Article Text

Navigate this article
Statistics from Altmetric.com
Foreword
In 1961, the publication of the findings of the Framingham study provided the National Institutes of Health (NIH), the USA, and the world at large with a huge return on the initial investment. Identification of the common risk factors fuelling the epidemic of cardiovascular disease (CVD) stimulated a ‘call to arms’ and the initiation of programmes to attack these targets on a national scale. This has led to stunning declines in CVD mortality over the last 40–50 years in North America, Western Europe and other high income countries. Nonetheless, this is not the time for complacency. CVD is by far and away the leading cause of deaths worldwide; the epidemic of CVD in the low and middle income countries is rampant and the alarming increases in obesity and diabetes threaten to reverse or blunt the steady decline in CVD mortality, particularly in younger people. The focus on prevention is as imperative now as it ever has been.
This is the 3rd iteration of the Joint British Societies ( JBS) recommendations for the prevention of cardiovascular disease. Current prevention strategies tend to focus upon patients at relatively short term (10-year) risks and upon specific thresholds for pharmacologic therapies, although there is considerable variability among the different guidelines. This approach is logical and has been successful in directing therapy to those at highest risk who stand to gain the greatest benefit.
A unique aspect of JBS3 is the emphasis upon the lifetime risk of CVD events, so as to encompass a large pool of people in the population who have a lower 10-year risk of a CVD event but who nevertheless have a high lifetime event risk. Such predominantly younger patients and women might be excluded from therapy based upon the ‘high risk strategy’, even though they have a high rate of significantly elevated and modifiable risk factors. Recognition of this ‘continuum of risk’, and the impact of the duration of exposure to risk factors upon future CVD events, is an important concept and offers the opportunity to modify the evolution of CVD.
This consensus statement is clearly written, evidence based, and beautifully illustrated. The JBS3 risk calculator is a novel and exciting tool that can be used to motivate both physicians and patients to tackle the potential scourge of CVD, at a time when overt disease is not present and prevention may exert its greatest impact. The importance of these consensus recommendations and this document will extend beyond the boundaries of the UK and provides an invaluable resource for all physicians and healthcare providers who are involved in the prevention of CVD.
Bernard J Gersh
Professor of Medicine, and Consultant, Division of Cardiovascular Diseases, Mayo Clinic and Mayo Clinic College of Medicine
Executive summary
Despite the improvements in outcomes for cardiovascular disease (CVD) over the last 20 years, it remains the major cause of morbidity and mortality in the population. More patients are surviving their first CVD event and they remain at high risk. Furthermore, levels of certain risk factors such as obesity and diabetes are increasing. More focus on prevention is therefore required.
-
There is clear evidence that evolution of atherosclerosis and clinical events are related to several modifiable risk factors and that lowering levels of these factors results in benefit. Cardiovascular outcome is usually determined by the combination of multiple co-existing risk factors, rather than high levels of a single factor.
-
JBS3 emphasises the need for an integrated approach to CVD prevention across related disease conditions and different organ systems.
-
JBS3 endorses intensive risk factor lowering in patients with established CVD, as well as in those with high risk diseases which cause CVD without the need for estimation of CVD risk. Specific recommendations are made for those diseases resulting from atherosclerosis (coronary disease, stroke, peripheral arterial disease (PAD) and dementia), as well as for risk factors, and are based on recent evidence which shows that broader risk factor treatment to lower levels produces clinical benefit.
-
Current prevention strategies for the population have been based on quantification of absolute short term (10-year risk) and prescription of pharmacological treatments above a threshold. This ‘risk based’ approach has been successful and directs treatment of those at highest absolute risk and who stand to obtain the highest absolute benefit.
-
There is a continuum of CVD risk in the population and most CVD events occur in individuals who are at ‘intermediate’ CVD risk. These individuals would not receive risk factor lowering treatment based on current guidelines (>20% of 10-year CVD risk). Such individuals are more likely to adopt lifestyle risk reduction strategies with communication of their lifetime risk. Conversely, 10-year risk estimates may provide false reassurance over the long term, especially in young individuals and women with high lifetime risk. As cardioprotective drugs have become cheaper and have been shown to be safe and efficacious over the longer term, there is an opportunity to extend their use beyond the current 10-year CVD risk threshold. JBS3 supports such a revaluation of indications for drug treatment which should be based, however, on acceptability, cost effectiveness, and practicality.
-
The major change in JBS3, however, is the recommendation of an approach to risk estimation and management, based not only on short term (10-year) risk, but also on CVD risk over lifetime. Short term absolute risk estimates are heavily dependent on age and gender, so that decisions based on this approach will result in drug prescription to a very large number of older and elderly individuals. Younger subjects and women tend to be excluded, even if they have substantially elevated modifiable risk factors and are consequently at high lifetime risk. Evidence is accumulating that long term exposure to CVD risk factors drives atherogenesis and that early treatment can modify disease evolution and risk of future CVD events. This represents an opportunity for ‘investment’ in future cardiovascular health.
-
A new JBS3 calculator has been designed to identify the sizeable number of individuals in the population who are at low short term risk but at high lifetime risk. Novel metrics such as ‘heart age’ and CVD event-free survival are displayed together with 10-year risk. The calculator is designed to communicate the long term consequences of an individual's lifestyle and associated risk factors and the substantial lowering of CVD risk which can be obtained by early lifestyle changes and, where appropriate, by use of evidence based drug therapies. The JBS3 risk calculator should empower individuals to understand why they should start CVD risk reduction, when they should start, and what they should do. It also emphasises the need for long term maintenance of risk factor lowering to have the greatest influence on CVD risk over lifetime. It will also help clinicians to engage in this important dialogue with their patients.
-
This new approach to risk estimation and management is widely applicable across the UK and internationally.
-
The principles of JBS3 and the widespread use of the JBS3 risk calculator will support the CVD Outcomes Strategy and the NHS Health Check programme in England which invites adults from 40 to 74 years for CVD risk factor assessment.
Recommendations
General recommendations
-
Use JBS3 risk calculator to estimate both 10-year risk and lifetime risk of CVD in all individuals except for those with existing CVD or certain high risk diseases: that is, diabetes age >40 years, patients with chronic kidney disease (CKD) stages 3–5, or familial hypercholesterolaemia (FH).
-
Total cholesterol (TC) and high density lipoprotein (HDL) cholesterol from a non-fasting blood sample should be used for the lipid profile estimate of CVD risk in the JBS3 calculator.
-
Non-HDL cholesterol, measured from a non-fasting blood sample as total cholesterol (TC) minus HDL cholesterol, should be used in preference to low density lipoprotein (LDL) cholesterol as the treatment goal for lipid lowering therapy.
-
Intensive risk factor modification with diet, lifestyle intervention, and pharmacological therapy in patients with existing CVD, without the need for estimation of CVD risk.
-
Intensive risk factor modification with diet, lifestyle intervention, and pharmacological therapy, in individuals at particularly high risk of developing CVD: that is, diabetes age >40 years, patients with CKD stages 3–5, or FH without the need for estimation of CVD risk.
-
Diet, lifestyle intervention, and pharmacological therapy in people at high short term risk. Thresholds for treatment with statins based on 10-year CVD risk will be informed by National Institute for Health and Care Excellence (NICE) guidelines.
-
Diet, lifestyle intervention, and for some people pharmacological therapy in those with increased modifiable lifetime risk, as informed by JBS3 calculator metrics.
Risk model refinement recommendations
-
Use of non-invasive imaging tools to detect subclinical atherosclerosis is not recommended for CVD risk assessment in the primary prevention setting. Utility for selected groups of individuals requires further study.
-
Currently available novel biomarkers do not replace or enhance established methods for CVD risk assessment in the primary prevention setting, but studies are ongoing.
-
Common genetic variants associated with blood lipids and coronary events currently perform less well than phenotype based methods for risk assessment and, except for screening for FH, are not recommended for CVD risk assessment in the primary prevention setting.
Lifestyle recommendations
Smoking
-
Professional support on how to stop smoking should be given at every available opportunity, with provision of self-help material and referral to more intensive support, for example, stop smoking services.
-
The JBS3 risk calculator emphasises the benefits for early smoking cessation and the diminishing but still substantial returns from quitting at an older age.
-
Patients should be offered behavioural counselling, group therapy, pharmacotherapy or a combination of treatments that have been proven to be effective.
-
Nicotine replacement therapy (NRT), varenicline or bupropion should be offered to people who are planning to stop smoking as part of an abstinent contingent treatment in which the smoker makes a commitment to stop smoking on or before a particular date (target stop date).
-
People who have heart or respiratory diseases, and those who live with them, should be made aware of the risks of both active and passive smoking (secondhand smoke (SHS)).
-
For specific recommendations on quitting smoking in pregnancy and following childbirth, see NICE public health guidance 26.
-
The importance of stopping smoking during pregnancy should be emphasised and guidance from NICE followed.1
Diet
Professional support to consume a diet associated with the lowest cardiovascular risk should be provided based on the following principles:
-
Intake of saturated fat to <10% of total fat intake (preferably in lean meat and low fat dairy products)
-
Replace saturated fat with polyunsaturated fat where possible
-
Consume five portions per day of fruit and vegetables
-
Consume at least two servings of fish (preferably oily) per week
-
Consider regular consumption of whole grains and nuts
-
Keep salt consumption to <6 g/day
-
Limit alcohol intake to <21 units per week for men and <14 units per week for women
-
Avoid/reduce consumption of:
-
Processed meats or commercially produced foods which tend to be high in salt and trans fatty acids (TFA)
-
Refined carbohydrates, such as white bread, processed cereals
-
Sugar sweetened beverages
-
Calorie rich, but nutritionally poor, snacks such as sweets, cakes, and crisps
-
-
Children and young people should be supported to consume a diet based on the same principles.
Physical activity and exercise
-
An increase in overall levels of sustained physical activity and avoidance of prolonged sedentary behaviour are important for reduction of CVD risk.
-
Emphasise walking, cycling, and other aerobic physical daily activities, at moderate intensity, as part of an active lifestyle, for at least 150 min per week in bouts of ≥10 min or 75 min per week of vigorous physical activity, or a combination of the two.
-
Muscle strengthening activities performed on at least two occasions per week.
Exercise training
General population and those at low to moderate risk of CVD:
-
Exercise, incorporating a warm up and cool down period, should be performed at moderate to high intensity two to three times per week for 30–40 min each time.
-
The mode of exercise should be aerobic and, where possible, continuous allowing for a steady progression in effort, for example, walking programmes, cycling, jogging, swimming.
-
The time spent exercise training contributes to meeting the 150 min per week physical activity recommendation.
Patients with established CVD and those considered at higher risk of CVD:
-
A more structured approach is needed in managing patients, and in all cases assessment and specific goal setting, with risk stratification, delivered by professionals skilled in health related exercise is preferable.
-
Increase in exercise on referral with community based exercise initiatives are recommended for patients at risk of CVD.
-
Cardiac rehabilitation programmes are recommended for patients with established CVD and in those following a CVD event.
Childhood and adult obesity recommendations
-
Multidisciplinary approaches to obesity management in children and young people are required with a ‘lifetime risk’ message. These may include interventions during the early postpartum period as well as regular monitoring of childhood weight and family counselling.
-
With appropriate training, all healthcare professions should be able to Ask and Assess adiposity and Advise appropriate adult patients on evidence based ways to target weight change.
Lipid recommendations
-
Non-fasting blood samples should be taken to measure TC and HDL cholesterol (HDL-c). The JBS3 risk calculator enables entry of these two measures and it is expected that non-HDL-c (TC minus HDL-c=non-HDL-c) will replace LDL-c in clinical practice as well as in clinical trials.
-
All high risk people should receive professional lifestyle support to reduce TC and LDL-c, raise HDL-c, and lower triglycerides to reduce their CVD risk.
-
Cholesterol lowering drug therapy is recommended in:
-
Patients with established CVD
-
Individuals at high risk of CVD: diabetes age >40 years, patients with CKD stages 3–5, or FH
-
Individuals with high 10-year CVD risk (threshold to be defined by NICE guidance)
-
Individuals with high lifetime CVD risk estimated from heart age and other JBS3 calculator metrics, in whom lifestyle changes alone are considered insufficient by the physician and person concerned
-
-
Statins are recommended as they are highly effective at reducing CVD events with evidence of benefit to LDL-c levels <2 mmol/L which, justifies intensive non-HDL-c lowering.
-
Statins are safe, with trial evidence showing no effects on non-cardiovascular mortality or cancer. There is a small increase in risk of developing diabetes but the benefits of cholesterol lowering greatly exceed any risk associated with diabetes. If statin intolerance develops a stepwise strategy involving switching agents and re-dosing is recommended.
-
Despite low HDL-c values contributing to CVD risk, drug therapy to raise HDL-c has not been shown to reduce CVD risk and is not currently indicated.
Blood pressure recommendations
-
Hypertension should be suspected when office blood pressure (BP) is persistently elevated: that is, ≥140/90 mm Hg.
-
Ambulatory BP monitoring (ABPM) is recommended to confirm the diagnosis of hypertension (daytime mean ABPM ≥135/85 mm Hg).
-
All high risk people should receive professional lifestyle support to reduce their BP which may avoid the need for, or complement the use of, drug therapy for hypertension and reduce CVD risk.
-
People with an office BP >160/100 mm Hg, a 24 h daytime ABPM average or home ABPM average of >150/95 mm Hg (stage 2 hypertension) should be offered pharmacological therapy to reduce BP.
-
People with an office BP >140/90 mm Hg, but <160/100 mm Hg, a 24 h daytime ABPM average or home ABPM average of >135/85 mm Hg (stage 1 hypertension) and established CVD, hypertensive target organ damage, diabetes, CKD, or a high lifetime risk assessed by JBS3 calculator, should be offered pharmacological therapy to reduce BP.
-
People with stage 1 hypertension without established CVD, hypertensive target organ damage, diabetes, CKD, or a significant increase in lifetime risk assessed by JBS3 calculator, should receive advice on lifestyle interventions and be scheduled for annual BP and lifetime risk assessment to inform future need for therapy.
-
Pharmacological treatment for patients with hypertension should follow the current NICE guidance (CG127) treatment algorithm:
-
Patients <55 years of age should be offered an angiotensin converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) as preferred initial therapy
-
Patients aged ≥55 years should be offered a calcium channel blocker (CCB) as preferred initial therapy
-
-
Combinations of drug treatment are usually required to optimise BP control for the majority of patients.
-
Thiazide-like diuretics are an alternative to CCBs and are preferred for patients intolerant of CCBs, or with heart failure or at high risk of heart failure.
-
β-blockers are not preferred, unless there are specific indications for use: that is, in patients with symptomatic angina or chronic heart failure.
-
For pregnant women or women planning pregnancy, the recommendations of the NICE guideline CG107 Hypertension in pregnancy should be followed.
Established CVD recommendations
-
For all patients with established CVD, an intensive approach to risk factor modification is recommended, including lifestyle intervention and the use of pharmacological therapy for secondary prevention based on NICE, Scottish Intercollegiate Guidelines Network (SIGN), and European Society of Cardiology (ESC) guidance.
-
Statins should be prescribed with a ‘lower is better’ approach to achieve values of at least <2.5 mmol/L for non-HDL-c (equivalent to <1.8 mmol/L for LDL-c).
Post-myocardial infarction recommendations
Antiplatelet therapy
-
Antiplatelet therapy with low dose aspirin (75–100 mg) is recommended indefinitely after myocardial infarction (MI).
-
In patients with true aspirin intolerance, clopidogrel 75 mg should be considered as an alternative.
-
More potent antiplatelet agents (such as prasugrel or ticagrelor) are recommended as dual antiplatelet therapy in combination with aspirin in patients with acute coronary syndromes.
-
Dual antiplatelet therapy is recommended for up to 12 months post-MI with a minimum of:
-
1 month for patients also receiving a bare metal stent
-
6 months for patients also receiving a drug eluting stent
-
Lipid lowering therapy
-
Intensive statin therapy is recommended in all patients following MI, in the absence of a contraindication or intolerance, irrespective of initial cholesterol values.
-
Statins should be prescribed with a ‘lower is better’ approach to achieve values of at least <2.5 mmol/L for non-HDL-c (equivalent to <1.8 mmol/L for LDL-c).
β-blockers, ACE inhibitors/ARBs, aldosterone antagonists
-
Use of β-blockers, ACE inhibitors/ARBs, and aldosterone antagonists post-MI is recommended in line with existing NICE, SIGN, and ESC guidance.
Stroke recommendations
BP lowering
-
Optimal BP levels on treatment for patients with established cerebrovascular disease are unclear, but levels of <130/80 mm Hg are recommended. Care should be taken not to reduce rapidly BP in those with significant carotid/vertebrobasilar stenosis. Treatment should usually be started within 1–2 weeks of the acute event.
Lipid lowering
-
Statin therapy is recommended for patients with ischaemic stroke. Its introduction should be delayed for 2 weeks post-stroke, but there is no need to discontinue statins in patients already on therapy.
