction by any means there was a 20% (95% CI 14% to 26%) reduction in risk of all stroke, which was largely due to a reduction in thromboembolic stroke.14
The more recent placebo controlled statin trials which specified stroke as an end point, including the trial with the largest number of people with stroke at entry and subsequent stroke events (HPS), have demonstrated a substantial reduction in ischaemic stroke. In HPS there were 1080 strokes during follow up and there was a 25% relative reduction in the incidence of strokes of any type (95% CI 0.66 to 0.85) in the statin arm (absolute rate 4.3% compared to 5.7% in placebo), which compares with a reduction in CHD events of 27% (95% CI 0.67 to 0.79). The reduction in non-fatal mild-moderate strokes was also significant (odds ratio 0.70, 95% CI 0.60 to 0.82) alone.50 This treatment effect was seen in both people with prior myocardial infarction or other CHD, and in those with no prior CHD. It was largely due to a reduction in the incidence of strokes attributed to ischaemia. Importantly, there was no difference in this trial between statin and placebo in the frequency of haemorrhagic stroke. In addition, there was a significant reduction in the number of episodes of transient cerebral ischaemia.
In the MIRACL trial stroke was a predefined secondary end point and, despite the short 16 week follow up, there was a 50% relative reduction in fatal and non-fatal stroke (95% CI 0.26 to 0.99), and this was also significant for non-fatal stroke alone (odds ratio 0.41, 95% CI 0.20 to 0.87).51 In the PROSPER trial stroke was part of a composite primary end point and based on a total of 266 non-fatal and fatal strokes there was no difference for stroke risk alone, but a favourable trend for TIAs.37 In the ASCOT-LLA trial the pre-specified secondary end point was the combination of fatal and non-fatal stroke together and, based on 210 events, this was reduced by 27% (95% CI 0.56 to 0.96).27 In the CARDS trial stroke was also a pre-specified secondary end point and, based on 60 events, this was reduced by 48% (95% CI 0.31 to 0.89).28 In the ALERT trial of renal transplant recipients combined cerebrovascular events was a predefined secondary end point, but there was no evidence of any treatment effect (odds ratio 1.16, 95% CI 0.83 to 1.63).35 In the LIPS trial stroke was not a pre-specified end point and no data on stroke were reported.34
A meta-analysis of statin trials, including HPS, showed that for an average reduction of about 1.0 mmol/l in LDL cholesterol there was a 21% reduction in stroke risk (95% CI 0.73 to 0.85).52 The Cholesterol Trialists’ Collaboration reported a 17% proportional reduction in the incidence of first stroke of any type (rate ratio 0.83, 95% CI 0.78 to 0.88) per mmol/l lower LDL cholesterol. This was due to a 19% reduction in ischaemic strokes (0.81, 95% CI 0.74 to 0.89) and no apparent difference in haemorrhagic stroke.40
So the clinical trial evidence for statin therapy in the primary prevention of stroke is now compelling and this applies to people with established CVD, those with hypertension, diabetes, and others who are at high total risk of developing CVD. For those who have already had a stroke there is currently no evidence that a statin will reduce the risk of recurrent stroke. In HPS there were 3280 people with stroke at entry and there was no apparent reduction in the risk of recurrent stroke. However, there was a 20% (95% CI −8% to −29%) reduction among the stroke population for any major vascular event.50 This risk reduction was similar in those people with stroke, whether or not also having CHD at entry. So the clinical trial evidence for statin therapy following the development of stroke supports the use of statins to reduce the risk of further major vascular events, but not at the present time for recurrent stroke.53
Lipid assessment
All adults from 40 years onwards should have their total cholesterol and HDL cholesterol measured as part of an opportunistic CVD risk assessment in primary care. For asymptomatic individuals with no history of CVD or diabetes the values of total and LDL cholesterol should be viewed in the context of total cardiovascular risk based on the Joint British Societies’ cardiovascular risk prediction chart, and the total and LDL cholesterol targets for this group. For people already on lipid lowering therapy at the time cardiovascular risk is first estimated, the total cholesterol value before diet and drug treatment was started should always be used to estimate risk, not the cholesterol value on treatment. If this measurement is not available assume the pre-treatment total to HDL cholesterol ratio is at least 6 for the purposes of estimating total CVD risk. Those who are not found at this cardiovascular risk assessment to be at high total CVD risk, or started for other reasons on drug therapy to lower blood pressure, lipids or glucose, should have their lipids and risk assessment repeated, ideally within five years.
For people with established atherosclerotic disease, diabetes, and others who are at high total risk of developing CVD (⩾ 20% over 10 years), their lipids should be monitored regularly, and not less than once per year, and the total and LDL cholesterol target values should be achieved for these groups.
The measurement and management of lipids in people with acute myocardial infarction/ischaemia, other acute vascular diseases such as stroke, and following major surgery is addressed below.
Total cholesterol and HDL cholesterol can usually be measured in a non-fasting state. However, all people who are found to be at high risk should then have a full fasting lipid profile (blood should be drawn after at least a 12 hour fast, usually from 10 pm the previous evening) including total cholesterol, triglycerides, HDL cholesterol and, where available, a direct measurement of LDL cholesterol.
When LDL cholesterol cannot be measured directly it can be estimated by calculation (in mmol/l) using the Friedewald formula: LDL cholesterol = total cholesterol − HDL cholesterol − [triglyceride/2.2]. The accuracy of this estimation of LDL cholesterol concentration is a function of the analytical errors of each component lipid measurement. The Friedewald formula should not be used in non-fasting individuals, or if plasma triglyceride values are higher than 4.0 mmol/l, and it is less reliable in people with diabetes. Measuring lipids in the non-fasting state will underestimate LDL cholesterol to the extent that triglycerides are raised.
Lipid analyses should be made in a laboratory participating in the National Quality Control scheme. With newer analytical methods to measure HDL cholesterol directly, HDL cholesterol can be measured even when triglycerides are as high as 10 mmol/l. Plasma triglyceride values are influenced by a number of factors, such as diet, alcohol consumption, and some diseases. Therefore, elevated plasma triglyceride values (> 1.7 mmol/l) on fasting samples signal the need to investigate secondary causes. A fasting profile will identify people with severe hypertriglyceridaemia (> 10 mmol/l), for whom specific therapies may be appropriate.
In asymptomatic individuals with no history of CVD, lipid values should always be measured on several occasions before initiating drug therapy because of biological and laboratory variation. It is practical to start with a non-fasting sample for total blood cholesterol, and HDL cholesterol, in the context of a comprehensive cardiovascular risk assessment. Then, if the person is at high cardiovascular risk, take a fasting sample to measure a full lipoprotein profile. Lifestyle advice should be given and lipids monitored. This allows for the effects of changes in diet and physical activity to be assessed. Secondary causes of elevated lipids should always be investigated before drug treatment is given. These include alcohol abuse, diabetes, renal disease, liver disease, and inadequately treated hypothyroidism.
At the time of an acute coronary syndrome, especially myocardial infarction, total cholesterol, LDL cholesterol, and HDL cholesterol decrease (and triglycerides may rise).54 Other acute vascular diseases, other severe diseases, and major surgery will have similar effects on blood lipids. The depression of total cholesterol following myocardial infarction generally lasts no longer than 6–8 weeks, but can be longer if there is a complicated recovery. However, a lipid measurement as soon as possible, and preferably within 24 hours of the onset of symptoms, will give a reasonable indication of the total cholesterol and HDL cholesterol values before the acute event, although it will usually be an underestimate. Therefore, it is important to measure a full fasting lipoprotein profile about 8–12 weeks following the acute event, although this will normally be after statin treatment has been started. The clinical reasons for this repeat measurement are: (1) to determine whether the person has a familial dyslipidaemia, particularly familial hypercholesterolaemia, and therefore to initiate screening of first degree relatives; (2) to assess whether the person has achieved the total and LDL cholesterol targets; (3) as a guide to possible changes in lipid modification therapy. Secondary causes of elevated lipids, where these have not already been fully investigated during the hospital admission, should be assessed at the same time.
It is common practice to measure baseline creatine phosphokinase (CK) and alanine/aspartate transaminases (ALT or AST) before starting treatment with a statin as some people may have high values that are physiological, not pathological. If creatine kinase (CK) and liver function are normal, routine measurement of these tests subsequently is not indicated unless the person develops symptoms. If they are measured for whatever reason in asymptomatic individuals, a rise in alanine aminotransferase (ALT) (or aspartate aminotransferase (AST)) to three times, and in CK to five times or even 10 times, the upper limit of normal can be acceptable in the context of statin therapy. The rare syndrome of acute myositis, with the very rare possibility of progression to non-fatal or fatal rhabdomyolysis, is considered below. Statins do not significantly alter other parameters of liver function.
Triglycerides, HDL cholesterol, and non-HDL cholesterol
While the main target for lipid management in high risk people is LDL cholesterol, many will have a mixed dyslipidaemia, with elevated triglycerides and low HDL cholesterol. In these people the primary treatment is still to treat LDL cholesterol to target with a statin. This mixed dyslipidaemia represents accumulation of atherogenic triglyceride-rich remnant lipoproteins. The LDL particles are often smaller, denser, and more triglyceride-rich than normal. They are less readily cleared by the normal pathways, are more readily taken up by macrophages in the arterial wall, and for a given LDL cholesterol concentration there are relatively more particles present.
Although there are no lipid targets other than for total and LDL cholesterol, a desirable value for non-HDL cholesterol is < 3 mmol/l. Non-HDL cholesterol (total cholesterol minus HDL cholesterol) represents the total of cholesterol circulating on apoprotein B particles (both LDL and triglyceride-rich lipoproteins). One advantage of using non-HDL cholesterol is that it includes the main atherogenic particles and can be calculated in non-fasting samples. Statins will lower LDL cholesterol and non-HDL cholesterol by about the same amount, as their primary action is on LDL cholesterol with little effect on triglyceride-rich particles.
When estimating CVD risk using the charts, individuals with hypertriglyceridaemia (> 1.7 mmol/l) have a higher CVD risk than that shown in the charts, and it is appropriate to increase that risk by a factor of 1.3.
HDL cholesterol is inversely related to risk of CVD. For this reason the ratio of total cholesterol to HDL cholesterol is used for CVD risk assessment, but there is no treatment target for HDL cholesterol. The reasons for this are as follows. HDL cholesterol is only altered modestly, and not independently of changes in other lipid parameters, in the clinical trials. There are as yet no drugs available which independently alter HDL cholesterol. Statins increase HDL cholesterol by about 3–10%. Fibrates increase HDL cholesterol, and reduce triglycerides, but have only a modest effect on LDL cholesterol. Nicotinic acid also raises HDL cholesterol. Fish oils (n3 fatty acids; DHA/EPA) raise HDL cholesterol and reduce triglycerides.