-
Statin therapy should be avoided in individuals with a history of haemorrhagic stroke, particularly in those with inadequately controlled hypertension unless there is a compelling indication, such as concomitant coronary artery disease.
Antithrombotic therapy
In the absence of atrial fibrillation (AF), recommendations for patients who have had an ischaemic stroke follow the current NICE guidelines:2
-
After acute ischaemic stroke, patients should initially receive 300 mg of aspirin daily for 2 weeks, then be changed to long term clopidogrel 75 mg daily. For patients who have a contraindication or intolerance to clopidogrel, modified release dipyridamole plus aspirin is an alternative. For people who have a contraindication or intolerance to both clopidogrel and aspirin, modified release dipyridamole alone is recommended.
-
For patients with transient ischaemic attacks (TIAs), modified release dipyridamole 200 mg twice daily plus aspirin 75–150 mg daily is an alternative treatment option to clopidogrel. For people who have a contraindication or intolerance to aspirin, modified release dipyridamole alone is an alternative treatment option.
In the presence of AF (valvular or non-valvular), patients with a TIA or ischaemic stroke:
-
Should be anticoagulated with warfarin to achieve a target international normalised ratio (INR) on warfarin of 2.5 (range 2.0–3.0) or with one of the new oral anticoagulant agents.
-
Anticoagulation should not be started until brain imaging has excluded haemorrhage, and not usually until 14 days have passed from the onset of a disabling ischaemic stroke.
-
Anticoagulation should not be used for patients in sinus rhythm unless a cardiac source of embolism has been identified.
Peripheral arterial disease recommendations
-
Patients with PAD should have intensive risk factor modification including intensive statin therapy and BP managed in line with NICE guidelines.
-
Patients with PAD should be screened for diabetes and CKD.
-
Patients with PAD should be encouraged to exercise, and supervised exercise programmes should be available for appropriate patients.
-
Patients with PAD should be started on an antiplatelet agent with clopidogrel being the agent of first choice.
Diabetes mellitus recommendations
Type 1 diabetes mellitus
All people with type 1 diabetes should receive professional lifestyle advice. Statins should be offered in type 1 diabetes for the following categories:
-
All patients with type 1 diabetes aged ≥50 years.
-
The majority aged 40–50 years, unless short duration of diabetes (<5 years) and absence of other CVD risk factors.
-
Those aged 30–40 years with any of the following features: long duration of diabetes (20 years) and poor control (HbA1c >9% (75 mmol/mol)), persistent albuminuria (>30 mg/day) or estimated glomerular filtration rate (eGFR) <60 mL/min, proliferative retinopathy, treated hypertension, current smoking, autonomic neuropathy, TC >5 mL/min with reduced HDL-c (<1 mmol/L for males and <1.2 mmol/L for females), or central obesity, or with a family history of premature CVD (<50 years).
-
Those aged 18–30 years should receive statins if persistent albuminuria is detected, with caution exercised in women of childbearing potential.
Blood pressure
-
This should be maintained at 130/80 mm Hg and consideration of lower values (120/75–80 mm Hg) as a target in younger type 1 diabetes (aged <40 years) with persistent microalbuminuria.
-
ACE inhibitors should be the drugs of first choice.
Aspirin
-
There is no role for aspirin in primary prevention of CVD in type 1 diabetes.
Glycaemic control
-
Intensive Glycaemic control to achieve and maintain an HbA1c of 48–58 mmol/L, should be aimed for.
Type 2 diabetes mellitus
All people with type 2 diabetes should receive professional lifestyle advice.
Lipid lowering
-
Statin therapy remains the best and only effective lipid modifying agent to lower CVD risk in type 2 diabetes.
-
Statin therapy is recommended for all patients with type 2 diabetes above age 40, irrespective of cholesterol value.
-
Intensive statin treatment is recommended for diabetes patients with existing CVD, and those with persistent proteinuria or CKD with eGFR 30–60 mL/min. Intensive statin treatment is also recommended for patients who do not achieve non-HDL-c targets.
-
Statins should also considered for patients with type 2 diabetes under 40 years of age if there is persistent albuminuria, eGFR <60 mL/min, proliferative retinopathy, treated high BP (HBP), or autonomic neuropathy.
-
Fibrates, used as monotherapy or in combination therapy, have not been shown to provide overall cardiovascular benefit in type 2 diabetes, and should not be prescribed for CVD risk reduction.
-
Fibrates show some promise in prevention or treatment of retinopathy in type 2 diabetes in a manner independent of lipid lowering action.
Blood pressure
-
Lowering systolic BP in the majority of type 2 diabetes patients to ∼130 mm Hg appears beneficial. Pursuing lower targets does not reduce coronary event rates, although stroke incidence may be modified.
-
The degree of BP appears to be the critical aspect in reducing CVD risk rather than the method or agent used to lower BP, although renin–angiotensin system blockade appears to reduce overall mortality.
-
The ACE inhibitor and ARBs reduce development and progression of albuminuria and reduce major renal outcomes.
-
However, dual blockade of the renin–angiotensin system, with ACE inhibitors, ARB or direct renin inhibitors in any combination, is associated with worsening of cardiorenal outcomes and should not be used.
Glycaemic control
-
The effect of intensive glucose lowering cannot be conclusively quantified, but trial results suggest a 10–15% reduction in CVD events for ∼0.9% (10 mmol/mol) reduction in HbA1c.
-
Recent trial findings and observational studies have noted that younger onset type 2 diabetes has an especially poor prognosis, requiring earlier intensive glucose lowering and reduction of all CVD risk factors, whereas intensive glucose lowering may not be appropriate in older patients and/or those with existing CVD.
-
The CVD effects of intensive glucose lowering are less than can be achieved with statin therapy or BP lowering therapy.
Aspirin
-
Low dose aspirin is not recommended for primary prevention of CVD in patients with type 2 diabetes.
Chronic kidney disease recommendations
-
In CKD, the JBS3 risk calculator can be used to highlight the increased CVD risk and to guide appropriate risk factor modification.
Blood pressure
-
In adults with stages 3–5 CKD, with or without diabetes, BP should be treated to maintain systolic BP <140 mm Hg and diastolic BP <90 mm Hg.
-
In adults with CKD, with or without diabetes, in whom urinary albumin excretion >30 mg/day (equivalent to an albumin: creatinine ratio (ACR) of 3 mg/mmol), these targets should be reduced to systolic <130 mm Hg and diastolic <80 mm Hg.
-
All antihypertensive agents are effective in adults with stages 3–5 CKD. ACE inhibitors or ARBs should be included in the antihypertensive regimen, particularly in people with albuminuria >30 mg/day (equivalent to an ACR of 3 mg/mmol).
Lipids
-
In adults with stages 3–5 CKD, lipid lowering therapy with statins should be considered in all patients.
Aspirin
-
Routine use of aspirin is not recommended for primary prevention in CKD.
Chronic inflammatory disease recommendations
-
There is clear evidence of heightened CVD risk in patients with rheumatoid arthritis (RA), as summarised in a recent European League Against Rheumatism (EULAR) consensus document.
-
The JBS3 risk calculator now incorporates the appropriate multiplier for CVD risk, based on the presence of RA.
-
Intensive management of traditional CVD risk factors should be undertaken in patients with RA, taking into account their CVD risk score.
-
Optimisation of inflammation suppression with disease modifying antirheumatic drugs may also help reduce CVD risk.
-
CVD risk may be lowered by use of the minimum effective glucocorticoid dose for the shortest possible time.
-
Where anti-inflammatory drugs are indicated for symptoms in patients with an average gastroduodenal damage risk, the use of a conventional non-steroidal anti-inflammatory drug (NSAID) with a gastroprotective agent is preferable to use of a cyclooxygenase-2 (COX-2) selective inhibitor.
-
Clinical judgement may be used to determine whether a risk multiplier should be applied to patients with other autoimmune conditions.
Chronic obstructive sleep apnoea/hypopnoea recommendations
-
Lifestyle advice to support weight loss should be offered to all patients with a diagnosis of obstructive sleep apnoea/hypopnoea syndrome (OSAHS) who are obese or overweight.
-
Patients with significant daytime sleepiness and confirmed OSAHS should be offered continuous positive airway pressure (CPAP) treatment.
-
CVD risk factors should be assessed using the JBS3 risk calculator and managed according to JBS3 recommendations.
Implementation recommendations
-
All patients with established CVD should have access to evidence based prevention/rehabilitation programmes addressing lifestyle, risk factor management, and adherence to drug therapies.
-
A national screening programme for ascertainment of FH cases should be supported, including cascade screening and specialist referral.
-
The JBS3 approach linked to NHS Health Checks should be used to promote better uptake of lifestyle improvements (and where required drug therapy) in primary care. This should include development of a CVD prevention strategy for individuals who, despite low short term risk, are found to have a high lifetime risk of developing CVD and its complications.
Section 1: Cardiovascular disease prevention
1.1 Introduction and aims
This third iteration of the Joint British Societies’ Consensus Recommendations (JBS3) on prevention of CVD represents an evolution in CVD prevention. The JBS (see appendix 2) first produced guidelines in 1998,3 that emphasised the need for a common, coordinated, and integrated approach to the prevention of CVD and introduced the now widely used risk prediction charts. These remained a key feature of JBS2,4 which extended the evidence base for CVD prevention and highlighted the importance of managing high risk individuals in a manner similar to those with established CVD. It provided guidance on the treatment thresholds in asymptomatic patients with multiple risk factors based on a 20% 10-year risk of developing established CVD, and also stressing the importance of treating individuals with a particularly elevated single risk factor.
Considerable new evidence has emerged since JBS2, as have new ways of cross-silo working to address broader issues of CVD risk prevention. In addition, some concerns have been raised that JBS2 fails to fully address the potential CVD risk of young patients, especially females, where a low short term risk masks significant lifetime risk and where substantial healthcare and economic gains may be achieved by early intervention.
Improvements in cardiovascular care across the UK, most clearly manifest through implementation of the National Service Framework in England, published in 2000, have resulted in a significant reduction in the incidence of, and mortality from, CVD. These improvements are a consequence of many factors including public health improvement, better acute and long term care combined with better engagement of primary care in prevention and management of CVD. The IMPACT model evaluated the reasons for the declining coronary heart disease (CHD) mortality in England between 2000 and 2007 and similar analyses have been undertaken for Scotland and Northern Ireland.5 ,6 For England the model explained about 86% of the mortality fall, with 34% of this due to decreases in the major cardiovascular risk factors in the population, with reductions in smoking and cholesterol, and improved physical activity levels. The biggest contributor was falling BP in the population not on antihypertensive medication. These beneficial risk factor trends were partly negated by increases in body mass index (BMI) and diabetes which blunted the mortality decline. The remaining 52% of the mortality fall was explained by medical treatments with lipid reduction, angina management, and secondary prevention making the largest contributions.
Despite impressive progress, there is much still to be achieved in the prevention and management of cardiovascular care, with no room for complacency. There remains significant geographic variation in cardiovascular mortality as well as by social deprivation score. Acute cardiovascular care is expensive and with life expectancy continuing to rise, the prevalence of CVD continues to increase. The lifesaving gains made through national investment in acute cardiovascular care over more than a decade need to be complemented by a modern and integrated approach to cardiovascular prevention. In the ASPIRE-2-PREVENT national survey, only half of all patients with coronary disease participated in such programmes.7
CVD represents a single family of diseases, linked by a common pathology of atherosclerosis with common risk factors, which merits a coordinated and integrated approach to prevention and management, consistent with the aspirations of the CVD Outcomes Strategy published in 2013.
JBS3 has been developed, primarily for healthcare professionals, to facilitate informed communication with individuals about their personal cardiovascular risk and the benefits of its early modification. It represents an evidence based consensus of the JBS3 Professional Societies which synthesises existing information, reviews the strength of new evidence, and fills the gaps in managing cardiovascular prevention. It emphasises the importance of identifying cardiovascular risk at a young age, thereby providing the greatest opportunity to maximise the benefits of risk factor modification. It highlights the importance of lifestyle intervention and empowering individuals to make early lifestyle adjustments in order to reap potential long term gains, as well as the importance of an integrated, coordinated approach to cardiovascular prevention. Key scientific literature which informs the recommendations is referenced and, where available, JBS3 supports the gradation of evidence based recommendations within referenced guidelines.
JBS3 strengthens the recommendations for patients with existing CVD and those at known high risk of its development, all of whom require professionally guided lifestyle intervention, risk factor and therapeutic management to reduce their risk of disease progression, the need for revascularisation, and to prevent recurrent events and ultimately increase life expectancy.
In particular, JBS3 recognises the arbitrary nature of treatment thresholds, supporting the need for intensive risk factor modification in those with established CVD or at particularly high risk of developing it.
Importantly, it also presents cardiovascular risk for those without existing CVD, or at high risk of its development, as a continuum by utilising the concept of lifetime risk linked to a new, clinically useful, risk calculator to inform the benefits of personalised, timely, risk factor modification. By taking a lifetime approach to cardiovascular risk, people who are apparently healthy can see their cardiovascular age (or ‘heart age’) today in relation to their chronological age, and their lifetime risk, which should encourage adoption of a healthier lifestyle. Physicians should monitor such people more closely and have a lower threshold for intervention, initially through professionally guided lifestyle interventions and, where appropriate, with drug therapies to reduce total CVD risk over the long term.
Given the enormous burden and economic consequences of CVD, this also provides a basis for healthcare providers to benefit from a national prevention framework with locally delivered services and care, linking directly with the NHS Health Check programme in England. The JBS3 risk calculator, which will form a pivotal component of NHS Health Checks, will facilitate discussion between healthcare professionals and individuals about their cardiovascular risk, empowering individuals to make informed personal decisions about how best to modify this and the cumulative benefits of timely intervention.
It is not the role of JBS3 to undertake a cost effectiveness analysis of risk factor interventions, especially when these are based on arbitrary thresholds which challenge the concept of individualised care. However, it is important that JBS3 informs the balance between the clinical benefits of lifestyle only versus additional pharmacological intervention, and provides the necessary tools for health economists and public health professionals to make these value judgements. As such, JBS3 supports the updated guidance provided in the NICE lipid modification guideline, due to be published in July 2014.
Prevention of CVD is a rapidly evolving area. JBS3 had recognised this by ‘horizon scanning’ potential developments to allow future modification of the risk calculator as new evidence emerges, and highlights new areas for research interest. The implementation of the JBS3 recommendations has the potential to realise long term healthcare benefits from timely, personalised risk factor assessment and intervention.
The full list of contributors to the JBS3 is given in appendix 2. The project was managed under the auspices of the British Cardiovascular Society and supported by the British Heart Foundation.
1.2 Principles of cardiovascular prevention
Since 1993, death rates from CVD have fallen >50% in England, beating the target set by the National Service Framework in 2000. Despite this, CVD remains the major cause of morbidity and mortality in the population. More patients are surviving their initial CVD event and remain at high risk, and furthermore the prevalence of several risk factors, such as obesity and diabetes, are increasing in the population. Treatment of established disease is very expensive and better CVD prevention approaches are crucial. This applies not only to developed countries but, increasingly, to the developing world, where a rapid deterioration in risk profiles in the population, particularly in the young, threatens to overwhelm healthcare systems in the future. JBS3 aims to guide practitioners towards strategies that reduce further the risk of CVD events in patients, as well as to develop a more effective prevention strategy for the population. In England, this aligns with the agenda of the CVD Outcomes Strategy, which was published in 2013.8
CVD is a diffuse vascular disease which develops over decades. Its evolution and clinical consequences are causally related to several modifiable (and in some cases preventable) risk factors. CVD events are rarely determined by elevation of a single risk factor, and for most individuals multiple coexisting risk factors combine to increase the risk of future CVD events. The INTERHEART study, which was a case–controlled study of more than 15 000 cases from 52 countries, suggested that nine easily measurable risk factors accounted for more than 90% of MIs.9
In 2005, JBS2 recommended estimation of the absolute risk a CVD event and advised that decisions regarding pharmacological treatment be based on risk levels over 10 years, not on previously used targets for individual risk factors. This approach, which treats risk, not risk factors, has been adopted by the majority of national guidelines, including those published recently by the American Heart Association/American College of Cardiology (AHA/ACC).10
JBS3 recommends a new approach to CVD prevention which builds on JBS2. It is not only based on 10-year absolute CVD risk, but also on CVD risk over an individual’s lifetime. This provides a framework for clinical decision making on both prescription of pharmacological therapy to those at ‘high risk’, but also for early lifestyle interventions (and where required pharmacological therapy) to modify the evolution of CVD and lifetime risk. A new risk calculator has been developed (see below), and figure 1 illustrates its use in the new risk management algorithm.

JBS3 flowchart. CVD, cardiovascular disease; JBS, Joint British Societies.
1.2.1 Established CVD
Patients with existing CVD, with or without previous clinical events, have the highest level of risk and benefit from intensive lowering of their risk factors, without the need for estimation of risk levels. CVD affects several vascular beds and may have a variety of clinical presentations. There is increasing evidence that the principles of treatment should be similar, regardless of clinical presentation, with risk factor lowering resulting in reduction of CVD events in different territories. For example, statin use in patients who have sustained a stroke results in substantial lowering of future MI rates. JBS3 therefore includes recommendations for the management of patients with PAD and cerebrovascular disease, in addition to clinical cardiac presentations. Individuals and patients without clinical CVD may also be at high risk because of their risk factor profiles or comorbidities. JBS3 defines categories of patients, for example, diabetes, whose short term (10-year) and lifetime risk levels are sufficiently high to mandate pharmacological risk factor lowering without prior risk assessment.
1.2.2 Risk assessment for CVD prevention in the population
Population studies and randomised clinical trials have shown that a given degree of cholesterol lowering produces the same relative reduction in CVD risk regardless of the absolute risk of the group being targeted, so that those at high absolute risk experience the greatest absolute benefit.11 This occurs regardless of the precise combination of risk factors that determines the overall risk level in an individual. For example, statins appear to be as effective in those with high BP or diabetes as in individuals with elevated cholesterol concentrations. The advantage of this ‘risk based’ approach is that it directs preventative treatments to those who stand to gain the most individually. In current UK guidance, pharmacological treatments are recommended to lower cholesterol values (and where appropriate BP) in those whose 10-year absolute CVD risk exceeds a threshold of 20%. This strategy of identification and targeting of individuals at high 10-year risk was developed, however, at a time when effective drugs such as statins were under patent protection (and therefore expensive) and had uncertain long term safety and efficacy. While it has been fit for purpose for over a decade, several developments have prompted a re-evaluation. In the last 5 years, the cost of potent statins has fallen sharply and this has been accompanied by accumulating evidence of their long term safety and benefit. There is also increasing appreciation that the widely used risk equations can accurately assign a group risk (ie, observed group event rates are close to event rates predicted by the risk model), but are less good at distinguishing which individuals will or will not experience a CVD event in the future. The apparent paradox of accurate risk stratification but poor disease discrimination is explained by the fact that a high proportion of events occur among the ‘intermediate risk majority’. Exposure to risk factors is almost universal and factors such as BP and cholesterol have an approximately normal distribution and a log linear association with CVD risk. Thus, individuals with average risk factor levels contribute a substantial proportion of all CVD events. Setting a high threshold for intervention thus misses many people who might benefit and reduces the population impact. Reducing the burden of CVD by broadening the eligibility for pharmacological intervention therefore seems appropriate.
One approach would be to reduce the 10-year absolute CVD risk threshold from the current 20% level. This apparently straightforward solution has been adopted by the latest AHA/ACC guidance which advocates a lowering of the 10-year absolute CVD risk threshold for statin treatment to 7.5% for both men and women.12 Despite a rigorous evidence gathering process, these recommendations have been highly controversial and they have substantial implications for healthcare providers. For example, it has been estimated that the new guidance could result in 33 million adults in the USA being eligible for statins for primary prevention and would apply to approximately 920 million people worldwide were this approach to be adopted internationally. In the UK, the current threshold of 20% already makes around half of all men of >50 years, without clinical CVD, eligible for statins. Adoption of the new US recommended threshold of 7.5% in the UK would result in the great majority of men and a substantial proportion of women >50 years being eligible for preventative use of statins.
1.2.3 Age based approach
One consequence of such a major reduction in threshold for pharmacological intervention is that, beyond a certain age, such a large proportion of the population would be included that estimation of risk levels becomes redundant. A potential alternative approach would be to use an age threshold, for example, 50 years for men, 55 years for women, as the basis for prescription of drugs, without formal estimate of absolute CVD risk. This might involve a statin alone or prescription of multicomponent treatment, for example, a ‘polypill’, aimed at reduction of several CVD risk factors. Both risk stratification with a lower treatment threshold, and an age based selection approach, would greatly expand the indication for drug prescription in the elderly, some of whom may not have modifiable risk factors. The cost effectiveness, acceptability, and implementation challenges of these approaches have yet to be evaluated fully. Importantly, the preferences of people who might be the recipients of drug therapy need to be determined.
1.2.4 Lifetime risk for CVD
Age and gender, which are not modifiable, are such powerful determinants of absolute CVD risk over the relatively short 10-year period, that individuals only cross the pre-set threshold of risk (currently 20%) that mandates drug treatment at an older age, despite having important modifiable CVD risk factors from much earlier in life. In the USA, it has been estimated that up to half of the adult population (predominantly young individuals and women) have a low 10-year CVD risk (<10%), but nevertheless have a high risk of a future event (>39%) over their lifetime.13 With the current approach to risk stratification, such individuals do not get effective risk factor reduction until late in the evolution of their disease, potentially missing the opportunity to influence favourably CVD evolution. Recent risk factor guidelines have attempted to overcome this important problem by ‘extrapolating risk from elderly patients back to younger patients’ but these projections are not easy to understand and are subject to many assumptions.14 There is considerable scope for improvement in the communication of CVD risk to patients and the public.
Most surveys suggest that the majority of the public underestimate their lifetime risk of developing and dying of CVD, considering cancer to be a greater threat despite robust evidence to the contrary.
1.2.5 JBS3 lifetime risk approach
A key change in the new JBS3 Guidelines is the adoption of a ‘lifetime risk’ approach to assess and communicate CVD risk, in addition to 10-year absolute risk estimates. This change is based upon several lines of evidence. Although most CVD events occur after the age of 50 years, the atherosclerotic process begins many years earlier, often from the first decade of life. Studies have confirmed a steady increase in the presence of atherosclerosis with age in individuals dying from non-cardiac causes.15 Exposure to CVD risk factors occurs from early life and this has been shown to promote the progression of this long preclinical phase of arterial disease. In large observational trials, levels of classical CVD risk factors in adolescents (including LDL-c, BMI, smoking, and BP) have been associated with increased carotid intima–medial thickness measurements in adulthood, a marker of emerging arterial disease. The epidemic of obesity and the resulting increase in type 2 diabetes in the young is likely to accelerate disease progression and is predicted to have a substantial adverse impact on the prevalence of CVD in the population over the next 20 years.16
The emergence of CVD appears to be related to long term and cumulative exposure to causal and modifiable risk factors. The Framingham Heart study examined the relationship between CVD risk profiles at the age of 50 years in men and women and the risk of subsequent CVD events, and showed a large difference in outcomes dependent on risk profiles at this age.17 This emphasised the importance of the interaction between risk factors and the arterial wall in early life, suggesting that prevention efforts need to begin earlier. The importance of this risk factor exposure for future CVD was confirmed in a meta-analysis of studies which included more than a quarter of a million men and women, and showed a strong influence of CVD risk factors on lifetime risk of CVD.18 This suggests that there is an opportunity to modify the evolution of disease by earlier intervention.
All studies on the impact of CVD risk factors in the young and the potential benefits of early treatments have been observational and use surrogate measures of CVD. Prospective randomised trials to evaluate the impact of risk factor lowering from a young age on CVD event rates in later life would need to be very long and are not feasible. Indirect evidence from genetic studies, however, and more direct evidence from intervention trials support the concept that a longer period of cholesterol lowering (and other risk factor lowering) could leverage larger reductions in later CVD risk. The Atherosclerosis Risk In Communities (ARIC) study reported that a rare genetic variant in the population resulted in lower PCSK9 values (now an important target for drug treatment), with 28% lowering of lifetime LDL-c concentrations.19 This was associated with an 88% reduction in future CVD events.
More recent work has confirmed that genetic variants which are associated with lower LDL-c values over life are associated with substantially better outcomes than those which can be achieved by equivalent LDL-c lowering with statins in later life.20 FH is perhaps the best example of a monogenic disorder which elevates a causal risk factor, LDL-c, and which results in rapid early manifestations of atherosclerosis and premature CVD morbidity and mortality. In this context, the concept of statin treatment from a young age to reduce lifetime risk is already universally accepted. The benefits of early statin use have been shown on progression of carotid intima–media thickness (cIMT), even in prepubertal children.
Smoking is a further example of lifetime cumulative damage related to exposure. Smoking from age 35–44 years results in approximately one decade loss in life expectancy. Stopping smoking from this age ‘recovers’ approximately 90% of this lost decade but the survival benefit decreases progressively the later smoking cessation is achieved.21 Reduction in exposure to risk factors by CVD prevention efforts in younger individuals is thus an important opportunity for lifetime CVD risk reduction.
CVD risk over lifetime can be estimated and takes into account both risk from CVD and competing diseases such as cancer. As with 10-year absolute risk levels, lifetime risk estimates represent an average derived from large cohorts, and thus, caution must be applied for their use with individual patients. Nevertheless, lifetime risk is a novel way of communicating risk to individuals in a clinical setting.
The JBS3 risk calculator with its range of measures and communication tools, aims to empower patients and the public to make appropriate decisions about their lifestyle and drug treatments based on a better understanding of their personal CVD risks. It addresses three key questions:
-
Why should I start CVD risk reduction?
-
When should I start?
-
What should I do?
The details of the new calculator are provided in the Risk Calculator section, together with the novel metrics for communication and illustrative clinical cases. ‘Heart age’ is calculated by estimating the age of someone of the same gender and ethnicity, and with the same annual risk of an event, but with all other risk factors at their ‘optimal’ levels. Heart age is thus a measure of both relative and absolute risk and is easily understood. An ‘old’ heart age provides motivation to individuals to consider what they might do to bring their heart age back to their real chronological age, thus taking responsibility for their own future health. The age by which an individual might expect, with their current risk profile, to sustain their first CVD event is also presented and represents ‘event-free’ survival. The impact of risk factor reduction, both alone and in combination, on these key measures can be estimated. Several graphic presentations have been developed to facilitate communication with patients of different levels of sophistication. All, however, demonstrate a number of key messages. Firstly, the impact of traditional risk factors such as BP, smoking, and cholesterol on lifetime CVD outcome is strongly reinforced. Even a single major risk factor from early life is associated with substantially increased lifetime risk for CVD. It is clear that even a relatively low risk factor burden over a long period has an important impact on future CVD outcomes. Furthermore, the lifetime benefits of even small reductions in risk factors, when introduced at an early age, are shown. The calculator also demonstrates, for the individual's ‘risk profile’, how delay in initiating risk factor reduction (eg, smoking cessation) greatly reduces the lifetime benefits. It also shows that, for most interventions, it is never too late to obtain some benefit. For the individual, it is possible to calculate the age at which the initiation of risk factor modification provides the greatest lifetime benefit and, for the healthcare provider and/or doctor, the balance of clinical versus cost effectiveness of treatments at different ages can be estimated. This type of mathematical modelling addresses the important issue of when best to start drug treatment from both a clinical and economic perspective.
The concept of projecting CVD risk over lifetime has been incorporated in previous national CVD guidelines (eg, New Zealand) and those for other diseases, for example, respiratory disease using lung age.22 ,23 While this approach may still be novel for the medical community, it has been applied by the insurance industry for many years to determine appropriate levels of insurance premiums. They have long understood that the excess morbidity and mortality associated with most CVD risk factors increases with duration of exposure, and that the benefits of interventions depend on the age of initiation of treatment. Lifetime risk measurement is an adjunct to the estimation of 10-year absolute risk levels. It is not intended primarily as a guide to decisions about drug initiation, but rather as a way of allowing an individual to understand the lifetime consequences associated with their current lifestyle/risk factors, and the substantial opportunity to reduce/delay future CVD events by early appropriate lifestyle changes and drug treatments.
Using the JBS3 risk calculator in practice readily demonstrates a number of key points:
-
With current behaviour, individuals have accumulated much of their CVD risk before treatment has started.
-
Risk factors combine to determine CVD risk, supporting the global risk factor approach rather than concentrating on a single risk factor.
-
‘Event free life years’ can be gained by multiple early interventions and that the benefit of each can be easily demonstrated for an individual's risk factor profile.
-
Delay in instituting appropriate risk factor lowering can greatly reduce the ‘lifetime gains’, so that an optimal age for intervention can be estimated for an individual.
-
There are striking health benefits from achieving ‘optimal CVD risk factors’ from early in life.
The JBS3 algorithm for CVD risk assessment and management is shown in figure 1. Patients with established CVD or conditions which markedly elevate their CVD risk do not need risk assessment. They should receive evidence based interventions, as outlined by specialist guidelines and JBS3. In the remainder, 10-year CVD risk should be estimated using the JBS3 calculator. If an individual's risk is above the threshold, CVD risk reduction should be prescribed by lifestyle and pharmacological therapy. The appropriate treatment threshold for 10-year risk is currently under review by NICE. In those whose 10-year CVD risk is below the threshold, the new metrics in the JBS3 calculator, such as heart age, should be used to communicate to the patient/individual the opportunities from lifestyle change and, in some cases, pharmacological therapy.
The JBS3 risk calculator complements the NHS Health Check programme in England. This offers CVD risk factor measurement from the age of 40 years. A 10-year risk estimate from this age is of limited value as the great majority of CVD events occur after 50 years of age. We anticipate that the NHS Health Check programme, together with the lifetime risk metrics in JBS3, will provide an exciting opportunity to communicate better the concepts of CVD risk and the benefits of interventions, including lifestyle and in some cases medications. This approach is novel and the impact on public understanding and behaviour as well as its acceptability will need formal testing. It is important to emphasise that, for the majority, the strong message will be the potential gains from an early and sustained change to a healthier lifestyle rather than prescription of drugs. Adoption of JBS3 recommendations will result in significant changes in the approach to CVD prevention. The cost effectiveness and implications for implementation in different age groups will require evaluation. Ensuring equitable access to effective and safe pharmacological agents for those who would benefit is important, but a greater focus on adoption of healthier lifestyles by the wider population for long term CVD risk reduction is a major challenge. Understanding of the lifetime ‘investment’ opportunities is a key step in encouraging individuals to ‘take control’ of their CVD health agenda and that of their families. Strategies will need to be developed not only by medical experts, but by policymakers, health economists, patients, and the public.