As triglycerides rise, especially when HDL cholesterol values are low, so does CVD risk. At triglyceride levels above 1.7 mmol/l there are adverse changes in the quality of LDL and HDL molecules. With high triglycerides plasma residence time of triglyceride-rich lipoproteins also rises, so there is increased interchange of triglyceride from chylomicrons and very low density lipoprotein (VLDL) into LDL and HDL, while cholesterol esters travel in the opposite direction, through the action of cholesterol–ester transfer (CETP) protein. The triglyceride enriched LDL is converted to small dense LDL which is cleared less rapidly from the circulation. Studies of CETP inhibitors which raise HDL are being undertaken.
Management of blood lipids
Lipid thresholds for intervention with drug therapy
All people should receive lifestyle advice to modify their lipoproteins favourably (to reduce total and LDL cholesterol, raise HDL cholesterol, and lower triglycerides) and reduce their cardiovascular risk. The indication for intervention with lipid lowering drug therapy is that an individual is “at high risk”: atherosclerotic disease, diabetes (see next paragraph), or at high total risk (CVD risk ⩾ 20% over 10 years).
In people with diabetes mellitus the total risk of developing CVD is a function of age, duration of diabetes, complications of diabetes, and concomitant risk factors. Therefore, we recommend the following indications for statin therapy in diabetes:
-
all those who are aged 40 years or more with either type 1 or 2 diabetes; and
-
for people aged 18–39 years with either type 1 or 2 diabetes and who have at least one of the following:
-
retinopathy (pre-proliferative, proliferative, maculopathy)
-
nephropathy, including persistent microalbuminuria
-
poor glycaemic control (HbA1c > 9%)
-
elevated blood pressure requiring antihypertensive therapy
-
raised total blood cholesterol (⩾ 6.0 mmol/l)
-
features of metabolic syndrome (central obesity and fasting triglyceride > 1.7 mmol/l (non-fasting > 2.0 mmol/l) and/or HDL cholesterol < 1.0 mmol/l in men or < 1.2 mmol/l in women)
-
family history of premature CVD in a first degree relative.
After LDL cholesterol has been treated to target, other lipid parameters (HDL cholesterol, triglycerides and non-HDL cholesterol) should be considered, especially in people with a mixed dyslipidaemia, most commonly seen in the metabolic syndrome and diabetes mellitus. In these people the concentration of atherogenic triglyceride-rich lipoproteins can be estimated from non-HDL cholesterol (total cholesterol minus HDL cholesterol), and a value of < 3.0 mmol/l is desirable. A fibrate, nicotinic acid, or fish oils may all have a role in relation to further modifying HDL cholesterol and triglycerides on specialist advice.
When to start lipid lowering therapy
People with coronary and other atherosclerotic disease
Data on the optimal time to start statin therapy in acute coronary syndromes (ACS) was, until recently, limited to observational studies and post hoc analyses of clinical trials. The traditional approach has been to start with dietary advice and then consider lipid lowering therapy some months after the acute event. The impact of early initiation of statin treatment has now been addressed in three clinical trials—MIRACL,51 A to Z,39 and PROVE-IT29—but MIRACL is the only placebo controlled trial to assess the short term impact of immediate treatment.51 Interpreting the results of the other two trials is potentially confounded by the use of different statins in each of the treatment arms.29,39 In the MIRACL trial, 3086 people with ACS were randomised to a statin or placebo between 24–96 hours after diagnosis. LDL cholesterol was reduced from 3.2 mmol/l to 1.9 mmol/l by 16 weeks. At this time there was a 16% relative reduction in the combined primary end point of fatal and non-fatal coronary events (95% CI 0.70 to 1.0; p = 0.048). This difference was largely due to a reduction in recurrent symptomatic ischaemia requiring hospitalisation.51
In the A to Z trial of 4497 people with ACS an early intensive strategy (high dose statin) was compared with a delayed conservative strategy (placebo for four months followed by the same statin at a lower dose).39 LDL cholesterol was reduced from 2.9 mmol/l to 1.7 mmol/l in the intensive arm compared to a reduction from 2.9 mmol/l to 2.1 mmol/l in the conservative arm. About a third of people discontinued the treatment in both groups. Overall there was no significant difference between the two treatment groups in the first four months for the combined primary end point of fatal and non-fatal cardiovascular events which fell by 11% (95% CI 0.76 to 1.04) in the intensive treatment arm. In a post hoc analysis after the first four months, the primary end point was reduced by 25% (95% CI 0.66 to 0.95) in the intensive arm. In the PROVE-IT trial 4162 people with ACS were randomised at a median of seven days to intensive or standard statin treatment.29 LDL cholesterol was reduced from 2.7 mmol/l to 2.5 mmol/l with standard therapy, and to 1.6 mmol/l in the intensive arm. The combined primary end point of fatal and non-fatal cardiovascular events was reduced by 16% (95% CI 5% to 26%) at two years. The size and direction of this benefit was evident at 30 days and remained consistent across the whole period of the trial.
So the evidence from these three trials supports the view that early in-hospital statin treatment, and subsequent compliance with the drug following discharge from hospital, is of benefit in reducing the risk of further cardiovascular events in the short term; principally, recurrent myocardial infarction requiring hospitalisation.
Therefore, our pragmatic recommendation is that all people with acute atherosclerotic (coronary, cerebral, and peripheral) disease, but not cerebral haemorrhage, should be prescribed a statin in hospital regardless of the initial cholesterol value. The rationale for this policy is as follows. Firstly, the recent trials of early initiation of statin treatment as reviewed above show some evidence of early cardiovascular benefit. Secondly, the vast majority of such people will have a total cholesterol ⩾ 4.0 mmol/l (LDL cholesterol ⩾ 2.0 mmol/l) and therefore most will require a statin to achieve and maintain the lipid targets. Thirdly, measurement of lipids in the acute phase of the disease will usually underestimate the pre-disease values, and therefore are not usually an accurate guide to therapy at this point. So a total cholesterol below the target of < 4.0 mmol/l in the acute situation is not a reason to delay treatment with a statin. Fourthly, it emphasises to the person with the disease the importance of lipid lowering, by both lifestyle and drug intervention, for their future cardiovascular health. Finally, starting treatment in hospital is more likely to result in the same treatment being continued in general practice. There will be clinical exceptions to this pragmatic policy—for example, a person with stroke related dementia and a poor life expectancy—but most people with acute atherosclerotic disease will be suitable for statin treatment. Assessment for secondary causes of dyslipidaemia should take place at the same time. About 8–12 weeks after the acute event fasting lipids should be measured and drug therapy appropriately modified to ensure lipid targets are achieved.
People with diabetes mellitus
For people with diabetes mellitus (without CVD) fasting lipids should be measured. If they meet the criteria for statin therapy (see above) give lifestyle advice, monitor blood lipids, and treat to target. Low HDL cholesterol and elevated triglycerides are commonly seen in type 2 diabetes and may also require treatment on specialist advice once the total and LDL cholesterol targets are achieved.
People at high total CVD risk
For asymptomatic people who are at high total risk (CVD risk ⩾ 20% over 10 years) of developing CVD, a guide for the management of lipids is given in fig 6.

Risk thresholds and targets for blood cholesterol in asymptomatic people without CVD. †Assessed with CVD risk chart.
Familial dyslipidaemias
People with familial hypercholesterolaemia
Familial hypercholesterolaemia (FH) is an autosomal dominant disorder with an estimated prevalence of 1 in 500 of the adult population.55 Clinically it is characterised by hypercholesterolaemia (total cholesterol is usually > 9 mmol/l), and this is principally due to elevated LDL cholesterol values, the presence of tendon xanthomata, the premature development of CHD, and a family history of one or more of these. The criteria for the diagnosis of FH are given in table 10 or via PRODIGY (http://www.prodigy.nhs.uk).
Criteria for clinical diagnosis of familial hypercholesterolaemia (FH)
In people with FH, angina or acute coronary syndromes (non-fatal and fatal) typically occur in men between 30–50 years, and in women between 50–70 years. The Simon Broome Register of Genetic Hyperlipidaemia shows that FH people who have not already developed CHD have a CHD mortality rate at least 10 times greater than the general population.56 This very high risk of premature atherosclerotic coronary disease is further exacerbated by other risk factors such as smoking and elevated blood pressure. Early identification of people with FH should result in appropriate professional lifestyle intervention, treatment with a statin, and, where necessary, other lipid lowering therapies including apheresis and plasmapheresis, to achieve LDL cholesterol values as low as possible. This will result in a reduction in risk, a lower mortality, and longer life expectancy.56 FH is present in about 5–10% of individuals who develop CHD before the age of 55 years.57 Therefore, it is particularly important that all the first degree relatives of people with premature CHD (men < 55 years and women < 65 years) are screened for lipids. The effectiveness of cascade testing in the relatives of FH people has been demonstrated in this country.58 In England the Department of Health has commenced a pilot clinical study of FH case finding by cascade screening of first degree relatives of identified probands.59 Guidelines for children are to be found in the joint publication of the former British Hyperlipidaemia Association and the British Paediatric Association on Paediatric Hyperlipidaemia.60 People with FH and their families should all be looked after by lipid specialists.
People with familial combined hyperlipidaemia
Familial combined hyperlipidaemia (FCH) comprises a heterogeneous group of lipid disorders of variable inheritance pattern.61,62 The prevalence is at least 1 in 300 of the adult population. They are characterised by raised cholesterol and/or triglycerides, and premature CHD in family members. For more information visit PRODIGY (http://www.prodigy.nhs.uk). People with FCH and their families should also be managed by lipid specialists.
Selection of drug therapies
The lipid lowering drug classes include inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase (statins), fibrates, bile acid sequestrants (anion exchange resins), nicotinic acid and its derivatives, fish oils, and an inhibitor of cholesterol absorption. The first five classes of drugs (but not all drugs within each class) have been shown in trials to reduce myocardial infarction and coronary death. However, the most convincing clinical trial data in relation to cardiovascular events and total mortality is for the statin class. The compelling and possible indications, contraindications, and cautions for the major lipid modifying drugs are shown in table 11. Lipids and lipoproteins may be influenced by other drugs such as insulin, metformin, thiazolidinediones, orlistat, and sibutramine.
Compelling and possible indications, contraindications, and cautions for the major classes of lipid lowering drugs*
Statins
The HMG-CoA reductase inhibitor (statin) class is the most potent of the lipid lowering drug classes for lowering total and LDL cholesterol, is administered once daily with few side effects, and has a good long term safety record. The principal effect of statins is to lower LDL cholesterol but they also raise HDL cholesterol and lower triglycerides to some extent. The statins are first line drugs for reducing total and LDL cholesterol (table 11).