1.2.6 Summary
-
Patients with established CVD are at high risk of future events and should be treated with lifestyle interventions and drugs, according to current guidelines and JBS3 recommendations, without the need for CVD risk estimation.
-
Individuals with a 10-year absolute CVD risk, currently being reviewed by NICE, should be treated with lifestyle and drug therapy.
-
There is justification, from recent safety and efficacy evidence, to widen eligibility for preventative drugs such as statins.
-
Absolute risk estimation is heavily dependent on age and gender, so that young people and especially women may not be eligible for treatment, despite having high levels of modifiable CVD risk factors.
-
JBS3 has developed a new calculator which addresses this issue and estimates both 10-year CVD risk and CVD risk measures over lifetime.
-
New metrics, such as heart age and CVD event-free survival, are displayed to assist communication of CVD risk and motivation for lifestyle change.
-
The JBS3 risk calculator will complement the NHS Health Check programme in England. Formal testing of its impact on understanding, behaviour, and outcomes is needed.
1.3 Risk calculator
1.3.1 Background
A recent review identified at least 70 different CVD risk scoring systems.24 Each system requires a specification of three main components:
-
What events are being predicted, for example, CHD, CVD, death?
-
What factors are used to make predictions?
-
What measure of risk is used?
This section describes the various choices that have been made about the final component, the measures which have been incorporated in the JBS3 risk calculator, and the assumed effects of interventions (appendix 1 contains the technical details).
1.3.2 Approach
Relative and absolute risks
Additive scoring systems are constructed on the basis of standard regression models, for example, logistic models for fixed-time events or Cox regression models for survival analysis. These estimate the relative risks associated with factors: specifically, if a factor x1 multiplies a risk by r1, then a series of factors x1,…, xk will produce an overall relative risk r1r2…rk. Taking logarithms shows the effect on the log(relative risk) to be log r1+log rk, which can then be interpreted as an additive scoring system. The scores can therefore be interpreted as log (relative risks). Technically, for logistic regression models these relative risks are actually odds ratios (ORs), and hazard ratios (HRs) for Cox regression models.
Relative risks are not enough for decision-making. In order to decide whether interventions are worthwhile, absolute risks of events need to be determined, together with the impact of different interventions on these risks. Total scores are therefore transformed to absolute risks by assuming a level of baseline risk appropriate to the population of interest. In general, this has generated absolute risks of CVD events up to a fixed period of time into the future: for example, 5 or 10 years.
It is important to note that no allowance for ‘competing risks’ is made in these short term prediction models—that is, it is implicitly assumed that the individual will not die of non-CVD causes. As people get older, this becomes an increasingly inappropriate assumption.
5- and 10-year absolute risks
These have been the standard measures of CVD risk since the early development of the Framingham score based on a logistic regression. The latest revision—Framingham General Cardiovascular Risk Score—is based on a Cox survival analysis, but still only considers a 10-year horizon, with no allowance for competing risks.25
The Framingham score has been adapted by many other groups. For example, JBS2 used a modified 10-year risk model,26 and the New Zealand system uses 5-year risks based on Framingham.27 Other groups have used their own data to produce 10-year risk estimates, including QRISK2,28 ASSIGN,29 and HeartScore.30 However, for reasons outlined in the preceding sections, there has been increasing attention on other risk measures, including longer term outcomes.
Absolute risks for longer horizons, allowing for competing risks
The Framingham system has been adapted to provide 30-year risk estimates.31 A number of different techniques were investigated, including simply putting together three 10-year risk scores. Their recommended procedure was a full survival analysis that allowed for competing risks from other causes of deaths.
Without allowance for other causes of death, the apparent cumulative risk of CVD will increase to implausibly high values over a long period, due to the implicit assumption that the individual cannot die from anything else. By including competing risks, a more realistic assessment of the risks of CVD is obtained, even though some apparently paradoxical consequences can result. For example, someone who stops smoking may increase their risk of an eventual CVD event, since the chance of their dying of non-CVD causes is substantially reduced, thus giving them a greater opportunity of a CVD event. The mathematical details of the competing risk approach are outlined in appendix 1.
Heart age and vascular age
These terms have been introduced as a way of visualising an individual’s current risk profile as a characteristic of their current state, rather than relating it to something that may or may not happen in the future. In smoking cessation research, telling a patient their ‘lung age’ has been found to have a beneficial effect on the smoking quit rate.32
Heart age and vascular age are used interchangeably in the revised Framingham score,25 each meaning the age of someone who has the same risk as the individual in question, but in whom all other risk factors are set at ‘normal’ levels. This has been particularly emphasised in the New Zealand risk calculator ‘know your numbers’ (http://www.knowyournumbers.co.nz/heart-age-forecast.aspx), which shows an individual's 5-year risk, and how this is projected to increase during their lifetime. It compares this risk with an ‘ideal’ profile (non-smoker, TC to HDL-c ratio of 4, BP of 120/80 mm Hg), and therefore obtains a heart age—the age of an ‘ideal’ person with the same current risks as the patient.
1.3.3 Lifetime risk profile
A lifetime risk perspective looks at the development of CVD risk throughout an individual's life, using a variety of summary measures. These include:
-
Cumulative risk of CVD: the accumulating risk of a CVD event occurring before each age, retaining in the denominator those individuals who die from other causes and hence who are not available to suffer an event. Risk of a CVD event up to any specified age can be read off from this.
-
Survival without CVD: this is a survival curve in which people are withdrawn as ‘failures’ if they suffer either a CVD event or death from another cause. It therefore displays the chance of being alive and without having suffered a CVD event.
-
Mean (median) age at first CVD event: the median is simply read off from the preceding survival curve—the mean is the area under the survival curve, added to the current age.
Ulrich et al33 carried out a discrete-time competing risks analysis in 5-year bands, using Framingham for the 5-year CVD risks and Office of National Statistics mortality data for non-CVD risks. This explored a range of measures for communicating the impact of interventions on the long term cause of CVD risk. These have been adapted for use in the JBS3 risk calculator. The Framingham data have been used to create lifetime risk assessments, with allowance for competing risks, for an age range between 50 and 95 years.17 However, these models do not appear to be available for general use. The QRISK Lifetime risks model uses a competing risks analysis, producing both summary CVD risk up to age 95 years, and a curve showing the cumulative risk of a CVD event.34
Which summary risk measure is it best to use?
The academic literature is clear that there is no ‘correct’ way to communicate risks, both for estimation of CVD risk level and for use of preventative interventions—preferences and understanding can depend on an individual's educational level and in particular their numeracy, but also their personality, particularly their optimism.35 Selecting among the range of potential measures, therefore, presents a problem: while some individuals may be motivated by short term absolute risk, others may have a stronger attachment to longer term outcomes such as maximising their chance to reach an age—for example, 70 years—at which they might expect to know their grandchildren. In JBS3, the use of multiple forms of presentation therefore reflects the fact that there is no ‘best’ way of communicating to people their future risks—different summaries may have different salience for different individuals. Certain measures may also be more appropriate for guiding decisions about therapeutic intervention.
Methods used in JBS3 risk calculator
Use of QRISK
As noted previously, many different CVD risk scoring systems have been developed. QRISK Lifetime has been chosen as the basis for the JBS3 risk calculator as it provides the option of a calculation of lifetime risk and is based on a UK population. However, all risk assessment systems have limitations in the factors that can be included and the broad assumptions that are made, and so any numerical risk calculation must necessarily be interpreted in the light of the specific circumstances.
The data collected are based on the requirements of QRISK Lifetime http://www.qrisk.org/lifetime/ (table 1).
The requirements of QRISK Lifetime
Applying transformations and the HRs shown in the table, HRs for CVD events and non-CVD deaths are obtained.34 Applying these to a baseline age-specific risk of death (see appendix 1) provides the probability of being alive and CVD-free at each age, and the cumulative risk of CVD.
In the Heart Age and Compare screens, the baseline (‘optimal’) individuals are assumed to have the following characteristics:
-
Baseline female: Non-smoker, same ethnicity, no clinical conditions, and with √(BMI/10)=1.605 (BMI=25.8), systolic BP=120.0, cholesterol ratio=3.5, and Townsend score=−0.30 (where the covariate is in terms of five units, and so corresponds to an original Townsend score of −1.51).
-
Baseline male: Non-smoker, same ethnicity, no clinical conditions, and with log(BMI/10)=0.968 (BMI=26.3), systolic BP=120.0, cholesterol ratio=3.5, and Townsend score=−0.165 (where the covariate is in terms of five units, and so corresponds to an original Townsend score of −0.83).
1.3.4 Intervention assumptions
The table provides an ‘epidemiological’ HR for CVD events, which is the ratio of the daily risks of two different people who differ in this risk factor. However, when assessing the effect of intervening on an individual, it is necessary to decide the HR when an intervention changes the risk factor —that is, the ratio of the daily risks before and after the intervention in the same person. This may be less than the epidemiological HR, but also could be greater.
Direct evidence of the effect of changing behaviour or intervening to change physiological measures comes from clinical trials; it is also possible to make indirect inferences from observing cohort studies. However, evidence is limited and some assumptions are inevitable.
Blood pressure
In a recent review of trial data,36 Law et al estimated an approximate 50% reduction in CVD events per 20 mm Hg reduction in systolic BP, which is similar to that expected from the epidemiological evidence for CVD mortality from the Prospective Studies Collaboration.37 This is substantially larger than the association found in the QRISK Lifetime risk formula, which uses an HR of 1.13 (female) and 1.11 (male) per 20 mm Hg increase in systolic BP—that is, around 11% reduction in event rate per 20 mm Hg reduction in systolic BP. This difference likely to be due to the many other correlated factors included in the risk formula. In JBS3, the Law et al estimate has been adopted, which corresponds to a HR of 0.966/mm Hg reduction in systolic BP. Law et al reported no impact of blood pressure intervention on non-CVD causes of death.
Cholesterol
A recent meta-analysis estimated a 22% reduction in CVD event rate per 1 mmol/L reduction in LDL-c over a wide range of baseline conditions.11 Since TC and HDL-c are readily measured in general practice, JBS3 has adopted non-HDL=TC-HDL-c as the measure of intervention: assuming that non-HDL-c is approximately 1.24×LDL38 this leads to an HR of (0.78)1/1.24=0.82 per 1 mmol/L reduction in non-HDL-c. No impact of cholesterol interventions on non-CVD causes of death has been assumed.
Smoking
Since ‘former smoker’ is a category in the QRISK lifetime score, it has been assumed that an intervention to stop smoking leads to the epidemiological risk associated with ‘former smoker’. There is also a clear impact on non-CVD causes of death, and again the ‘former smoker’ risk is assumed.
Weight
No reliable data on the effect of weight reduction in its own right are available, rather than through its effect on BP and cholesterol, thus currently weight has not been included as an intervention.
While weight and height are included in the risk calculator, a weight reduction entered into the risk calculator will not in itself lead to any change in CVD risk score, as associated risk factor changes in BP and lipids are not automatically modelled. However, it is known that a 10% weight loss will typically lead to a 10 mm Hg reduction in systolic BP, a 10% reduction in TC, and an 8% rise in HDL-c. Such changes, or those expected for a given weight reduction, should be entered directly to help determine expected risk changes with weight loss.
1.3.5 Ongoing and unresolved issues
It is crucial to acknowledge that any numerical summary that is derived from a risk calculator is not the risk of an individual. Many assumptions are used in the calculation, and limited information on each individual is included so that further evidence, such as genetic information, would almost certainly change the assessed risk. It is perhaps best to think of the quoted risk as being constructed on the basis of available evidence from populations and limited information on the individual: it does not exist as an objective state of the world, and hence, it is unreasonable to seek great precision.
Nevertheless, it is reasonable to seek some discrimination, in that different people do get assigned a range of risks, and calibration, so that, for example, when a risk of 70% is quoted for an event, then it will happen in around 70% of cases. Validation details for QRISK Lifetime have been published.34
There are inherent assumptions when population based estimates for risk factor modification effects on CVD outcomes are extrapolated for use in an individual. Nevertheless, these estimates provide the individual with a reasonable guide to the potential benefits of risk modification and emphasise the importance of early intervention of multiple risk factors.
1.3.6 Using the JBS3 risk calculator
The online risk calculator can be accessed at http://www.jbs3risk.com. The profile page highlights that the calculator should not be used for patients with known CVD, where treatment and healthcare professional advice should be followed according to established recommendations. In patients with certain high risk condition such as high BP, diabetes, and CKD, the risk calculator must be used with caution as specific drug treatment and other recommendations may already be indicated in these conditions, as indicated in the relevant JBS3 sections. However, the risk calculator may be of additional help in highlighting the high risk and the benefits of intervention. Note also, that when TC exceeds 7.5 mmol/L the calculator will highlight the possibility of FH, where further assessment is indicated.
The Townsend Quintile score allows the user to input information on social deprivation, where this is available, and can be guided by the visual display. This has some small influence on the risk calculation, but defaults to an average score which should be used when social status is unknown or unclear.
Once the profile page is completed, it is then possible to advance to display estimated CVD risk in various formats, as detailed below. Display of these various formats can be changed from the top menu display. The ‘intervention’ section on the right hand side of all screens (other than the profile page) allows the user to input various interventions to see the effect on CVD risk estimates. More displays are available, revealed using the ‘more’ button on the menu bar.
The following examples demonstrate these various displays and show a number of clinical scenarios to highlight the potential value of the JBS3 risk calculator.
Example 1: young female with adverse risk factors
This example demonstrates the potential effect of early risk factor modification on CVD risk, and the clinical benefits of early versus delayed/no intervention. It also demonstrates the variety of visual displays designed to assist clinical discussion and to facilitate a person's understanding of the importance for them, as an individual, of early lifestyle modification and risk factor reduction.
In addition, it demonstrates some of the disadvantages of using current 10-year absolute risk in young females. Finally, this example demonstrates how the risk calculator can predict optimal time for intervention to achieve the greatest clinical gain and how it might be used to inform the balance of clinical gains versus economic consequences when pharmacological therapy is required in addition to other lifestyle interventions.
Profile of subject 1 (figure 2)
-
A 35-year-old female smoker
-
Systolic BP of 160 mm Hg
-
TC of 7.0 mmol/L, HDL-c of 1.4 mmol/L (non-HDL-c 5.6 mmol/L)
-
Family history of premature CVD
The risk calculator estimates this person's heart age to be 47 years (figure 3)—predicting an average survival to the age of 71 years without a CVD event, but a 10-year CVD event risk of 1.9% (figure 4).
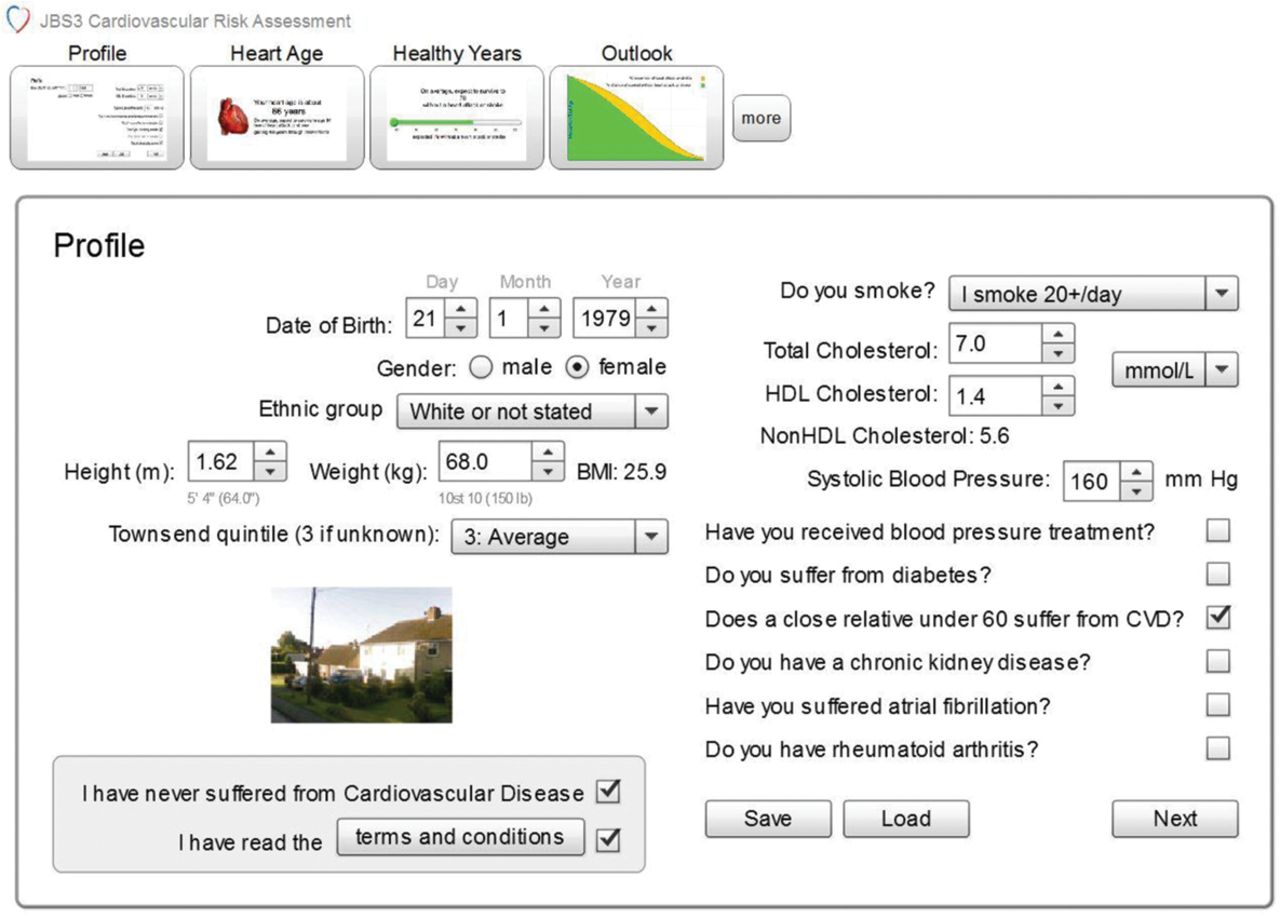
Profile of subject 1.