Other agents
Other lipid lowering drugs will be needed in some people, usually in combination with a statin if the total and LDL cholesterol targets are not achieved with a statin alone, or in place of a statin when the primary lipid abnormality is severe hypertriglyceridaemia (> 10 mmol/l), or when people are intolerant of statins.
Fibrates
Fibrates, working by modulation of nuclear receptors in various tissues (predominantly liver, muscle, and adipose tissue), raise HDL cholesterol and lower triglycerides. They are primarily indicated for the management of mixed lipaemia and hypertriglyceridaemia.63 They are the drug class of choice for familial dysbetalipoproteinaemia (type III hyperlipoproteinaemia, remnant hyperlipidaemia). Some fibrates, but not gemfibrozil, may be added to statin therapy on specialist advice where hypertriglyceridaemia and low HDL persist after LDL cholesterol has been treated to target.64
Bile acid sequestrants
The anion exchange resins, cholestyramine and colestipol, bind bile acids in the intestine. This results in increased LDL receptor activity in the liver which increases the clearance of LDL cholesterol from plasma.
In people who can take resins they can reduce cholesterol substantially, and are appropriate in individuals with severe elevations of LDL cholesterol, as in familial hypercholesterolaemia.
Cholesterol absorption inhibitors
Ezetimibe, the first of a new class of cholesterol absorption inhibitor which blocks cholesterol absorption in the gut, is now available. It can lower LDL cholesterol by around 15–20% when added to diet, or by 20–25% when added to diet with a statin.65 Unlike resins, ezetimibe is well tolerated. It should be used either in addition to a statin, or as monotherapy in statin intolerant individuals. There are no randomised controlled trial data in relation to CVD morbidity or mortality, or long term safety, but trials are in progress.
Nicotinic acid
Nicotinic acid raises HDL cholesterol and reduces triglycerides. It works through inhibition of adipose tissue lipolysis, and inhibition of hepatic triglyceride synthesis. It has been used with statins and other lipid lowering agents with benefit in angiographic studies of atheroma progression. Flushing is a common side effect and can be reduced if taken in the evening with food, and the concurrent use of low dose aspirin. Slow release preparations may be helpful.
Omega-3 (n-3) fatty acids/fish oils/DHA-EPA
Omega-3 fatty acids (fish oils) at a dose of 2–4 g/day, or omega-3 marine triglycerides at a dose of 5–10 g/day, are licensed for lowering triglycerides. Omega-3 fatty acids are also licensed for the prevention of CHD at the lower dose of 1–2 g/day. Fish oils can be used with statins or with other lipid lowering therapies.
Combinations of drug therapies
Combination statin–fibrate therapy
There are no large randomised clinical trials with statin–fibrate combinations yet published. For most people with both elevated cholesterol and triglycerides, treatment should still start with a statin. Where persistent hypertriglyceridaemia is present after LDL targets are achieved, a combination of a statin with a fibrate (using fenofibrate, bezafibrate, or ciprofibrate) can be considered on specialist advice.64 Gemfibrozil should not be used in combination with a statin. When a statin–fibrate combination is used, monitoring of CK and ALT is appropriate.
Combination of statins with inhibitors of cholesterol absorption
Ezetimibe is well tolerated in combination with statins, but there are no long term safety or outcome trials.
Safety of statins
The increasingly large evidence base for statin therapy shows a very high benefit to hazard ratio for individuals with increased atherosclerotic risk. In a systematic review and meta-analysis of 58 trials of statins there was no excess risk for statin therapy. For a 1.0 mmol/l reduction in LDL cholesterol there was no significant effect on deaths from circulatory diseases other than CHD and stroke (0.87, 95% CI 0.73 to 1.03); for cancer deaths (1.06, 95% CI 0.96 to 1.16); for injuries and suicide (0.94, 95% CI 0.72 to 1.23); and for diseases other than circulatory diseases and cancer (0.88, 95% CI 0.78 to 1.01).40 In the Cholesterol Treatment Trialists’ Collaboration there was no evidence that lowering LDL cholesterol by 1 mmol/l with five years of statin therapy increased the risks of any specific non-vascular cause of death or of any specific type of cancer.40 There was a non-significant reduction in non-vascular mortality (rate ratio 0.95, 95% CI 0.90 to 1.01) in the context of a 12% proportional reduction in all cause mortality (0.88, 95% CI 0.84 to 0.91). There was no evidence of an increased risk of developing cancer (1.00, 95% CI 0.95 to 1.06), no evidence of an excess incidence of cancers with increasing duration of treatment, and no excesses among any particular site-specific cancer. In HPS there was no significant excess in liver enzymes (ALT) comparing statin with placebo, and neither was there any significant difference between the groups in the number of participants whose drug was stopped because of elevated liver enzymes.38 There was no significant difference in unexplained muscle pain and weakness, nor in the numbers of study participants whose study treatment was stopped because of such symptoms. There was no significant excess of elevated CK comparing statin with placebo, and only a slight but non-significant excess of statin treated participants were diagnosed to have a myopathy (muscle symptoms plus CK above 10 times the upper normal limit). The annual excess risk of myopathy with a statin was about 0.01%. A small number of these myopathy cases developed rhabdomyolysis (five on statin and three on “placebo”), but none was fatal. The extremely low incidence of rhabdomyolysis (five year excess: 0.01%) is confirmed by the Cholesterol Trialists’ Collaboration.40 Significant adverse events with statin therapy are therefore rare. Myopathy associated with statins is dose related, is increased when statins are used in conjunction with other therapies sharing common metabolic pathways, and potential drug–drug interactions increase in certain higher risk subgroups of people.66 Although the risk of serious myositis progressing to rhabdomyolysis is very small, education about the typical presentation is essential, namely myositis, generalised muscle discomfort, pain, tenderness, or weakness.
After initiating treatment with a statin, CK only needs to be checked again if definite unexplained muscle symptoms are reported.
Lipid treatment targets
Cholesterol and LDL cholesterol
There are no clinical trials which have evaluated the relative and absolute benefits of cholesterol lowering to different total and LDL cholesterol targets in relation to clinical events. Therefore, targets defined by guidelines are a matter of judgement set in the context of the total CVD risk of trial populations and using, where available, pre-specified and post hoc analyses of total and LDL cholesterol concentrations achieved. The Pravastatin Pooling Project (PPP) reported significant relative reductions in all cause and coronary mortality across most of the baseline LDL cholesterol concentrations from 5.5 mmol/l down to 3.2 mmol/l.67 In the lowest quintile (< 3.5 mmol/l) of the CARE/LIPID studies22,23 there was no significant treatment effect. However, since then the HPS, which recruited about 3500 people with a pre-treatment LDL cholesterol value already below 2.6 mmol/l, and reducing that with a statin to an average of 1.7 mmol/l, produced a relative reduction in risk about as great as that seen among those presenting with higher LDL cholesterol values.38 In this trial a 1.0 mmol/l reduction in LDL cholesterol from 4.0 mmol/l to 3.0 mmol/l reduced the risk of major vascular events by about one quarter, while reducing it from 3.0 mmol/l to 2.0 mmol/l produced the same relative reduction in risk. This evidence from the HPS has been reinforced by more recent statin studies. In the ASCOT trial of 19 342 patients with well treated hypertension, of whom 10 305 were included in the lipid lowering arm (ASCOT-LLA), statin treatment reduced the primary end point of non-fatal myocardial infarction and fatal CHD by 36% (0.64, 95% CI 0.50 to 0.83) by reducing LDL cholesterol from 3.4 mmol/l to 2.3 mmol/l—a reduction of 1.1 mmol/l at three years compared to placebo.27 In the CARDS trial of 2838 people with type 2 diabetes, and no history of CVD,28 treatment with a statin resulted in a 37% relative risk reduction (95% CI 0.48 to 0.83) in major cardiovascular events by reducing LDL cholesterol from 3.0 mmol/l to 2.1 mmol/l.
The PROVE-IT,29 TNT,30,31 and IDEAL32 trials have compared the effects of achieving different LDL cholesterol values, either using different statins or the same statin at different doses, but without placebo comparison groups. In the PROVE-IT trial of 4162 people with a recent acute coronary event, which compared intensive (80 mg atorvastatin daily) with standard (40 mg pravastatin daily) statin therapy, there was a 16% relative reduction (95% CI 5% to 26%) in risk of death from any cause or a major cardiovascular event (combined end point). This was achieved by reducing median LDL cholesterol from 2.7 mmol/l at baseline to 1.6 mmol/l in the intensively treated group, compared to 2.5 mmol/l in the standard group.29 In the TNT study of 10 001 people with coronary disease, treatment with 80 mg atorvastatin daily lowered mean LDL cholesterol values to 2.0 mmol/l, compared to 2.6 mmol/l with the low dose of 10 mg of atorvastatin. This was associated with a relative risk reduction of 22% (95% CI 0.69 to 0.89) in new CVD events over a median 4.9 years. There was no difference in total mortality.31 The IDEAL trial of 8888 people with a history of acute myocardial infarction compared the effects of atorvastatin 80 mg with simvastatin 20/40 mg and there was a 11% reduction in major coronary events (hazard ratio 0.89, 95% CI 0.78 to1.01) which did not reach statistical significance.32 However, there was a 13% reduction in major cardiovascular events (0.87, 95% CI 0.77 to 0.98). There was no difference in all cause, cardiovascular or non-cardiovascular mortality. A secondary end point in the IDEAL trial which included stroke, and which matched the primary end point in TNT,30,31 showed a 13% (p = 0.02) reduction. Similarly, when the primary end point in PROVE-IT29 (any cardiovascular event including revascularisation) was considered in the IDEAL trial there was an identical 16% risk reduction (p < 0.0001). Furthermore, the primary end point results in IDEAL fits exactly on the regression line of the meta-analysis from the Cholesterol Trialists’ Collaboration.40 Therefore, the results of IDEAL are consistent with both PROVE-IT and TNT and also with the meta-analysis from the Cholesterol Trialists’ Collaboration. There is one other large statin trial called SEARCH in which people with CHD are being randomised to treatment with simvastatin at high and low doses, but the results of this trial will not be known until at least 2007.68
An intravascular ultrasound study of people with coronary disease (REVERSAL69) also compared atorvastatin at doses of 80 mg and 10 mg, but over a shorter duration, and showed a significant reduction in progression of atherosclerosis in the intensively treated (80 mg daily) group. This was achieved by reducing LDL cholesterol from 3.9 mmol/l to 2.1 mmol/l, a difference of 0.8 mmol/l compared to the standard therapy (10 mg daily) group with an LDL cholesterol value of 2.8 mmol/l.
The GREACE trial of 1600 people with coronary disease compared managed (“treat to target”) with usual care. In the managed care arm there was up titration of a statin to achieve the old National Cholesterol Educational Program (NCEP) ATP-III target LDL cholesterol of <100 mg/dl (2.6 mmol/l).26 The NCEP LDL cholesterol goal was reached by 95% of the people in managed care at a mean atorvastatin dose of 24 mg/day, compared to 3% of the usual care patients. Total mortality (−43%), coronary mortality (−47%), coronary morbidity (−59% for myocardial infarction and −52% for unstable angina), and stroke (−47%) were all significantly reduced by managed care. This was achieved by reducing LDL cholesterol from 4.7 mmol/l to 2.5 mmol/l in the managed care group, a mean treatment difference of 1.9 mmol/l between managed and usual care.
The Cholesterol Trialists’ Collaboration reported an approximately linear relationship between the absolute reductions in LDL cholesterol achieved in these trials and the proportional reductions in the incidence of coronary and other major vascular events.40 The proportional reduction in the event rate per mmol/l reduction in LDL cholesterol was largely independent of the presenting level. So lowering the LDL cholesterol level from 4 mmol/l to 3 mmol/l reduced the risk of vascular events by about 23%, and lowering LDL cholesterol from 3 mmol/l to 2 mmol/l also reduced the residual risk by about 23%.
Therefore, the lipid targets defined in our recommendations in 1998, and currently endorsed by the NSF on CHD, the NSF on diabetes, and the GMS contract, are now too conservative in the context of the more recent trial evidence with statins in which high risk people are now achieving lower cholesterol values. These trials support the view that in high risk individuals any threshold below which lowering LDL cholesterol does not safely reduce cardiovascular risk is now at a much lower concentration—for example, below 2.0 mmol/l for LDL cholesterol or below 4.0 mmol/l for total cholesterol—than previously demonstrated. The NCEP ATP III guideline70 was revised in 2004 and a lower LDL cholesterol target of < 70 mg/dl (1.8 mmol/l) is advised for people at high risk.71
So we now recommend in people with established CVD, people with diabetes, and those asymptomatic individuals at high CVD risk ⩾ 20% of developing CVD, new total cholesterol and LDL cholesterol targets of < 4.0 mmol/l and <2.0 mmol/l respectively, or a 25% reduction in total cholesterol and a 30% reduction in LDL cholesterol, whichever gets the person to the lowest absolute level. These total and LDL cholesterol targets can usually be achieved with lipid lowering drugs (statins) prescribed at doses whose efficacy and safety have been shown in trials (table 12). The place of statins combined with other lipid lowering drugs has yet to be demonstrated by clinical trials in relation to cardiovascular outcomes.
Optimal and audit standard lipid targets
Although the original lipid target defined in the 1998 recommendations—namely, a total cholesterol < 5.0 mmol/l and LDL cholesterol < 3.0 mmol/l—has now been superseded by new scientific evidence, we have retained it as an audit standard (table 12). This standard is consistent with the new GMS contract and applies to people with established CVD, people with diabetes, and those at high total risk of developing the disease. It represents the minimum standard of care for such high risk people. Wherever possible the optimal lipid targets of a total cholesterol < 4.0 mmol/l and LDL cholesterol < 2.0 mmol/l, or a 25% reduction in total cholesterol and a 30% reduction in LDL cholesterol, whichever gets the person to the lowest absolute level, should be achieved.
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
(D) BLOOD GLUCOSE AND DIABETES
Glycaemia, whether evaluated by fasting glucose, the two hour value from an oral glucose tolerance test (OGTT), or by HbA1c in the healthy population, is continuously related to the risk of developing CVD.1,2 This continuous relation between glycaemia and CVD risk in the population without diabetes mellitus is similar to that of blood pressure and cholesterol—as these risk factors increase across their respective distributions there is a corresponding increase in the risk of CVD.3–5 In addition, as for blood pressure and cholesterol, the absolute risk of CVD associated with any level of glycaemia is also determined by the presence of other risk factors.6 This has important implications for measuring glycaemia in the overall assessment of cardiovascular risk and managing it alongside other risk factors.
Although a continuous relationship between glycaemia and CVD risk exists, the traditional assessment of glycaemia has been with an OGTT which categorises individuals as follows: (1) normal glucose tolerance; (2) impaired fasting glycaemia (IFG); (3) impaired glucose tolerance (IGT); and (4) diabetes mellitus (table 13). For individuals with IGT the relative risk of developing CVD is 1.5 compared to individuals with normal glucose tolerance.2 In people with diabetes the relative risk of CVD is two to fourfold compared to normal glucose tolerance.7–9 Increasingly abnormalities of glucose metabolism are seen as part of the metabolic syndrome which has several definitions, but the NCEP definition is clinically useful as it does not require insulin measurement (table 14). People with the metabolic syndrome as defined are inevitably at higher risk of CVD because this syndrome is based on several interrelated CVD risk factors.10–12
Diagnosis of diabetes mellitus, impaired fasting glucose (IFG), and impaired glucose tolerance (IGT)
Clinical diagnosis of metabolic syndrome
Concomitant CVD risk factors differ according to the type of diabetes. Type 1 diabetes, which occurs largely, but not exclusively, in children and young people, is characterised by loss of pancreatic β cell function and endogenous insulin production, and there is a two- to threefold increase in risk of developing CHD and stroke in later life. This risk is notably increased in those developing diabetic nephropathy. In type 2 diabetes there is insulin resistance and eventual β cell failure which often occurs in the context of central obesity and physical inactivity. Incidence and prevalence increase with age and people with type 2 diabetes commonly have elevated blood pressure, dyslipidaemia, and other risk factors for CVD. All people with type 2 diabetes are at increased CVD risk, even in the absence of diabetic nephropathy. Other markers of CVD risk in people with diabetes include diabetic retinopathy, autonomic neuropathy, erectile dysfunction, microalbuminuria, and proteinuria.13–15
However, in a study of the general population, medically diagnosed diabetes only accounted for 20% of all subsequent fatal CVD. The majority of fatal events came from apparently healthy individuals with a glycated haemoglobin > 6% in the absence of diabetes.16 This relation between glycated haemoglobin in the healthy population and the development of CVD was independent of other CVD risk factors. Importantly, the total risk of CVD, for any value of HbA1c, was further determined by the presence of other factors such as smoking, elevated blood pressure, and dyslipidaemia. So focusing CVD prevention solely on medically diagnosed diabetes will inevitably have a limited impact, as only a minority of glycaemia related fatal CVD events in the population are attributed to diabetes per se. By broadening the clinical focus to include impaired glucose regulation (IFG and IGT) which is outside the diabetic range, will increase the scope and yield for CVD prevention. Impaired glucose regulation and diabetes mellitus are both under-diagnosed in clinical practice. In a study of people admitted to a coronary care unit with myocardial infarction, and who did not have medically diagnosed diabetes, an OGTT three months after diagnosis revealed 40% with IGT and 25% with new diabetes mellitus. When the prevalence of known diabetes at the time of diagnosis (about 15%) is taken into account, approximately 40% of all patients admitted with myocardial infarction had new or known diabetes mellitus.17 If fasting glucose criteria had been used alone for the diagnosis of diabetes then 47% of these new cases of diabetes would have been missed. In Asians with impaired fasting glucose a subsequent OGTT revealed diabetes mellitus in 83% and the other 17% all had IGT.18,19
Although an OGTT is required for the accurate diagnosis of diabetes and impaired glucose regulation, a more pragmatic approach is being increasingly followed in clinical practice. This is based on a measurement of random (non-fasting) glucose followed, where necessary, by fasting blood glucose to detect dysglycaemia. This approach will detect all those with IFG but, inevitably, some with IGT or even diabetes will be missed. It is important to measure random and fasting glucose alongside other cardiovascular risk factors. Intervening through lifestyle to reduce glycaemia, and control other risk factors like blood pressure and lipids, can prevent the development of diabetes as well as CVD.
Assessment of plasma glucose
All adults from 40 years onwards should have a random (non-fasting) blood glucose measured as part of an opportunistic CVD risk assessment in primary care. This can be a plasma venous sample or a capillary blood sample. For asymptomatic individuals with no history of CVD or diabetes this glucose value should be viewed in the context of total CVD risk based on the Joint British Societies’ cardiovascular risk prediction chart. Those who are not found at this cardiovascular risk assessment to be at high total CVD risk, and not to have newly diagnosed impaired glucose regulation or diabetes, should have their glucose and risk assessment repeated, ideally within five years.
At present there is no cardiovascular risk assessment model which incorporates one or more of the different measures of glycaemia, together with other cardiovascular risk factors, in order to estimate total risk of developing CVD for the general population. Therefore, a pragmatic strategy for assessing glycaemia in clinical practice is to measure random glucose as part of an initial cardiovascular risk assessment (fig 7). If random glucose is normal (⩽ 6.0 mmol/l) there is no need to repeat this measurement for five years. If the random glucose is potentially abnormal (⩾ 6.1 mmol/l) but not indicative of diabetes (⩾ 11.1 mmol/l) then this should be repeated fasting. If this fasting glucose is ⩾ 6.1 mmol/l but < 7.0 mmol/l, the glucose measurement should be repeated fasting. If the second fasting glucose is still ⩾ 6.1 mmol/l but < 7.0 mmol/l this confirms IFG. If the second fasting glucose is ⩾ 7.0 mmol/l then perform an OGTT. In individuals with no symptoms of diabetes two abnormal fasting values ⩾ 7.0 mmol/l, on separate occasions, are needed for the diagnosis of diabetes mellitus. In the presence of diabetic symptoms a fasting glucose ⩾ 11.1 mmol/l on one occasion is diagnostic of diabetes mellitus.