Heart age of subject 1 is 47 years.

Subject 1 has an average survival to the age of 71 years.
The percentage chance of having had a CVD event increases with age as shown in figure 5.

The percentage chance of having had a cardiovascular disease event by age for subject 1.
Effect of risk factor modification
Intervention in this individual at her current age of 35 years, including stopping smoking and introducing other lifestyle changes and, if necessary, drug therapy to reduce systolic BP to 130 mm Hg and TC to 4.0 mmol/L (non-HDL-c 2.6 mmol/L), has the following effect on her risk profile (figures 6 and 7).

Effect of risk factor modification on heart age for subject 1.

Effect of risk factor modification on survival for subject 1.
Heart age is reduced from 47 years to 30 years and the average age to first CVD event is increased from age 71 to age 85, gaining 14 years of expected life without a CVD event through risk factor modification.
These benefits can also be demonstrated graphically comparing the temporal effects of early sustained intervention versus no intervention (figures 8 and 9). Note that as the lines diverge, this indicates the optimal time for risk factor modification to obtain maximum clinical benefit.

Chance of survival free of heart attack or stroke for subject 1.

Percentage chance of having had a heart attack or stroke for subject 1.
The clinical benefits of early intervention to modify risk factors are shown in figure 10, demonstrating that, although risk factor modification at any age has some clinical benefit, the number of potential years gained begins to fall off sharply if intervention is delayed beyond the age of 40 years.

Event-free years gained or lost for the age that intervention starts for subject 1.
The following additional visual displays can also be used to highlight further the value gained for an individual by early intervention, the various displays enhancing the potential impact on different individuals who often resonate more with one particular display. This first display (figure 11) demonstrates outcome with and without intervention as compared to the general population, and shows the substantial impact of intervention at an early age.

Outcome with and without intervention as compared to the general population for subject 1.
The next display (figure 12) demonstrates the effect of intervention in 100 identical individuals who undertake this level of risk factor modification from age 35–80, with 46 of the 100 individuals being prevented from having a CVD event.

The effect of intervention in 100 individuals identical to subject 1 who undertake the same level of risk factor modification from age 35–80 years.
This can also be displayed in an alternative format that shows what would happen to 100 people who carry on as usual compared to 100 people who undertake the intervention (figure 13).

The situation that is expected to occur if 100 people identical to subject 1 carry on as usual.
Or, simply displayed as the difference between the two groups (figure 14).

The difference between individuals identical to subject 1 who either carry on as usual or receive intervention.
Using the visual displays as above, the risk calculator can demonstrate the difference between early intervention compared to the effect of waiting for the 20% absolute risk threshold to be crossed, which in this individual would occur at age 64 years. Although there are still significant benefits from risk factor modification at age 64 years, these are predicted to be considerably less than those obtained by early intervention at age 35 years under the assumptions stated (figure 15).

Risk factor modification at age 35 years compared with that at age 64 years for subject 1.
Optimal clinical and economic benefits
As demonstrated, the JBS3 risk calculator is able to display the optimal time for risk factor modification which will provide the maximum clinical benefit over time (figure 10). As the event-free years gained starts to fall off with increasing age, the compound interest in ultimate gain will be reduced.
Where lifestyle modification alone is insufficient to provide the optimal clinical gains in future risk reduction, it is often necessary to introduce pharmacological interventions to optimise risk reduction. Here there is a potential economic consequence which needs to be balanced against clinical gain. The JBS3 risk calculator provides a tool to facilitate this by providing an estimate of event-free years gained per year of intervention (figure 16). Not only does this provide an absolute estimate of the number years gained per year of intervention, which may inform an arbitrary threshold for commencing drug therapy, but it also provides an estimate, within an individual, of the point at which starting therapy provides the maximum benefit per year of intervention.
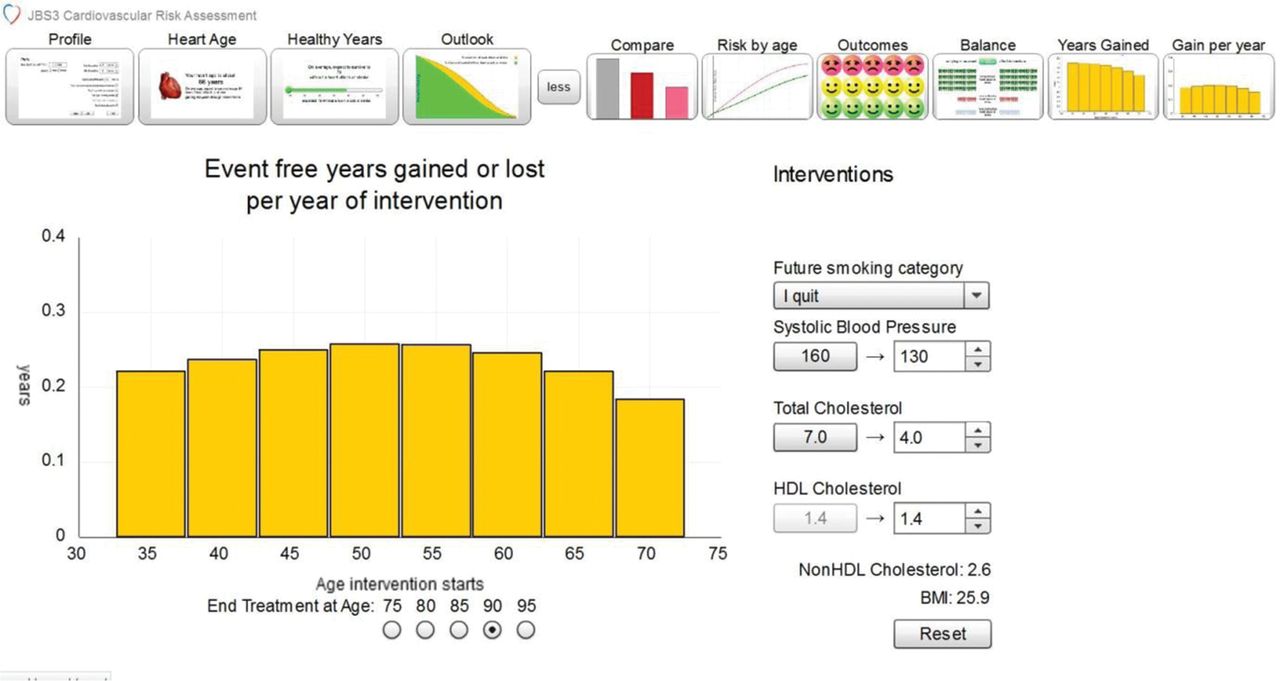
Event-free years gained or lost per year of intervention for subject 1.
Note that, for this particular risk profile, the optimal age to start treatment to achieve the maximum gain per year of intervention would be age 50 years. However, it is important to note that commencing treatment at the earlier optimal age for maximum clinical benefit still provides an additional gain for each year of intervention, which will be considerably greater for this individual rather than in others who have a much lower baseline risk profile.
It is not the role of JBS3 and the risk calculator to determine a threshold for intervention with drug therapy, but it does provide a tool which may help inform the selection of the appropriate metric threshold, based on both clinical and economic benefit. Whether this would be based on an absolute value of event-free years gained per year of intervention across a population, the maximum gain per year of intervention within an individual, or a combination of the two, would be a public health policy decision, in conjunction with an informed choice of the individual and their responsible clinician.
Example 2: 35-year-old male with significant risk factors
The JBS3 risk calculator emphasises the potential advantages of early intervention to modify CVD risk factors. Although in many cases this may require the additional introduction of pharmacological therapy, it also highlights the potential benefits of early lifestyle modification. For example, for a 35-year-old male, smoking 20 cigarettes per day, with a TC of 6.8 mmol/L, HDL-c of 1.2 mmol/L (non-HDL-c of 5.6 mmol/L), a systolic BP of 158 mm Hg, and a family history of premature CVD, the risk calculator would predict a heart age of 44 years (figure 17) and an expected age of survival without a CVD event of 66 years, but a 10-year risk of only 3.2% (figure 18).

Heart age of subject 2.

Expected age of survival without a cardiovascular disease event for subject 2.
By instituting lifestyle changes alone, stopping smoking, weight reduction, exercise and dietary advice, it would be reasonable to expect a modest reduction in TC to 5.9 mmol/L (non-HDL-c 4.7 mmol/L) and systolic BP to 145 mm Hg, without drug therapy. Heart age would then be reduced to 38 years (figure 19) with an average expected gain of 10 years before a CVD event (figures 20 and 21).

Effect on heart age of instituting lifestyle changes alone for subject 2.