{kind=link}
{kind=link}
{kind=link}
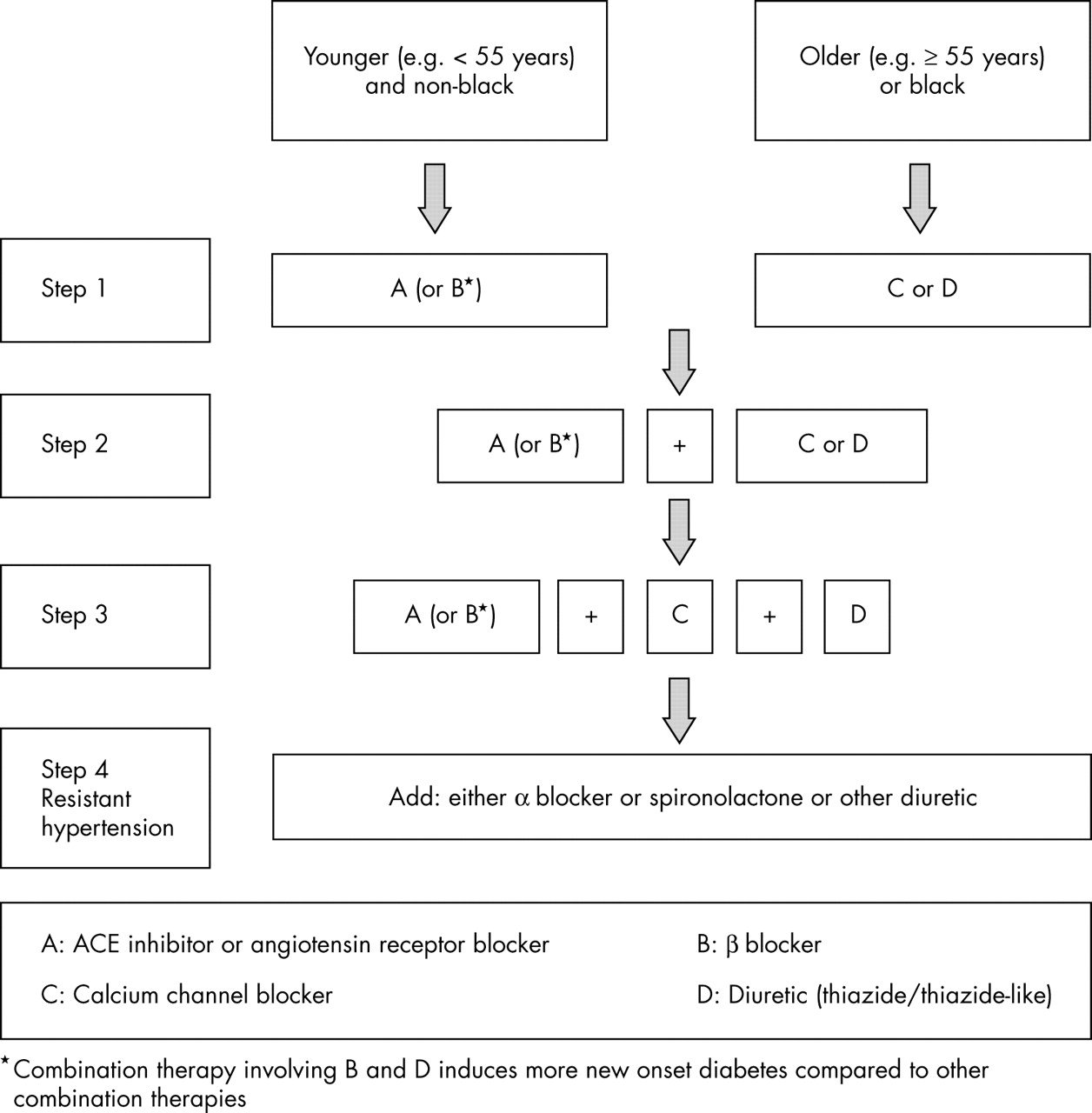{kind=link}
{kind=link}
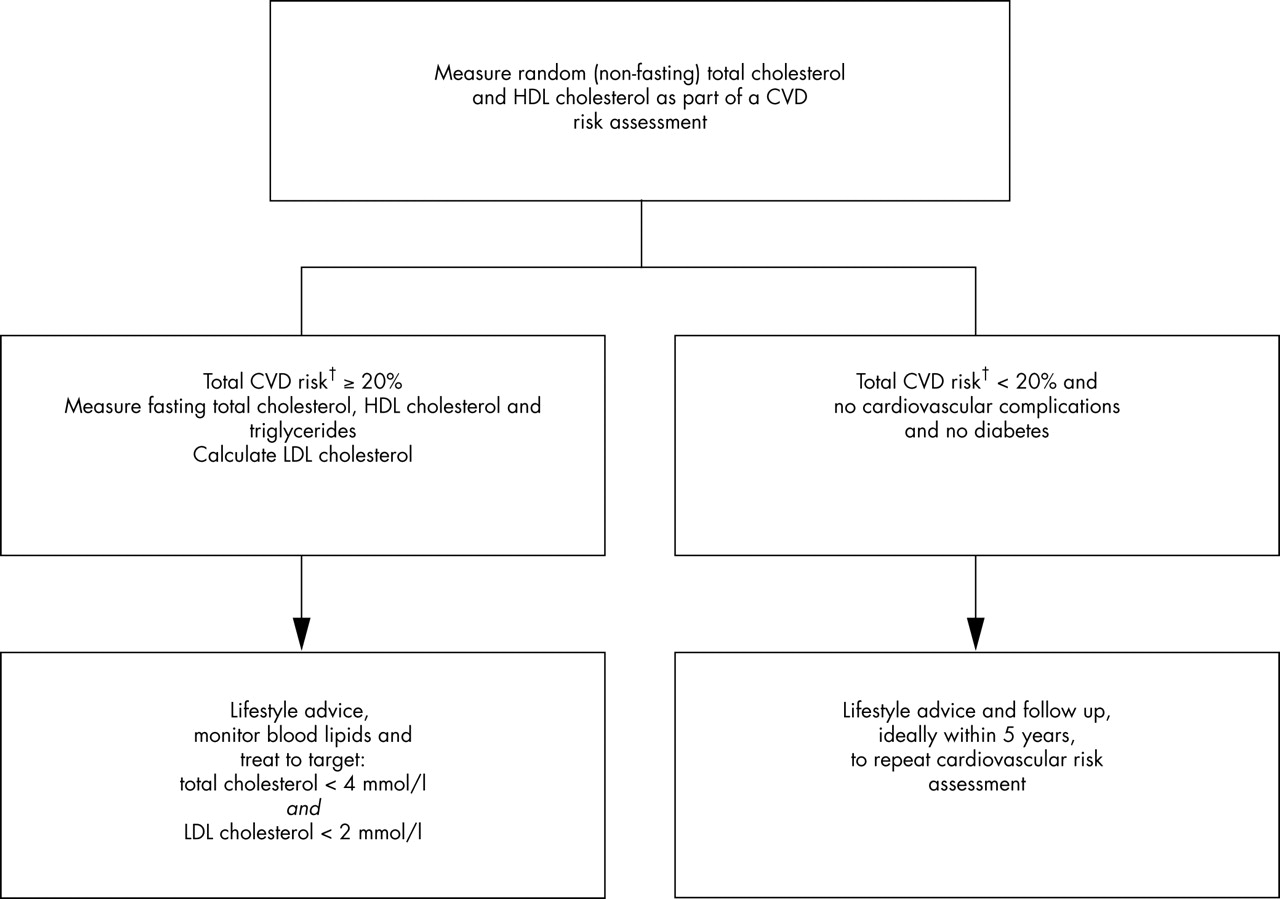{kind=link}
{kind=link}
Risk thresholds and targets for plasma blood glucose in asymptomatic people without CVD. *Impaired glucose tolerance: 2 hour glucose in an OGTT ⩾ 7.8 mmol/l and ⩽ 11.0 mmol/l. OGTT, oral glucose tolerance test. See table 13.
Apparently healthy individuals with a CVD risk ⩾ 20% over 10 years who have IFG or IGT (table 13) should receive appropriate lifestyle and risk factor intervention, including the use of cardiovascular protective drug therapies, to achieve the risk factor targets including glycaemic control. These high risk people with IFG or IGT should have their dysglycaemia, and other cardiovascular risk factors, monitored on an annual basis. If CVD risk is < 20% over 10 years, but IFG or IGT are present, then appropriate lifestyle advice should be given and their CVD risk and fasting glucose measured on an annual basis.
In people who present with an acute CVD event fasting glucose should also be measured on at least one occasion, or an OGTT performed during the in-hospital stay. Fasting glucose should be measured during the acute phase of the illness and, if there is evidence of IFG (⩾ 6.0 mmol/l but < 7.0 mmol/l), or an indication of diabetes (⩾ 7.0 mmol/l) a fasting glucose measurement should be repeated on two occasions (or an OGTT on one occasion) between 8–12 weeks following discharge from hospital. Those with IFG (or IGT) should have fasting glucose, and all other cardiovascular risk factors, measured on an annual basis.
An OGTT is not recommended as a routine part of CVD risk assessment in the general population. However, it can be clinically justified in high risk people because it is the only way to diagnose both components of impaired glucose regulation (IFG and IGT) in addition to diagnosing diabetes. Guidelines on screening for diabetes are expected in 2006.20
Prevention of diabetes
Impaired glucose regulation—both IFG and IGT—are associated with an increased risk of developing type 2 diabetes, and IGT is associated with an increased risk of death from atherosclerotic CVD and all causes. Impaired glucose regulation is associated with other cardiovascular risk factors and metabolic risk factors worsen across the spectrum of non-diabetic glucose tolerance. In people with IGT clinical trials have shown that progression to diabetes can be prevented or postponed by professional lifestyle intervention.21,22 In the largest trial to date, a comprehensive and intensive lifestyle intervention was more effective than metformin (850 mg twice daily) alone in reducing the incidence of diabetes. The development of diabetes in the lifestyle arm was reduced by 58% (95% CI 48% to 66%) compared to 31% for metformin (95% CI 17% to 43%) when both were compared to placebo.23 Other treatments that reduce progression to diabetes include acarbose in IGT, and orlistat in obese individuals with normal or impaired glucose tolerance.24,25 It is also important to note that use of β blockers and diuretics are associated with a significant increase in new cases of diabetes over trial periods of approximately five years in comparison to placebo and other antihypertensive therapies.26,27
Blood pressure, lipids, and glucose in diabetes
Blood pressure
Elevated blood pressure greatly increases the already elevated CVD risk in people with diabetes.28 Elevated blood pressure (blood pressure > 140/90 mm Hg) is twice as common in people with diabetes compared to people without diabetes. The combination of hypertension and diabetes doubles the risk of developing microvascular and macrovascular complications, and doubles the risk of mortality when compared to non-diabetic people with hypertension.
The evidence for blood pressure reduction in diabetes mellitus comes predominantly from subgroup analyses of clinical trials which included people with diabetes. The UKPDS randomised people with diabetes and hypertension in a substudy to intensive or less intensive antihypertensive therapy.29 More intensive therapy significantly reduced the risk of stroke by 44% and there was also a lower 21% risk of myocardial infarction, although the latter did not achieve statistical significance. Blood pressure lowering has been shown in those trials which included people with diabetes to reduce or prevent an aggregate of major cardiovascular events including heart failure, cardiovascular death, and total mortality. There is also evidence in randomised trials of people with diabetes, but without CVD, that reducing blood pressure reduces progression to retinopathy, albuminuria, and the progression of nephropathy.
The blood pressure target for people with diabetes is lower than for those without diabetes at < 130/80 mm Hg. The reasons are as follows. First, the trial data show that the greater the blood pressure lowering the greater the benefit in terms of cardiovascular events, and from observational data there appears to be no blood pressure threshold below which risk no longer declines.30 Second, strict control of blood pressure is the most important factor preventing the development of diabetic nephropathy and end stage renal failure.31,32 Therefore, a blood pressure treatment target of less than 130/80 mm Hg is recommended but it is recognised that this is difficult to achieve, especially in the older population with diabetes and isolated systolic hypertension.33–35 However, this target is not based on extensive clinical trial evidence.36,37 An audit standard for all people with diabetes should be to reduce blood pressure to below 140/80 mm Hg. Thereafter further cardiovascular benefit can be expected if the blood pressure is lowered to an optimal target of less than 130/80 mm Hg, particularly in those with diabetic nephropathy and retinopathy.
Almost all people with hypertension and diabetes will require a combination of blood pressure lowering drugs to achieve the recommended blood pressure targets, with many requiring three or more drugs. This combination is likely to include a drug which blocks the renin–angiotensin system (ACE inhibitor or ARB). The evidence for renin–angiotensin system blockade is strongest for nephroprotection (and reduction in surrogates such as proteinuria).38–43 When there are no cost disadvantages, the combined drugs should be used as a fixed dose combination to reduce the number of medications. Other drugs will be required to achieve blood pressure targets in most people such as thiazide/thiazide-like diuretics, longer acting CCBs, α blockers, or low dose spironolactone.44 In people with renal impairment and/or oedema, a loop diuretic may be required as an alternative to, or in addition to, a thiazide/thiazide-like diuretic.
Lipids
The evidence for cholesterol reduction in diabetes mellitus in relation to CVD has, until recently, also come predominantly from subgroup analyses of clinical trials which included people with diabetes. For people with established CVD several trials of statins, and one trial of the fibrate drug gemfibrozil, have all shown significant reductions in coronary and cardiovascular events in people with diabetes comparable to that seen in those without diabetes.45–49 The HPS included people with both type 1 and type 2 diabetes, and had more people with diabetes than all previous studies combined.50 A third had a history of coronary disease and two thirds were at high risk from diabetes without CVD. There was a significant reduction in CHD and stroke in people with diabetes of a similar relative size to that reported for those without diabetes. This treatment effect was independent of baseline cholesterol. In the ASCOT-LLA trial 2532 people had diabetes and there was a non-significant 16% reduction in the primary end point of fatal CHD and myocardial infarction (0.84, 95% CI 0.55 to 1.29). This result is likely to reflect reduced statistical power in a trial which was stopped early and therefore had a lower number of primary end points. All CVD events as a secondary end point were significantly reduced by 23% (0.77, 95% CI 0.61 to 0.98) without heterogeneity from the overall result.51 CARDS is the only trial to date to evaluate statin therapy exclusively in diabetes in the primary prevention of CVD. A total of 2838 people with type 2 diabetes and one risk factor (retinopathy, albuminuria, current smoking, or hypertension) were randomised to a statin or placebo.52 Like the ASCOT-LLA trial, the CARDS trial was also stopped earlier than expected because the pre-specified stopping rule for efficacy had been met. In people with diabetes treated with a statin the primary combined end point of acute coronary events, coronary revascularisation, or stroke was reduced by 37% (0.63, 95% CI 0.48 to 0.83). Taken separately acute coronary events and stroke were both significantly reduced by 36% and 48%, respectively. Together these trials provide convincing evidence that statin treatment is effective for prevention of CVD in diabetes mellitus.
Therefore, we recommend the following indications for statin therapy in diabetes:
(1) all those who are aged 40 years or more with either type 1 or 2 diabetes; and
(2) for people aged 18–39 years with either type 1 or 2 diabetes and who have at least one of the following:
-
retinopathy (pre-proliferative, proliferative, maculopathy)
-
nephropathy, including persistent microalbuminuria
-
poor glycaemic control (HbA1c > 9%)
-
elevated blood pressure requiring antihypertensive therapy
-
raised total blood cholesterol (≥ 6.0 mmol/l)
-
features of metabolic syndrome (central obesity and fasting triglyceride > 1.7 mmol/l (non-fasting > 2.0 mmol/l) and/or HDL cholesterol > 1.0 mmol/l in men or > 1.2 mmol/l in women)
-
family history of premature CVD in a first degree relative.
Although the most common form of dyslipidaemia in diabetes is low HDL cholesterol and elevated triglycerides, the roles of fibrates and the nicotinic acid group are still unclear and a statin is the drug class of first choice.53
Glycaemic control in diabetes
Good glycaemic control has been showed in clinical trials to prevent microvascular complications in both type 1 and type 2 diabetes.54–57 In the UKPDS trial people with type 2 diabetes with an average HbA1c of 7.0% (intensive treatment cohort) had considerably less microvascular complications than the conventional treatment cohort who had an HbA1c of 7.9%. The UKPDS study has also shown that good glycaemic control reduces the risk of stroke with a favourable trend for a lower risk of myocardial infarction (p = 0.052).58 The DCCT study showed clear evidence of benefit from good glycaemic control in people with type 1 diabetes with respect to microvascular complications.59 However, this study was not sufficiently powered to give any information on macrovascular disease. So glycaemic control is important for people with both type 1 and type 2 diabetes. Ideally, the glucose target for type 1 and type 2 diabetes is normoglycaemia (fasting glucose ⩽ 6.0 mmol/l) with the avoidance of hypoglycaemia and decompensated hyperglycaemia. Optimal clinical management targets are a normal HbA1c% (< 6.0%), and fasting or pre-prandial glucose values of 4.0–6.0 mmol/l. In clinical practice the practical HbA1c% target is ⩽ 6.5%, with an audit standard of ⩽ 7.5%.
In type 1 diabetes glucose control requires appropriate insulin therapy and concomitant professional dietary and lifestyle therapy. In type 2 diabetes professional dietary advice, reduction of overweight, and increased physical activity should be the first approach to achieve good glucose control. If these measures do not lead to a sufficient reduction of hyperglycaemia, oral hypoglycaemic drugs (biguanide, sulfonylurea, thiazolidinediones, or a combination) or insulin has to be added to the treatment regimen. In overweight and obese people metformin is the drug of first choice.
Metformin in obese people with diabetes had a better outcome in a retrospective analysis of the UKPDS trial than those on treatment with insulin or a sulfonylurea.60 Therefore metformin should still be the first line drug for treatment of people with type 2 diabetes with a BMI ⩾ 25 kg/m2. There was evidence of cardiovascular benefit with metformin, in contrast to insulin or sulfonylurea treatment, in reducing cardiovascular events and total mortality, when compared to conventionally treated obese people. Second line agents could include sulfonylureas, postprandial glucose regulators, and thiazolidinediones. A randomised controlled trial of a thiazolidinedione in 5238 people with type 2 diabetes did not achieve the composite primary end point (hazard ratio 0.90, 95% CI 0.80 to 1.02), but there was a reduction in the composite of all cause mortality, non-fatal myocardial infarction and stroke (0.84, 95% CI 0.72 to 0.48). So there is now prospective trial evidence for another oral anti-diabetic drug in relation to cardiovascular events.61 Insulin treatment should be considered as soon as treatment with oral agents fails to achieve the audit target HbA1c of ⩽ 7.5%.
The DIGAMI trials of people with an acute myocardial infarction and a glucose level ⩾ 11.1 mmol/l evaluated a glucose insulin infusion followed by at least three months of insulin therapy. The second trial (DIGAMI 2) did not confirm the results of the first trial and there was no evidence of benefit in relation to total or coronary mortality or non-fatal cardiovascular events.62
Multifactorial interventions in diabetes to reduce CVD
The clinical trial evidence for prevention of CVD in diabetes is largely based on single risk factor interventions. However, the Steno-2 study has provided some evidence for the cardiovascular benefits following a multifactorial intervention programme.62,63 One hundred and sixty patients with type 2 diabetes and microalbuminuria were randomised to receive conventional treatment, or more intensive treatment, with stepwise implementation of behaviour modification and drugs that targeted glycaemia, blood pressure, dyslipidaemia, microalbuminuria (treated with an ACE inhibitor or an ARB), and prophylactic aspirin over a period of 7.8 years. Eighty five cardiovascular events occurred in 35 of the 80 (44%) people in the conventional group, and 33 events in 19 of the 80 (24%) people in the intensive therapy group.60 Cardiovascular disease was reduced in the intensive group by 53% (0.47, 95% CI 0.24 to 0.73), stroke by 85%, amputations by 50%, nephropathy by 61% (0.39, 95% CI 0.17 to 0.87), retinopathy by 58% (0.42, 95% CI 0.21 to 0.86), and autonomic neuropathy by 67% (0.37, 95% CI 0.18 to 0.70) compared with conventional care. The multifactorial lifestyle and polypharmacy approach advocated in the Steno-2 study is similar to the approach advised in this guideline for all people with diabetes.
Although this section has focused predominantly on type 2 diabetes, in type 1 diabetes there is an even higher risk of premature cardiovascular disease.64,65 Therefore CVD risk reduction should be integral to the management of type 1 diabetes, principally through lifestyle in childhood, and then drug therapies for blood pressure and lipids in adulthood.66 The 10 year Pittsburgh study which followed up people with type 1 diabetes demonstrated that blood pressure, lipids, and concomitant peripheral vascular or renal disease are important risk factors for the prediction of CVD.67
Effective care in diabetes involves a multi-professional approach working across all healthcare boundaries. The close involvement of the person with diabetes is essential in planning individualised but effective care. CVD prevention has to be integrated with the management of other diabetic complications such as diabetic retinopathy, microalbuminuria/proteinuria, and erectile dysfunction. Otherwise, care may become fragmented by focusing on specific diabetic complications rather than on all aspects of cardiovascular risk. Most people with diabetes will need evidence based polypharmacy: aspirin, metformin (type 2 diabetes), lipid lowering drug (a statin), and antihypertensive drugs. The main components of diabetes care can usefully be remembered, both by healthcare professionals and those with diabetes, by using the “Alphabet Strategy”68:
-
Advice—Education, self management, concordance with treatment. Special focus on smoking cessation, diet, physical activity, and weight reduction.