Effect of lifestyle changes on age of subject 2 at which a heart or stroke occurs.
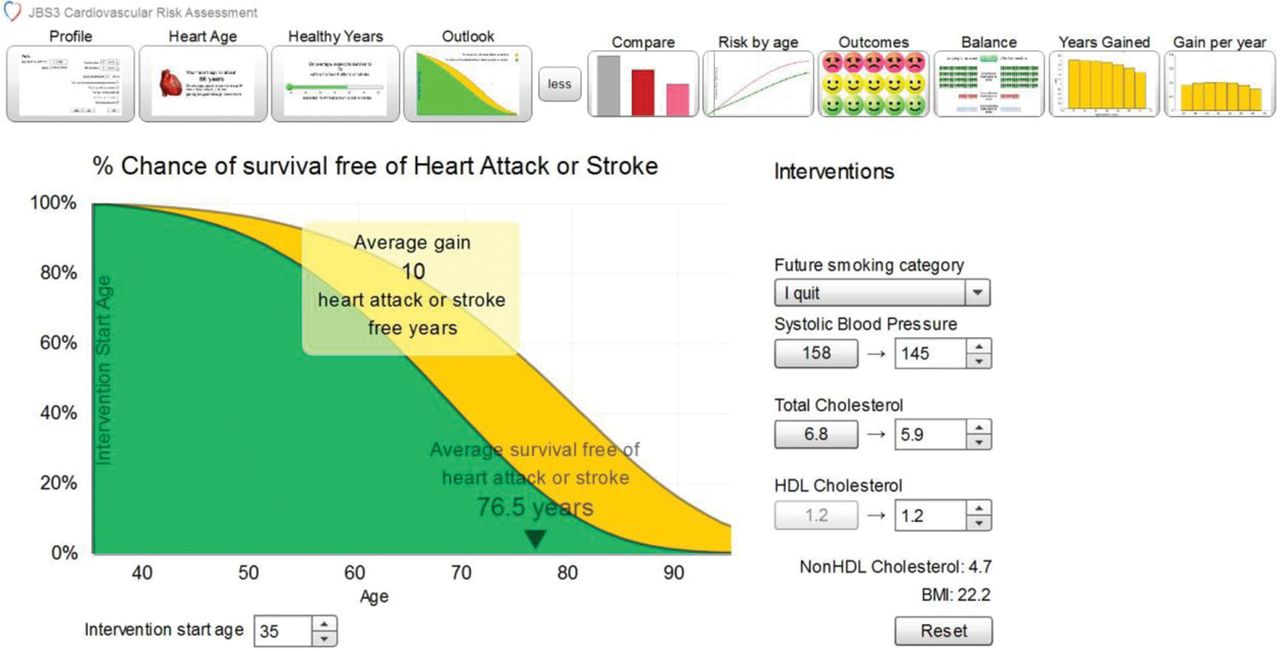
Percentage chance of survival free of heart attack or stroke for subject 2.
However, if intervention was delayed until the age of 60 years, the potential gain, although substantial, would be considerably reduced, even if intensive risk factor reduction with additional drug therapy was instituted at this stage, to achieve more optimal risk factor reduction (BP 130 mm Hg, TC 4.0 mmol/L, non-HDL-c 2.8 mmol/L) (figures 22 and 23). The ‘compound interest’ gained from early lifestyle changes outweighs the benefits from late intervention, even with additional drug therapy.

Effect of delaying intervention until the age of 60 years for subject 2 on survival without a heart attack or stroke.

Effect of delaying intervention until the age of 60 years for subject 2 on percentage chance of survival free of heart attack or stroke.
Of course, there are still additional advantages to be gained from this intensive, more optimal risk factor modification at the younger age (figures 24 and 25), where additional drug therapy is likely to be required to achieve this level of risk factor modification. Here, the balance of lifestyle modification alone versus additional drug therapy might merit further discussion with the individual and appropriate advice from their healthcare professional.

Effect of more intensive risk factor modification at a younger age for subject 2.

Effect of more intensive risk factor modification at a younger age for subject 2 on percentage chance of survival free of heart attack or stroke.
Example 3: 58-year-old male with multiple risk factors
The JBS3 risk calculator also emphasises the importance of intensive risk factor modification in those with substantial 10-year absolute risk. For a 58-year-old male, who smokes between 10 and 20 cigarettes per day, has a systolic BP of 155 mm Hg and a TC of 6.8 mmol/L (non-HDL-c 5.6 mmol/L), from the least affluent social background Townsend quintile, but with no significant pre-existing family history of CVD, the risk calculator would predict a heart age of 73 years and an average expected age of survival without a CVD event to age 72 years, with a 10-year risk of a CVD event of 17% (figure 26).
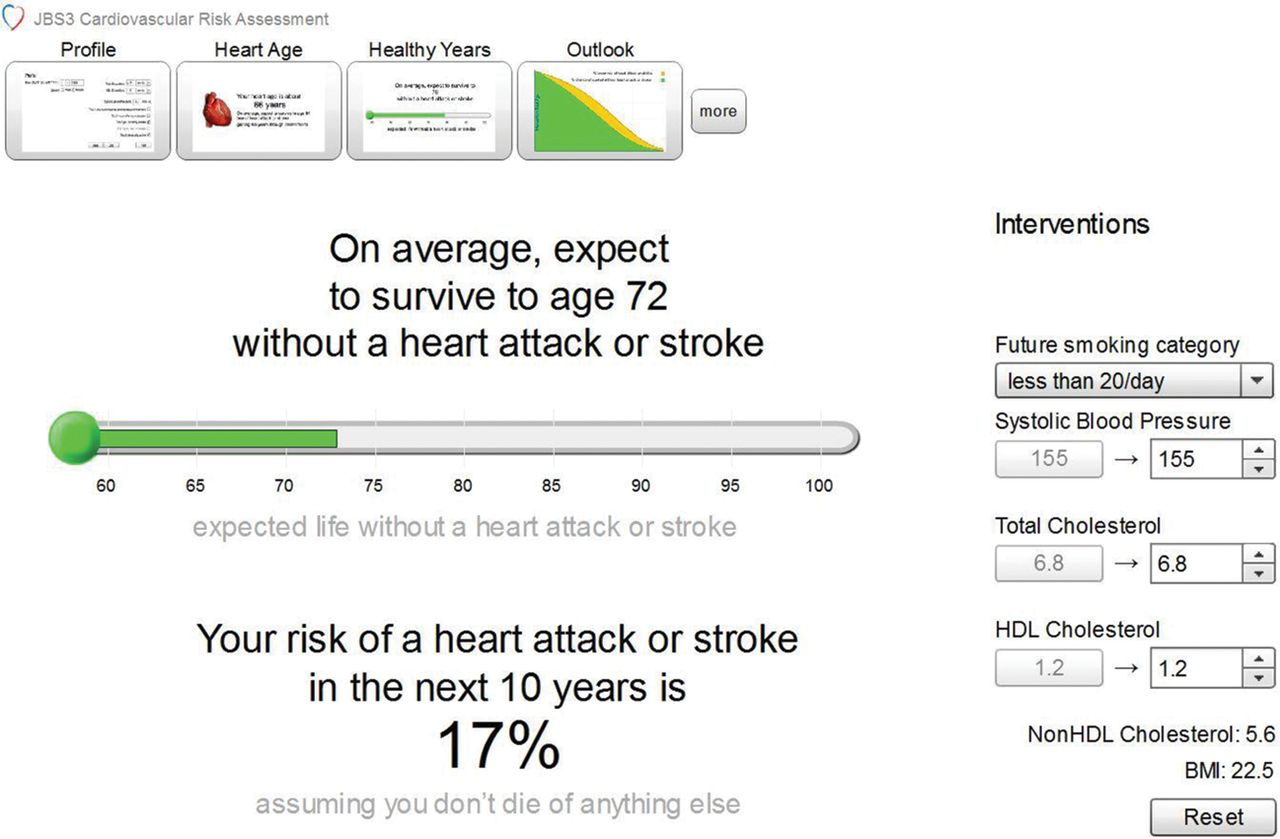
Average expected age of survival without a heart attack or stroke for subject 3.
Intensive risk factor modification including stopping smoking, reducing TC to 3.7 mmol/L (non-HDL-c 2.5 mmol/L), and reducing systolic BP to 125 mm Hg has the effect of gaining an average of a further 7 years without CVD event, as shown in figure 27.
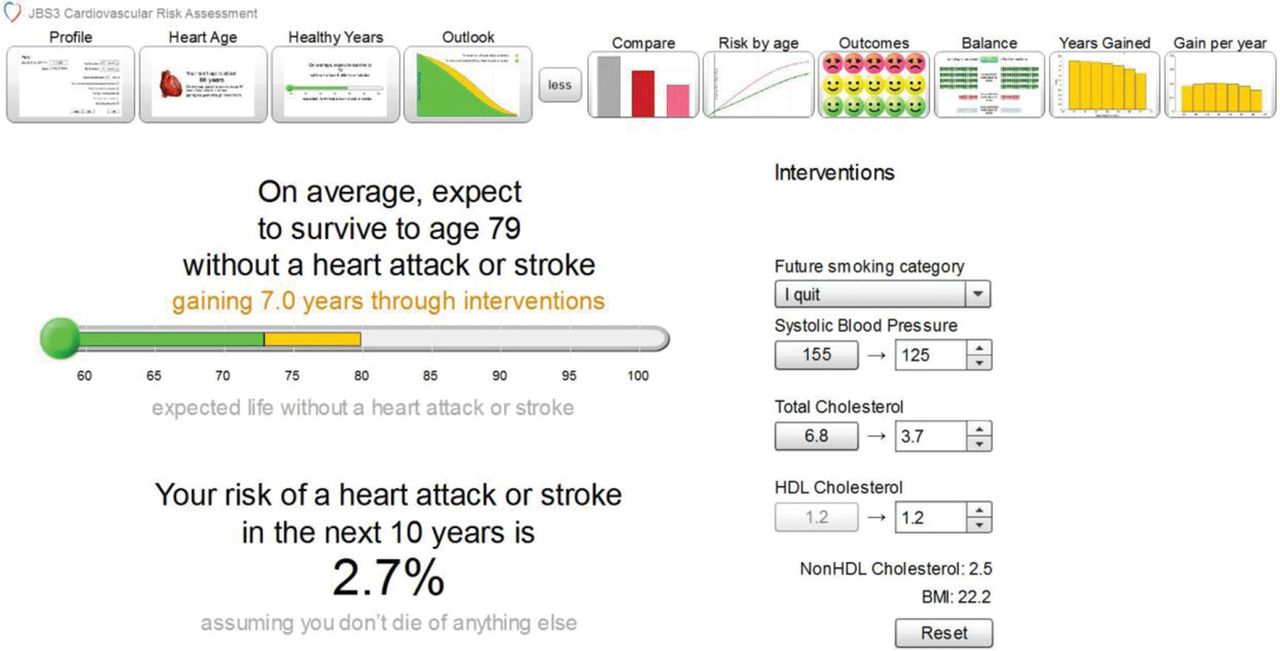
Effect of intensive risk factor modification on average expected survival without a heart attack or stroke for subject 3.
There are both short and longer term gains, as shown by the reduction in percentage risk of a future CVD event over time (figure 28).