-
Blood pressure targets—Blood pressure < 130/80 mm Hg, which may require combinations of a diuretic, ACE inhibitor/ARB, and a CCB (audit standard < 140/90 mm Hg).
-
Cholesterol and LDL cholesterol targets—Total cholesterol < 4.0 mmol/l and LDL cholesterol < 2.0 mmol/l or a 25% reduction in total cholesterol and a 30% reduction in LDL cholesterol, which ever gets the person to the lowest absolute level. A non-HDL cholesterol < 3.0 mmol/l and triglycerides < 1.7 mmol/l are preferred values but are not targets. Nor is there a target for HDL cholesterol, but values below 1.0 mmol/l in men (1.2 mmol/l in women) are associated with an increased risk of CVD.
-
Diabetes control—A normal HbA1c% is ideal but the practical target is ⩽ 6.5%. Metformin is the first choice for most people with type 2 diabetes, especially if overweight. Early recourse to multiple therapies and insulin will be needed if targets are not reached. While the evidence is limited, attention to glycaemic control in the context of acute coronary syndromes is advised, and the DIGAMI protocol may be an appropriate strategy.
-
Eye care—Yearly digital photography is recommended with appropriate ophthalmological referral if retinopathy is present, and management of all other CVD risk factors.
-
Feet care—Yearly examination with appropriate referral as required, and management of all other CVD risk factors.
-
“Guardian” drugs for cardiovascular prevention—Aspirin 75 mg daily is indicated for people with diabetes who meet any of the following criteria:
established atherosclerotic disease
≥ 50 years, or who are younger but have had the disease for more than 10 years, or who are already receiving treatment for hypertension.
A statin is appropriate in most people with diabetes in order to achieve the total and LDL cholesterol targets.
ACE inhibitor/ARB therapy is indicated when there is microalbuminuria or proteinuria or diabetic nephropathy.
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
(E) OTHER RISK FACTORS
Family history
A family history of CVD should be part of the assessment of all people with atherosclerosis and apparently healthy high risk individuals. The risk of CHD increases specifically: (1) when an individual is closely related (parent, sibling or offspring) to a family member who has developed CHD; (2) as the percentage of family members with CHD increases; (3) the younger the age at which a family member develops CHD. Risk factor screening should be undertaken in all first degree relatives of people with premature CHD (men < 55 years and women < 65 years). Families with familial dyslipidaemias will be detected in this way and affected family members require specialist treatment in a lipid clinic. A family history of premature CHD, or other atherosclerotic disease, should be taken into account in assessing the total risk of developing CVD in a healthy individual. Lifestyle advice and appropriate therapeutic management of risk factors should be offered to families where CHD is prevalent.
Other newer risk factors
Other newer risk factors which may have a clinical role continue to be the subject of research. These include apolipoprotein B,1 small dense LDL,2 markers of inflammation (for example plasma C reactive protein (CRP)),3 chronic infections,4 thrombogenic factors such as fibrinogen,3,5–7 platelet activating factor acetyl hydrolase,8 homocysteine,9–11 paraoxonase,12 and candidate genes (for example, for Apo E, ACE and others).13–17 However, none of these factors add substantially to CVD risk prediction, above that of the major classical risk factors, and nor do they have a clearly defined role in the clinical management of people. Therefore, for the present they have no place in routine investigation or management of people with established atherosclerotic disease or in those at high risk of developing this disease.
(F) ETHNICITY
Epidemiological studies have shown that Asians in this country are at increased risk of CHD and CVD; the excess risk of CHD is reported to be about 40% or more compared to the population of England and Wales.18–23 However, in a recent systematic review there is no direct evidence that Asians have a higher incidence of CHD once diabetes has been accounted for, and prevalence data suggest heterogeneity within Asian populations.24 Although CHD is an important disease in Asians this systematic review questions whether this risk is common to Indians, Pakistanis, and Bangladeshis. One population based study has shown important differences between Indians, Pakistanis, and Bangladeshis in the pattern of coronary risk factors.25 In the African-Caribbean population CHD mortality is about 50% lower in men (and about 25% lower in women) compared to white caucasians. However, African-Caribbean people have high rates of hypertension and stroke. In clinical practice it would be pragmatic to provide lifestyle advice appropriate to the person’s culture and to manage risk factors such as blood pressure and lipids with drug therapies to the same targets defined in this guideline.
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
(VI) CARDIOVASCULAR PROTECTIVE DRUG THERAPIES
Since 1998 new systematic reviews, meta-analyses, and individual clinical trial results have been published on the use of cardioprotective drug therapies for both people with established CVD and individuals at high risk of developing symptomatic atherosclerotic disease. In addition to drugs which may be needed to control symptoms and manage blood pressure, lipids, and glucose values to goal, the use of cardioprotective drugs shown in clinical trials to reduce CVD morbidity and mortality and all cause mortality must be considered. While some of these drugs are appropriate for all individuals at high total risk, whether from established CVD or at high risk of developing CVD, others are specifically indicated for selected people. The recommended use of drug therapies in people with atherosclerotic disease and those at high risk of developing the disease is shown in table 6 (see page v18).
(1) Antiplatelet therapies
(i) Atherosclerotic disease
Aspirin or other platelet modifying drugs are recommended in virtually all people with established atherosclerotic disease.
The most recent meta-analysis of antiplatelet trials by the Antithrombotic Trialist’s Collaboration provides convincing evidence of a significant reduction in all cause mortality, vascular mortality, non-fatal re-infarction of the myocardium, and non-fatal stroke in people with unstable angina, acute myocardial infarction, stroke, TIAs, or other clinical evidence of vascular disease.1,2 In the trials which used aspirin the most widely tested doses varied between 50–325 mg/day. There was no evidence of any greater clinical benefit for any doses within this range. Side effects from aspirin are lowest in those using lower dosages. Hence, the available evidence supports daily doses of aspirin in the range of 75–150 mg for the long term prevention of serious vascular events in high risk people, and it is common practice to prescribe 75 mg daily. Although there is no clinical trial evidence of treatment beyond a few years, it would be both prudent and safe to continue aspirin therapy for life. So for people with established atherosclerotic disease aspirin 75 mg daily is indicated for life.
For people with acute coronary disease, unstable angina or non-ST segment elevation myocardial infarction (NSTEMI), clopidogrel with aspirin has been shown to reduce the composite outcome of cardiovascular death, myocardial infarction, and stroke during the year following the hospitalisation (CURE trial).3 To evaluate the efficacy and safety of antiplatelet therapies against aspirin requires very large clinical trials. Only clopidogrel 75 mg/day has been tested in a single large trial against aspirin at a dose of 325 mg/day (CAPRIE).4 The two drugs were equally effective at preventing major vascular complications in people with recent myocardial infarction or ischaemic stroke. However, clopidogrel was more effective than aspirin among people with symptomatic peripheral arterial disease. As clopidogrel has a better side effect profile than aspirin this drug should be considered as an alternative to aspirin but only if the latter causes side effects.
If people with established atherosclerotic disease have a further event despite aspirin therapy (and in ischaemic stroke or TIA with or without the addition of dipyridamole M/R) the place of additional antiplatelet therapy is uncertain.
(ii) Diabetes mellitus
Aspirin 75 mg daily is recommended for all people with type 2 diabetes who are ≥ 50 years of age, and selectively in younger people with one of the following criteria: (1) who have had the disease for more than 10 years; (2) or who are already receiving treatment for hypertension; (3) or who have evidence of target organ damage in the form of retinopathy or nephropathy, and whose blood pressure is controlled to at least < 150/90 mm Hg, and preferably to the optimal target of < 130/80 mm Hg.
(iii) Asymptomatic high risk individuals
In asymptomatic high risk individuals with no history of CVD a meta-analysis has shown that aspirin reduced the risk of all cardiovascular events and non-fatal myocardial infarction but increased the risk of haemorrhagic strokes and major gastrointestinal bleeding.5 The net benefit of aspirin increases as cardiovascular risk rises and therefore estimating total risk of CVD is an absolute prerequisite to initiating antiplatelet therapy.5,6 Therefore, if the total CVD risk is ⩾ 20% over 10 years then prophylactic aspirin is appropriate as long as the blood pressure has been controlled. In primary prevention of CVD in women the benefits of aspirin in relation to the risk of cardiovascular events was only observed among women 65 years of age or older.7 The blood pressure should be reduced to at least the audit standard of < 150/90 mm Hg, and preferably to the optimal blood pressure target before aspirin is started. The HOT study assessed the effect of blood pressure lowering to one of three targets on cardiovascular outcome. The effect of aspirin in this cohort of hypertensive people was also examined. Aspirin reduced major cardiovascular events by 15% and all myocardial infarctions by 36%. There was no beneficial effect on stroke reduction or fatal bleeds with aspirin, but non-fatal bleeds were doubled with aspirin although with a prevalence of < 1% overall. Therefore control of blood pressure before initiating treatment with aspirin is particularly important.
When aspirin cannot be tolerated in asymptomatic high risk individuals, including those selected people with type 2 diabetes as defined above, alternative antiplatelet therapy can be considered.
In asymptomatic individuals with a CVD risk < 20% over 10 years, a small absolute vascular benefit with aspirin may be offset by the slightly greater absolute risk of bleeding complications and therefore prophylactic aspirin is not indicated.
(2) β Blockers
(i) Coronary heart disease
β Blockers are indicated in people with CHD, unless there are contraindications, for the following reasons:
-
control of symptoms of myocardial ischaemia
-
CVD protection following myocardial infarction
-
treatment of heart failure
-
reduction of blood pressure to target < 130/80 mm Hg.
In a meta-analysis of β blockers following myocardial infarction, there was evidence of a significant reduction in all cause mortality, cardiovascular death and in particular sudden cardiac death, as well as non-fatal re-infarction.8 The absolute benefits of β blockade are greatest in older people (> 60 years) and in people at increased risk of reinfarction and death (for example, people with left ventricular dysfunction or arrhythmias, or both). β Blockers have also been shown to reduce all cause mortality in people with heart failure caused by CHD.9
(3) ACE inhibitors
(i) Coronary heart disease
ACE inhibitors are indicated in people with CHD, unless there are contraindications, for the following reasons:
-
treatment of heart failure
-
treatment of left ventricular dysfunction
-
reduction of blood pressure to target < 130/80 mmHg.