Percentage chance of having had a heart attack or stroke for subject 3.
1.3.7 Conclusion
The JBS3 risk calculator provides an estimate of short term, 10-year CVD risk as well as longer term ‘lifetime’ risk with the potential benefits of risk factor modification. These are designed to facilitate an informed discussion between an individual and their healthcare professional regarding decisions about lifestyle changes and, where indicated, pharmacological therapy. Different visual displays are likely to resonate more with certain individuals so the spectrum of displays provided within the JBS3 risk calculator allows flexibility healthcare professionals on how to give individuals an understanding of CVD risk and the benefits of intervention. As new evidence evolves, the JBS3 risk calculator can be updated to allow a contemporary understanding of CVD risk and its modification.
1.4 Refinement of risk models
Recommendations
-
Use of non-invasive imaging tools to detect subclinical atherosclerosis is not recommended for CVD risk assessment in the primary prevention setting. Utility for selected groups of individuals requires further study.
-
Currently available novel biomarkers do not replace or enhance established methods for CVD risk assessment in the primary prevention setting, but studies are ongoing.
-
Common genetic variants associated with blood lipids and CVD events currently perform less well than phenotype based methods for risk assessment and, except for screening for FH, are not recommended for CVD risk assessment in the primary prevention setting.
1.4.1 Refining CVD risk assessment using new technologies
Risk equations, using traditional CVD risk factors, can accurately assign group risk (ie, observed group event rates are close to event rates predicted by the group model), but perform less well in distinguishing which individual will or will not experience a CVD event in the future. This is largely explained by the fact that the majority of the CVD events occur among those at ‘intermediate risk’. Since the publication of the Framingham risk score in 1976, there have been extensive efforts to identify additional factors which might refine risk prediction over and above the traditional risk factors contained in the score. An important aim has been to identify individuals within the intermediate risk category who are destined to suffer a CVD event in the future (and who therefore might merit pharmacological treatment) as well as those likely to have a good outcome without intervention. This approach is consistent with widespread interest in more personalised healthcare and new technologies.
It should be emphasised that an aetiological role is not a prerequisite for a novel predictive biomarker. The efficacy of a more tailored approach to CVD prevention based on genes, biomarkers, or imaging, is crucially dependant on how well these technologies predict CVD events and how much they add to existing risk equations.
New tools for CVD risk assessment fall into three broad categories: those developed to detect the presence of subclinical atherosclerosis, blood based biochemical markers of CVD risk, and genotype. Their value in clinical practice and implementation will depend not only on predictive accuracy but on their cost, safety, and convenience.
1.4.2 Tools to detect subclinical atherosclerosis
Atherosclerotic lesions develop as early as the first decade of life, advancing with time in many different vascular territories before clinical manifestations occur. These are usually consequent on atherosclerotic plaque rupture, and typically occur beyond the age of 50 years. Several non-invasive imaging methods are now available for detecting subclinical atherosclerosis during this preclinical window.
Ultrasound imaging of the carotid artery
Atherosclerotic plaques can be detected in the carotid artery using ultrasound imaging, and cIMT can also be quantified by the same technique. Carotid plaque detected by ultrasonography correlates well with atheroma detected histologically in the same vessel.39 However, there is debate as to what extent cIMT represents early atheroma or other age related alteration in vascular structure. Nevertheless, both measures are associated, in prospective studies, with a higher risk of both cerebrovascular and coronary events.40 cIMT has been included in the recent European Society of Hypertension (ESH) and ESC guidelines for management of arterial hypertension.41
However, consistent, statistically significant associations do not necessarily translate into clinically useful improvements in risk prediction. This depends not only on the strength and shape of the association but also on the distribution of the new measure in the population under consideration. Like many other new measures aimed at improving the prediction of CVD events, the distribution of cIMT values in populations describes a normal distribution, while the association with CVD risk is linear and without a threshold. As a consequence, many CVD events occur among those with intermediate values of cIMT, and the distribution of cIMT values in those who eventually suffer an event and those remaining healthy overlap considerably. A meta-analysis of 18 studies that incorporated information of 2920 individuals with CHD (mean age range 46–73 years) and 41 941 without (aged 44–73 years) reported that the presence of carotid plaque had a detection rate (DR or sensitivity) of 62% for a false positive rate of 30% (likelihood ratio 2.1, 95% CI 1.6 to 2.4). For a false positive rate of 30% (equating to an cut-off ≥0.82 mm), the detection rate for cIMT was 65% (likelihood ratio 2.2, 95% CI 1.9–2.5).42 Combining assessment of plaque with assessment of cIMT yielded some gains, but the authors concluded that while “combining cIMT measurement with plaque assessment was better than using either measurement alone the ‘improvement’ was insufficient to make carotid ultrasound screening for CHD worthwhile”.
Aortic stiffness can be assessed clinically by measurement of carotid–femoral (aortic) pulse wave velocity (PWV). Data from prospective observational cohort studies show that PWV is linked to future CVD events, even after adjustment for other CVD risk factors. In a recent systematic review of 17 685 subjects in 16 studies, the addition of PWV to Framingham risk score resulted in a 13% overall 10-year risk reclassification.43 PWV can be measured relatively easily and reproducibly in clinical practice, but randomised clinical trials are required to assess its value for risk stratification and/or treatment decisions.
Ankle-brachial pressure index
The ankle-brachial pressure index—the ratio of the systolic BP in the ankle (measured using a Doppler probe) to that in the brachial artery (using sphygmomanometry)—is an index of atherosclerosis in arteries of the leg. Lower values are associated with atherosclerosis in other vascular territories, with established risk factors for CVD and with higher risk of CVD events and total mortality.44 In a participant level meta-analysis of prospective studies, low ankle brachial pressure index (ABPI) (≤0.9) versus normal ABPI (1.11–1.4) was associated with an approximately threefold higher total mortality in both men and women, and a nearly three- to fourfold higher CVD mortality and rates of major coronary events, across all categories of Framingham risk. Despite this, when information on ABPI was added to the Framingham risk score, there were only marginal improvements in the area under the receiver operating characteristic curve. This may be because ABPI is associated with many of the variables already included in the Framingham risk score.
CT for detecting coronary artery calcification
Calcification can be observed in atherosclerotic plaques even from the early stages of their evolution, although calcium deposits become an increasingly common feature in older and more complex lesions. Calcium deposits can be detected non-invasively by ‘fast’ CT methods, such as electron beam or multidetector CT (EBCT and MDCT, respectively). Although the relationship of coronary calcium detected by these methods with the degree of coronary occlusion or the risk of plaque rupture is uncertain, the extent of CT detected calcium, quantified by established methods, is associated with an increased risk of CVD events.44 ,45 In several studies, measurement of coronary artery calcification has consistently proven to be the best surrogate measure for CVD prediction, discrimination, and risk reclassification. However, because this method of screening is expensive and requires a radiation exposure, there are obstacles to its widespread use for CVD risk assessment except in narrowly defined groups that might benefit the most from more refined risk assessment. There is currently insufficient evidence on the trade-off between the benefits and harms, or the cost effectiveness of this approach for CVD risk assessment, or the subset of the population that might benefit. The broad category of intermediate risk individuals constitute the majority of the population, so it seems unlikely that coronary calcium screening could be applied to this large group as a whole.
In individuals, the relationship between coronary artery calcification and outcome is even more difficult. Studies have shown that high calcium density in plaques is associated with lower CVD event rates, suggesting that it may be a ‘protective’ signal. Furthermore, LDL-c lowering with statins has been correlated with a significant increase in coronary artery calcification progression in some studies, so that changes in calcium scores with time or after interventions in individuals are difficult to interpret in clinical practice.
1.4.3 Blood markers
Atherosclerotic lesions are exposed to the circulating blood, which can be readily sampled by venepuncture. As a consequence a large body of research has documented alterations in lipid subfractions, apolipoproteins, coagulation, and inflammation markers, and other blood constituents in those with or at higher risk of cardiovascular events. The interest in these ‘emerging risk factors’ is twofold: first, in the possibility that one or more might be aetiologically involved in CVD (like LDL-c), and so amenable to therapeutic targeting; and second that information on emerging risk factors might assist CVD risk assessment, which does not necessarily require that the measure is causally involved in the disease.
Of the many hundreds of markers in this category, the most widely studied have been fibrinogen,46 C reactive protein (CRP),47 interleukin 6,48 B-type natriuretic peptide or NT-B-type natriuretic peptide,49 apolipoproteins A1 and B,50 lipoprotein (a),51 and lipoprotein associated PLA2.52
Biological function
Each of the biomarkers has a plausible biological function in the development or read-out of CVD; however, it remains uncertain whether—with the possible exception of apolipoprotein B, which is resident on the LDL-c particle—any of these biomarkers are actually causally involved in atherogenesis. Indeed, in the case of CRP, sufficient evidence has accumulated as to make this very unlikely.53 ,54 However, if the aim of measuring a biomarker is risk prediction, it need not play an aetiological role in atherosclerosis to have value.
Method of assay and variability
For a biomarker to be useful clinically it should be stable in routinely collected blood samples, there should be reliable assays that can operate at scale, and the marker itself should exhibit minimal biological variability. Several of the markers (eg, apolipoproteins A1 and B, and CRP) have these attributes, although, in this context, it is important that CRP is measured in the absence of overt infection or inflammation. However, there are complicating factors for others, such as Lp(a) (for which some assays fail to distinguish fully differences in isoforms from differences in concentration), lipoprotein associated PLA2 (where different assays exist for activity and concentration), and fibrinogen (where assays utilise different methods for measuring fibrinogen concentration).
Cross-sectional correlates
Biomarkers that exhibit multiple strong correlations with variables already included in existing risk models are less likely to yield incremental information for prediction. For example, CRP exhibits an extremely wide range of modest correlations with age, smoking, BMI, LDL-c, HDL-c, and triglycerides, all of which contribute to the Framingham score.47 Apolipoproteins B and A1 are very tightly correlated with LDL-c and HDL-c concentrations, to the extent that the argument on their utility has rested not on whether they might supplement information based on established risk factors, but rather on whether their measurement might take the place of LDL-c and HDL-c, largely for analytical reasons.50 Lp(a) concentration is largely genetically determined and exhibits fewer correlations with other CVD risk factors than most other biomarkers.51 However, there remain associations with the major blood lipid fractions and apolipoproteins A1 and B in subjects of European descent, particularly at very high Lp(a) values.
Shape and strength of the epidemiological associations with CVD outcomes
With the exception of Lp(a), where the relationship to CVD events appears confined to individuals with the very highest values,51 most other markers exhibit a log-linear relationship with no evidence of a threshold effect. Because most markers have a normal or log-normal distribution, the expectation would be that more events would occur among the larger proportion of individuals with intermediate biomarker values than among the smaller proportion with very high values.55 ,56 A corollary is that the distribution of marker values among those who later develop events and those remaining event-free should exhibit substantial overlap and that their ability to discriminate (distinguish) later cases would be limited. This has been borne out empirically. For example, despite exhibiting consistent association with CVD events, the ability of CRP to discriminate individuals who will suffer events is extremely modest and similar to BP or cholesterol values on their own.57 ,58
Combining risk factors, in the form of a multi-marker risk score, provides only small gains in discrimination.59 ,60 The reasons are twofold. First, the standard deviation of any multi-marker score is greater than that of its components, increasing the overlap of the score distribution among affected and unaffected individuals, and thereby reducing discrimination. Secondly, most risk factors tend to be correlated with one another.
1.4.4 Genotype
Genome-wide association studies (GWAS), which compare the frequencies of many hundreds of thousands of single nucleotide polymorphisms (SNPs) in patients and healthy controls, have identified several susceptibility genes or genetic regions for CHD.61–63 More are likely to be identified in the future as collaborative efforts to pool genetic data from independent studies progress. As with other common diseases, the effect at each locus is weak (typically a 5–10% increase in risk), the loci are dispersed across multiple chromosomes, each inherited independently, and the effect of each appears to be additive and independent. Few genetic loci for the common forms of stroke have been identified to date, but GWAS are ongoing.
Although these findings are beginning to provide new insights into disease aetiology, the potential for common SNPs of modest effect to improve prediction of CVD is limited.64 The reasons for this are:
-
The risk conferred by any one SNP is small
-
Few in a population carry the very small or very large number of risk alleles sufficient to cause substantial differences in risk; although those who carry a heavy burden of alleles will be at high risk, the number needed to screen to identify such individuals would be very large
-
The frequency distribution of common independently inherited risk alleles for CVD approximates a normal distribution, with most individuals carrying an intermediate number of risk alleles. Because the association with risk is additive, more cases of disease would be expected in the many people with an intermediate number of risk alleles than in the minority with a large number of alleles.
Although the common risk alleles, identified from GWAS, are constrained in their ability to help predict CVD risk, there may be scope for improvements. Genetic tests that capture a wider range of variability in a given gene or region, rather than simply a few SNPs, may help improve genotype based risk prediction in the future.
1.5 Lifestyle interventions
Recommendations
Smoking
-
Professional support on how to stop smoking should be given, at every available opportunity, with provision of self-help material and referral to more intensive support —for example, stop smoking services.
-
The JBS3 risk calculator emphasises the benefits for early smoking cessation and the diminishing, but still substantial, returns from quitting at an older age.
-
Patients should be offered behavioural counselling, group therapy, pharmacotherapy or a combination of treatments that have been proven to be effective.
-
NRT, varenicline or bupropion should be offered to people who are planning to stop smoking, as part of an abstinent-contingent treatment in which the smoker makes a commitment to stop smoking on or before a particular date (target stop date).
-
People who have heart or respiratory diseases, and those who live with them, should be made aware of the risks to them of both active and passive smoking (SHS).
-
For specific recommendations on quitting smoking in pregnancy and following childbirth, see NICE public health guidance 26.
Diet
Professional support to consume a diet associated with the lowest risk of CVD should be provided based on the following principles:
-
Intake of saturated fat to <10% of total fat intake (preferably in lean meat and low fat dairy products)
-
Replace saturated fat with polyunsaturated fat where possible
-
Consume five portions per day of fruit and vegetables
-
Consume at least two servings of fish (preferably oily) per week
-
Consider regular consumption of whole grains and nuts
-
Keep salt consumption <6 g/day
-
Limit alcohol intake to <21 units per week for men and <14 units per week for women
-
Avoid/reduce consumption of:
-
Processed meats or commercially produced foods which tend to be high in salt and TFA
-
Refined carbohydrates, such as white bread, processed cereals
-
Sugar sweetened beverages
-
Calorie rich, but nutritionally poor, snacks such as sweets, cakes, and crisps
-
Children and young people should be supported to consume a diet based on the same principles.
-
Physical activity and exercise
-
An increase in overall levels of sustained physical activity and avoidance of prolonged sedentary behaviour are important for reduction of CVD risk.
-
Emphasise walking, cycling, and other aerobic physical daily activities, at moderate intensity, as part of an active lifestyle, for at least 150 min per week in bouts of ≥10 min, or 75 min per week of vigorous physical activity, or a combination of the two.
-
Muscle strengthening activities performed on at least two occasions per week.
Exercise training
General population and those at low to moderate risk of CVD:
-
Exercise training, incorporating a warm up and cool down period, should be performed at moderate to high intensity two to three times per week for 30–40 min each time.
-
The mode of exercise should be aerobic and, where possible, continuous allowing for a steady progression in effort —for example, walking programmes, cycling, jogging, swimming.
-
The time spent exercise training contributes to meeting the 150 min per week physical activity recommendation (above).
Patients with established CVD and those considered at higher risk of CVD:
-
A more structured approach is needed in managing patients, and in all cases assessment and specific goal setting, with risk stratification, delivered by professionals skilled in health related exercise, is preferable.
-
Increase in exercise with community based exercise initiatives are recommended for patients at risk of CVD.
-
Cardiac rehabilitation programmes are recommended for patients with established CVD and in those following a CVD event.
1.5.1 Introduction
Despite the wealth of information on the risk factors which drive the development of CVD and its clinical consequences, the impact on the behaviour of the public and the overall risk profile has been disappointing. The AHA recently introduced a simple seven-point scoring system for the ‘ideal’ CVD health and in subsequent studies almost no subjects achieved the lowest (best) score.65 Similarly, the Health Survey for England (2012) showed that overall 60% of the adult population met the UK guidelines for aerobic physical activity, yet 55% of men and 47% women, in the lowest income quintile, met the guidelines.66
The JBS3 recommendations emphasise the importance of adoption of a healthy lifestyle for future CVD health in the population. The reductions in CVD risk factors from beneficial lifestyle changes, introduced early and sustained over years, result in substantial gains in later CVD outcomes.
The new metrics incorporated in the JBS3 calculator (in addition to 10-year CVD risk) are designed to facilitate communication of the ‘investment in health’ concept and the value of a healthy lifestyle. Services are available to help deliver appropriate behavioural changes (eg, smoking cessation), but more emphasis on a coordinated approach including weight control, diet, and physical activity is required, with long term adherence. Achieving healthier lifestyles for the public remains a challenge and discussions between healthcare professionals and their patients are not sufficient to deliver change at a population level. A recent cost effectiveness analysis in the USA demonstrated that legislation to mandate lifestyle changes (eg, banning smoking in public places, food composition/pricing) is very effective and the medical profession needs to engage closely with other professional groups, health services management, and politicians.67
1.5.2 Smoking cessation: interventions and specialist services
Background