Several clinical trials have shown that ACE inhibitors in people with symptoms or signs of heart failure, or left ventricular dysfunction (mainly caused by CHD), will significantly reduce the risk of death, recurrent myocardial infarction, and progression to persistent heart failure.10–16 Short term studies of ACE inhibitors in the acute phase of myocardial infarction have also shown the risk of death can be reduced.17,18 More recently ACE inhibition has been shown in two large clinical trials (HOPE and EUROPA) to reduce the risk of myocardial infarction and cardiovascular mortality in high risk people (aged 55 years or older with evidence of vascular disease or diabetes plus one other cardiovascular risk factor without left ventricular dysfunction or uncontrolled hypertension)19 and in people with stable angina pectoris without apparent heart failure.20 In the PROGRESS study of people with a previous history of cerebrovascular disease, blood pressure lowering using an ACE inhibitor/diuretic regimen produced significant reductions in the risk of recurrent stroke and cardiovascular events.21 However, in the PEACE trial of stable coronary disease and preserved left ventricular function there was no additional benefit from an ACE inhibitor.22
(ii) Diabetes mellitus
This drug class has also been shown to reduce cardiovascular outcomes in people with diabetes, with and without clinical hypertension.
(iii) Asymptomatic high risk individuals
In asymptomatic high risk individuals ACE inhibitors are also indicated for the following reasons:
-
Reduction of blood pressure to target < 140/85 mm Hg or < 130/80 mm Hg.
(4) Calcium channel blockers
This drug class has been shown to reduce cardiovascular outcomes in people with established atherosclerotic disease, diabetes and asymptomatic individuals at high risk23. This drug class is indicated for the following reasons:
-
Reduction of blood pressure to target < 140/85 mm Hg or < 130/80 mm Hg.
(5) Diuretics
Diuretics are indicated for the following reason:
-
Reduction of blood pressure to target < 140/85 mm Hg or < 130/80 mm Hg.
(6) Anticoagulation
Systemic anticoagulation with coumarins is not indicated prophylactically in all people with coronary artery disease. However, anticoagulation is appropriate in selected people following myocardial infarction who are at increased risk of thromboembolism including those with a large anterior myocardial infarction, left ventricular aneurysm or thrombus, paroxysmal tachyarrhythmias, chronic heart failure, or a history of thromboembolic events.24 Anticoagulation is also indicated for those people in atrial fibrillation at increased risk of stroke or who have a history of cerebral infarction.
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
(VII) AUDIT STANDARDS FOR CVD PREVENTION
People with established atherosclerotic disease
-
Medical record of smoking habit (current smoker, ex-smoker, life long non-smoker, number of cigarettes smoked/day, and number of smoking years)
-
Record of waist circumference (cm), height (m), and weight (kg) and calculated body mass index (BMI = weight/height2) kg/m2
-
Record of blood pressure (mm Hg) within the last year
-
Record of fasting lipids (total cholesterol, HDL cholesterol, triglycerides, and calculated LDL cholesterol) in mmol/l within the last year
-
Record of fasting glucose (mmol/l) within the last year
-
Record for people with diabetes mellitus of HbA1c and, where not already detected, a record of proteinuria/microalbuminuria within the last year
-
Record of prescriptions (and if prescribed reason specified including total daily dose) for:
Antiplatelet therapies
β Blockers
ACE inhibitors/All receptor antagonists
Calcium channel blockers
Statins and other lipid lowering drugs
Anticoagulants
-
People with disease and families offered a place on a comprehensive cardiovascular prevention and rehabilitation programme
Management
-
Current cigarette smokers offered professional smoking cessation supported appropriately with nicotine replacement therapy or other treatments
-
Overweight and obese people, and those with central obesity, offered professional dietetic support.
-
Sedentary people offered professional support to increase physical activity
Drugs
Prescriptions for cardioprotective drugs in all people:
-
Antiplatelet therapies in all people with atherosclerotic disease. Aspirin 75 mg daily or, if aspirin is not tolerated, clopidogrel 75 mg day
-
β Blockers in people without contraindications following myocardial infarction
-
ACE inhibitors in people with coronary disease and heart failure, or left ventricular dysfunction
-
Statins in all people with atherosclerotic disease
-
Anticoagulants in selected people following myocardial infarction at increased risk of thromboembolic events
Blood pressure
Lipids
Glucose
Asymptomatic people at high total risk of developing CVD including people with diabetes mellitus
Medical record
-
Record of smoking habit (current smoker, ex-smoker, life long non-smoker, number of cigarettes smoked/day and number of smoking years)
-
Record of waist circumference (cm), height (m), and weight (kg) and calculated body mass index (BMI = weight/height2) kg/m2
-
Record of blood pressure (mm Hg) within the last five years
-
Record of random total cholesterol and HDL cholesterol in mmol/l (or where appropriate fasting lipids (total cholesterol, HDL cholesterol, triglycerides, and calculated LDL cholesterol in mmol/1)) within the last five years
-
Record of random (non-fasting) glucose and, where appropriate, fasting glucose (mmol/l) within the last five years
-
Record for people with diabetes mellitus of fasting glucose (mmol/l) HbA1c and, where not already detected, a record of proteinuria and microalbuminuria within the last five years
-
Record of total CVD risk using the Joint British Societies’ cardiovascular risk prediction chart
Management
-
Current cigarette smokers offered professional smoking cessation supported appropriately with nicotine replacement therapy or other treatments
-
Overweight and obese people, and those with central obesity, offered professional dietetic support
-
Sedentary people offered professional support to increase physical activity
Drugs
Prescriptions for cardioprotective drugs in all people:
-
Antiplatelet therapy in all high risk people with a blood pressure recorded below the audit standard of < 150/90 mm Hg. Aspirin 75 mg daily or, if aspirin is not tolerated, clopidogrel 75 mg day
Blood pressure
Lipids
Glucose
(VIII) APPENDICES
APPENDIX I
HOW TO USE THE CARDIOVASCULAR RISK PREDICTION CHARTS FOR PREVENTION OF CVD
These charts (see inside front and back covers) are for estimating cardiovascular disease (CVD) risk (non-fatal myocardial infarction and stroke, coronary and stroke death and new angina pectoris) for individuals who have not already developed coronary heart disease (CHD) or other major atherosclerotic disease. They are an aid to making clinical decisions about how intensively to intervene on lifestyle and whether to use antihypertensive, lipid lowering, and antiplatelet medication, but should not replace clinical judgement.
-
The use of these charts is not appropriate for people who have existing atherosclerotic disease or are at higher risk for other medical reasons. Examples are:
CHD or other major atherosclerotic disease
familial hypercholesterolaemia or other inherited dyslipidaemias
renal dysfunction including diabetic nephropathy
type 1 and 2 diabetes mellitus.
-
The charts should not be used to decide whether to introduce antihypertensive medication when blood pressure is persistently at or above 160/100 mm Hg or when target organ damage caused by hypertension is present. In both cases antihypertensive medication is recommended regardless of CVD risk. Similarly the charts should not be used to decide whether to introduce lipid lowering medication when the ratio of serum total to HDL cholesterol exceeds 6. Such medication is generally indicated with such a ratio regardless of estimated CVD risk.
-
To estimate an individual’s total 10 year risk of developing CVD choose the table for his or her sex, lifetime smoking status, and age. Within this square define the level of risk according to the point where the coordinates for systolic blood pressure and the ratio of total cholesterol to high density lipoprotein (HDL) cholesterol meet. If no HDL cholesterol result is available, then assume this is 1.0 mmol/l and the lipid scale can be used for total cholesterol alone.
-
Higher risk individuals (red areas) are defined as those whose 10 year CVD risk exceeds 20%, which is approximately equivalent to a CHD risk of > 15% over the same period.
-
The chart also assists in the identification of individuals whose 10 year CVD risk is moderately increased in the range 10–20% (orange area) and those in whom risk is lower than 10% over 10 years (green area).
-
Smoking status should reflect lifetime exposure to tobacco and not simply tobacco use at the time of assessment. For example, those who have given up smoking within five years should be regarded as current smokers for the purposes of the charts.
-
The initial blood pressure and the first random (non-fasting) total cholesterol and HDL cholesterol can be used to estimate an individual’s risk. However, the decision on using drug therapy should generally be based on repeat risk factor measurements over a period of time.
-
Men and women do not reach the level of risk predicted by the charts for the three age bands until they reach the ages of 49, 59, and 69 years, respectively. The charts will overestimate current risk most in the under 40s. Clinical judgement must be used in deciding on treatment in younger people. However, it should be recognised that blood pressure and cholesterol tend to rise most, and HDL cholesterol to decline most, in younger people already possessing adverse values. Thus their untreated risk at age 49 years is likely to be higher than the projected risk shown on the age-less-than 50 years chart. From aged 70 years the CVD risk, especially for men, is usually ⩾ 20% over 10 years and the charts will underestimate true total CVD risk.
-
These charts (and all other currently available methods of CVD risk prediction) are based on groups of people with untreated blood pressure, total cholesterol, and HDL cholesterol values. In people already receiving antihypertensive therapy in whom a decision is to be made about whether to introduce lipid lowering medication, or vice versa, the charts can only act as a guide. Unless recent pre-treatment risk factor values are available it is generally safest to assume that CVD risk is higher than that predicted by current levels of blood pressure or lipids on treatment.
-
CVD risk is also higher than indicated in the charts for:
those with a family history of premature CVD or stroke (male first degree relatives aged < 55 years and female first degree relatives aged < 65 years) which increases the risk by a factor of approximately 1.3
those with raised triglyceride values (> 1.7 mmol/l)
women with premature menopause
those who are not yet diabetic, but have impaired fasting glycaemia (⩾ 6.1 but < 7.0 mmol/l) or impaired glucose tolerance (two hour glucose in an oral glucose tolerance test ⩾ 7.8 mmol/l but < 11.1 mmol/l)
-
In some ethnic minorities the risk charts underestimate CVD risk, because they have not been validated in these populations. For example, in people originating from the Indian subcontinent it is safest to assume that the CVD risk is higher than predicted from the charts (1.4 times).
-
An individual can be shown on the chart the direction in which his or her risk of CVD can be reduced by changing smoking status, blood pressure, or cholesterol. It should be borne in mind that the estimate of risk is for a group of people with similar risk factors and that within that group there will be considerable inter-individual variation in risk. It should also be pointed out in younger people that the estimated risk will generally not be reached before the age of 50, if their current blood pressure and lipid levels remain unchanged. The charts are primarily to assist in directing intervention to those who typically stand to benefit most.
APPENDIX II
Cardiovascular prevention quality indicators in the new General Medical Services contract
Footnotes
-
Authors affiliationsD Wood, R Wray, British Cardiac Society N Poulter, B Williams, British Hypertension Society M Kirby, V Patel, Diabetes UK P Durrington, J Reckless, HEART UK M Davis, F Sivers, Primary Care Cardiovascular Society J Potter, The Stroke Association
Linked Articles
- Miscellanea
- Miscellanea