The adverse health impacts of smoking are well established. Smoking remains the single largest preventable cause of morbidity and premature death in the UK, along with being the primary reason for the gap in healthy life expectancy between rich and poor.68 In addition, exposure to SHS (passive smoking) can affect non-smokers’ health, for example, through exacerbating respiratory symptoms and triggering asthma attacks, and increasing the risk of lung cancer, respiratory illnesses (such as asthma), heart disease, and stroke.69–71 Exposure to SHS during pregnancy can cause fetal growth impairment and, increased risk of pre-term birth.72
The evidence is strong and consistent on the health benefits of sustained smoking cessation,73 both recent74 and long term74 (boxes 1 and 2).75 Stopping smoking reduces the risk of many of the conditions associated with smoking. For some conditions, the risk drops soon after quitting towards the level of a never-smoker, but for others, elevated risk remains for >20 years. However, smoking cessation always carries some, often significant, health benefit. Risk depends on the previous duration and intensity of smoking, and varies between those with and without pre-existing evidence of disease; it is therefore advisable to promote smoking cessation as soon as possible rather than after smoking related disease has set in.73 Smoking is an excellent example of a ‘lifetime risk’ factor with duration and intensity related to CVD outcome and benefit from early cessation.
Benefits of smoking cessation within short term of having quit74,76–78
Benefit within days
-
Heart rate drops
-
Carbon monoxide and oxygen levels in blood return to normal (similar to those of never-smokers)
-
Nicotine levels in blood disappear
-
Senses of taste and smell sharpen
Benefit within weeks
-
Risk of sudden death from cardiovascular disease (CVD) event begins to reduce
-
Slows decline in lung function; lung function begins to improve
-
Reduced rates of postoperative complications
-
Low birth weight baby risk drops to normal (if quit occurs before pregnancy or during first trimester)
-
Reduced incidence of respiratory infections; coughing and shortness of breath decreases
-
Reduced severity of asthma attacks
-
Results in improved complexion
Benefits within a few months
-
Symptoms of chronic bronchitis (cough, phlegm, wheezing, shortness of breath) improve
-
Ulcer risk drops (gastric and duodenal)—improved short term healing and reduced recurrence
Benefit within a year of having quit
-
Reduced risk of CVD and respiratory disease, ie, slows progression of heart or respiratory disease and reduces risk of it recurring (coronary heart disease risk is cut by half 1 year after quitting)
-
Mild/moderate chronic obstructive pulmonary disease sufferers: improvement in lung function
Benefits of smoking cessation over medium and longer term of having quit74,76–78
Benefit after several years (5 years or less) of having quit
-
People without CHD: substantial reduction in CHD risk compared with persistent smokers (2–4 years)
-
People with CHD: ∼35% reduction in risk of reinfarction or death (2–4 years)
-
Decline in lung function with age slows to that of never-smokers (within 5 years)
-
Cervical cancer risk falls to that of never-smokers (5 years)
Being quit in the longer term (>5 years) reduces the risk of:
-
lung cancer
-
other cancers (compared with continuing-smokers): eg, mouth, throat, oesophagus (squamous cell rather than adenocarcinoma) and oral cancer, bladder, kidney, pancreas, urinary tract, stomach, larynx
-
COPD: risk of death is reduced after quitting
-
CVD including stroke/cerebrovascular disease, CHD and peripheral artery disease.
CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular disease.
Treatment approaches for the population
Legislation which banned smoking in public places in the UK, as well as in other countries including France and Ireland, resulted in an immediate reduction in the incidence of ST elevation MI (STEMI). For individuals, specialist stop-smoking services offer clients the highest chance of success.
Brief interventions
Brief interventions involve opportunistic advice, discussion, negotiation or encouragement. They are commonly used in many areas of health promotion and are delivered by a range of primary and community care professionals. For smoking cessation, brief interventions typically take between 5 and 10 min and may include one or more of the following:
-
Simple opportunistic advice to stop
-
An assessment of the patient's commitment to quit
-
An offer of pharmacotherapy and/or behavioural support
-
Provision of self-help material and referral to more intensive support such as the NHS Stop Smoking Services.
While the effectiveness of brief interventions might appear small in percentage or absolute terms, the cumulative public health effect can be significant due to the frequency with which individuals have contact with health or social-care staff, and the associated potential for reaching large numbers of smokers in the population over time. In addition, those who are medically referred to smoking cessation services are more likely to be successful than self-referrals.79
The NICE Public Health Guidance on brief interventions and referral for smoking cessation, in primary care and other settings, recommend that everyone who smokes should be advised to quit, unless there are exceptional circumstances.80 People who smoke should be asked how interested they are in quitting, and general practitioners (GPs) should take the opportunity to advise all smokers to quit when they attend a consultation. Those who want to stop should be offered a referral to an intensive support service (eg, NHS Stop Smoking Services). All other health professionals and community workers should also refer people who smoke to an intensive support service where novel approaches, including text based support services, enhance quit rates.
Despite all efforts, however, many individuals are unable or unwilling to quit. There is an increasing market for nicotine alternatives. While all are considerably safer than smoking, there are concerns about some approaches, particularly the use of e-cigarettes (current market >£500 million per year in Europe). These have the potential to ‘re-normalise’ smoking, particularly in the young, and thus remain controversial.
Cost effectiveness of smoking cessation services
As the harm caused by continued smoking is so great, smoking cessation interventions (whether brief interventions, group or individual intensive interventions, or pharmacotherapies) are among the most cost effective interventions available to preserve life,81 particularly relative to other routinely used primary prevention and screening interventions. Smoking cessation remains cost effective, even if an individual has been a smoker for many years.
All of the interventions described above lead to a reduction in the number of smokers, fewer comorbidities, and more quality adjusted life years. Although all smoking cessation interventions are cost effective, those which are especially so include group support (over individual support), brief interventions or behavioural support when combined with pharmacotherapy (over either without pharmacotherapy, or over pharmacotherapy without either type of support, respectively), and varenicline (over other types of pharmacotherapy or placebo).82 Specific information on cost effectiveness of interventions, including those of individual pharmacotherapies, is available from NICE (http://www.nice.org.uk).80 ,83
A study using previously collected data estimated the number of life years saved through the provision of interventions for every 100 000 smokers. This found that using only pharmacotherapy 3750 life years would be saved, but using behavioural support and medication would save 7500–15 000 life years.84
1.5.3 Diet
Background
It is now just over a century since the relationship between diet and CHD was first suggested. Over the last 50 years, it has become apparent that diet may exert effects on CVD through multiple biological pathways, in addition to its effects on lipid metabolism.
Dietary fatty acids
Dietary fatty acids are long chain hydrocarbons that can be separated into four categories: saturated fatty acids (SFA), monounsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), and TFA. Controlled dietary studies have clearly demonstrated that the consumption of SFA leads to increased concentrations of serum TC, LDL-c, and HDL-c, but reduced concentrations of serum triglycerides.85 Historically, there is strong observational evidence for a positive relationship between intake of saturated fat and CHD from ecological and migrant studies,86–88 but more recent data from prospective cohort studies have not confirmed this.
A systematic review involving nine cohorts evaluating 160 673 individuals, and a subsequent meta-analysis of 16 cohorts involving over 214 182 individuals, found no significant relationship between saturated fat consumption and risk of CHD.89 ,90 This lack of an association in the latter meta-analysis may have been due to the unreliability of the dietary data in some of the studies, the inclusion of ‘soft’ coronary endpoints, and confounding due to lack of inclusion of other dietary or serum lipids as covariates.91
There is little direct evidence for the benfits of MUFA in CVD prevention,92 although the protective effect of the Mediterranean diet has been attributed to its low levels of saturated fat and high level of MUFA (principally olive oil) consumption.
PUFAs can be divided into two subgroups: n-6 fatty acids (namely linoleic acid) and n-3 fatty acids (α linoleic acid (ALA)) as well as the long chain eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) derived from fish oils. There is substantial evidence from large prospective cohort studies for an inverse association with CVD outcomes.92–97 In contrast, there are significantly fewer observational data for the cardioprotective effect of the n-3 PUFA α-linoleic acid on CVD outcomes, but there is a likely inverse association.98 However, a randomised controlled study of a Mediterranean diet intervention fortified with ALA was found to be strongly protective in post-MI patients.99
There is, however, good observational evidence that the n-3 fatty acids (derived from fish consumption) are cardioprotective, with epidemiological studies showing that regular fish consumers are at lower risk of fatal CHD, including sudden death.100 A meta-analysis of 13 cohorts from 11 prospective studies confirmed this protective effect, even when fish was eaten only once per week. There was a graded increase in the potentially protective effect with increasing frequency of fish consumption (2–4 times per week was associated with an RR 0.77, 95% CI 0.66 to 0.89). These findings have been supported in two other separate reviews, which showed that consumption of around 20 g fish per day conferred a 5.5–7% reduction in CHD mortality.101 ,102
The consumption of industrial TFA (principally found in commercial baked/fried goods), compared with the consumption of an equal number of calories from saturated or unsaturated fats, increases LDL-c while reducing HDL-c, and results in an unfavourable increase in the TC to HDL-c ratio.85 Adverse findings from epidemiological studies have resulted in legislation in certain countries to reduce or ban TFA use in the food industry. Similarly, NICE guidance on the prevention of CVD, at a population level, recommends introduction in the UK of legislation to ensure that industrially produced TFA levels do not exceed 2% in the fats and oils used in food manufacturing and cooking.103
The increased risk of CHD associated with TFA has been found to be greater than that predicted by changes in the serum lipid profile alone, suggesting that TFA may promote CHD through additional mechanisms, such as a direct pro-inflammatory effect and the induction of endothelial dysfunction.
Naturally occurring TFA constitute a very small proportion of average total energy intake and recent data would not suggest an increased risk of CHD from their consumption.104
Metabolic studies suggest that the effect of dietary cholesterol on serum TC and LDL-c values in humans is modest compared with that of saturated fat105 However, an estimated 15–25% of the population are sensitive to dietary cholesterol (so-called hyperresponders), with around a threefold difference, primarily in the LDL-c response. A systematic review concluded that there was little evidence to support a major association between dietary cholesterol and CHD risk in the general population, with the caveat that it may have a detrimental effect in hyperresponders.106
Alterations in dietary fat consumption
There are several meta-analyses of randomised controlled trials (RCTs) of dietary fat interventions. The first, which was published in 2002, and updated in 2012 (trials involving dietary fat reduction/moderation), showed a relative risk reduction of 14% for CVD events (RR=0.86, 95% CI 0.77 to 0.96,) for dietary fat modification (reduction in saturated fat consumption and replacement with unsaturated fat).107 A separate meta-analysis, in which the dietary intervention was more homogenous —that is, reduction in saturated fat with replacement by PUFA—demonstrated a reduced occurrence of CHD events (MI/CHD death/sudden death) by 19% (RR=0.81, 95% CI 0.70 to 0.95), which is in line with the epidemiological evidence.108 There are no RCT data examining reduction in saturated fat together with replacement by MUFA. The evidence for n-3 fatty acid supplementation has not been supported by recent studies. A recent RCT of an additional daily intake of around 376 mg of the PUFAs EPA and DHA or 1.9 g of ALA did not significantly reduce the rate of major CVD events in patients who had had an MI and who were receiving antihypertensive, antithrombotic, and lipid modifying therapy.109 Similarly, daily supplementation with 1 g of n-3 fatty acids did not reduce the rate of CVD events in patients at high risk.110 Recent meta-analyses of relevant trials have also questioned the benefits of omega-3 fatty acid supplementation in primary and secondary prevention of CVD.111 ,112
Fruit and vegetables
Fruit and vegetables are sources of minerals, vitamins, and fibres. Meta-analyses of cohort studies show that fruit and vegetable consumption is inversely related to risk of CVD.113 ,114 The INTERHEART case–control study found a significant, inverse, and graded association between the intake of raw vegetables, green leafy vegetables, other cooked vegetables and fruits, and acute MI,9 but data on the CVD benefits of fruit and vegetables from RCTs are sparse. The DASH (Dietary Approaches to Stop Hypertension) trial demonstrated that a diet rich in fruit, vegetables, and low fat dairy products reduced levels of total and saturated fat and lowered BP.115 The ‘five a day’ dietary recommendation, however, remains arbitrary.
Glycaemic index, glycaemic load, and added sugar
A meta-analysis of 37 prospective observational studies showed that diets with a high glycaemic index (GI) or glycaemic load (GL) independently increased the risk of type 2 diabetes, heart disease, and breast cancer.116 Regular consumption of sugar-sweetened beverages which have a very high GL have been linked with obesity, type 2 diabetes, and increased CVD risk.116 ,117 Recent epidemiological evidence has linked excessive added sugar intake to future risk for CVD mortality.118 Excessive intake of sugar-sweetened beverages appear to be the biggest contributor to sugar intake in most individuals, and there is now trial evidence to support its reduction to lessen obesity.119 Helping individuals to cut not only their high fat intake, but also their refined sugar intake, could therefore have major health benefits, including lessening obesity and CVD.
Dietary fibre and whole grains
RCTs have demonstrated that soluble fibre has a modest effect on lowering concentrations of serum cholesterol,120–122 and also possibly BP.123 A pooled analysis of 10 prospective cohort studies demonstrated that both soluble and insoluble dietary fibres, from mainly fruit and cereal, were inversely associated with the risk of CHD.124
Whole grains, such as barley, wheat, millet, rice, rye and oats, in particular, tend to have a low GI and are rich in insoluble fibre and antioxidants. A meta-analysis of seven prospective cohort studies showed that an average of 2.5 servings per day of whole grains versus 0.2 servings per day was associated with a 21% (95% CI 15% to 27%) lower risk of CVD events.125 There are no RCT data specifically on dietary fibre or wholegrain consumption in CVD.
Nuts
Nuts are energy-dense foods that are particularly high in unsaturated fat, mostly MUFA. They also contain fibre, minerals, and antioxidants. Regular nut consumption has been associated with lowering of cholesterol,126 and in prospective cohort studies, a reduced risk of both CVD events and mortality.127 These findings recently reinforced by the results of two independent cohort studies in health professionals and nurses.128
Salt
Strong observational evidence supports the relationship between dietary salt consumption and BP levels.129 A reduction of sodium intake, especially in the form of sodium chloride, has been shown to reduce BP,130–132 and is additive to the more comprehensive dietary intervention used in DASH.133 Data from long term follow-up of two trials of sodium reduction also suggest a beneficial effect on CVD outcomes.134
Dietary advice to reduce salt intake, however, may have only limited impact and is difficult to maintain in the longer term.132 Legislation directed at the food industry to reduce salt concentrations in processed foods is likely to be more effective in achieving sustained reductions in BP across the whole population, although individual reduction of risk would be small.
Alcohol
Alcohol consumption ranging from 1–3 alcohol units per day (a unit equates to about 80 mL of wine, 250 mL of normal strength beer, and 30–50 mL of spirits) is associated with the lowest all-cause mortality, which is largely due to lower coronary mortality.135 ,136 This relationship is observed in both the general population and in those with established CVD.137 Optimum consumption is lower for women than for men.
There is a clear relationship between alcohol and BP elevation, with systolic and diastolic BP levels increasing as alcohol consumption increases above 3 units per day. Similarly, the risk of cardiac arrhythmias, cardiomyopathy, sudden death, and haemorrhagic stroke also increases above this level of alcohol consumption.138 ,139 The pattern of alcohol use has an effect on CVD risk; binge drinking is associated with a higher risk of sudden death140 and stroke.139 ,141 Although there is no clinical trial evidence on alcohol consumption and CVD, 1–3 units of alcohol per day may be considered safe, although it should be noted all evidence is based on observational data, and therefore the potential for confounding remains. The evidence is therefore insufficiently robust to recommended commencing alcohol intake for CVD risk prevention in current teetotallers.
Plant stanol/sterol esters
Stanols and sterols appear to offer a similar degree of LDL-c reduction (approximately 10%),142 even with concomitant statin use.143 Although there is no CVD outcome data for such products (and never likely to be), it is reasonable to postulate a beneficial effect on CVD outcomes based on the LDL lowering hypothesis.144
Vitamin supplementation
RCTs of vitamin supplementation, such as α tocopherol, vitamin E, vitamin C, β carotene, and retinol, have shown no benefit in either primary or secondary prevention of CVD events.145–147 Similarly, RCTs of homocysteine lowering through use of folic acid supplements/B vitamins have shown no benefit.148–151
A large RCT of calcium and vitamin D supplementation did not show a decrease in CVD events in healthy postmenopausal women.152 A growing body of evidence suggests that low vitamin D values in the vast majority of people may reflect, or be a consequence of, other adverse lifestyle factors such as obesity and smoking, rather than necessarily being a causal risk factor.153 ,154 The ongoing VITAL RCT of vitamin D supplementation will be the first to examine specifically whether vitamin D supplementation (it also includes an omega-3 arm) can lower CVD risk, and any recommendations on benefits or otherwise on CVD risk of vitamin D supplementation should await the results.
Dietary patterns
While it is important to understand the contribution of the above micronutrients to CVD, it is difficult for clinicians, let alone patients, to gauge with accuracy their daily consumption of saturated fat, salt, fibre, etc. Dietary advice based on specific dietary patterns, such as the Mediterranean diet or DASH diet, which advocate specific macronutrients or whole foods rather than concentrating on micronutrients, may therefore be more useful in the clinical setting.
The Mediterranean diet is comprised of abundant plant foods (ie, fruit, vegetables, cereals, beans, nuts and seeds), with olive oil as the principal source of dietary lipids, a low consumption of red meat and low to moderate consumption of dairy products and wine (usually with meals).155 A recently reported RCT (PREDIMED) tested the potential for such a diet to reduce CVD events in patients at elevated CVD risk. The multivariable adjusted HRs were 0.70 (95% CI 0.54 to 0.92) and 0.72 (95% CI 0.54 to 0.96) for groups assigned to a Mediterranean diet with extra-virgin olive oil and a group assigned to a Mediterranean diet with nuts, respectively, versus a control group.156
1.5.4 Physical activity and exercise
Background
There is considerable evidence for the impact of physical fitness and physical activity status on CVD risk profiles and outcomes. A sedentary lifestyle adversely influences CVD rates and a more intensive approach, aimed at incorporating physical activity and exercise into daily life, is needed.157–160 Physical inactivity is the fourth largest risk factor for premature death158 and, until recently, physical activity status and fitness levels have not featured in CVD prevention risk models. Recent evidence, including RCTs, meta-analyses, and epidemiological studies, has strengthened the case for their future inclusion.157 ,159 ,161–163
Physical fitness and activity status as part of CVD risk prediction
Physical fitness: There is sufficient evidence for the use of physical fitness levels as a determinant in CVD risk estimation:
-
Physical fitness levels above 7 metabolic equivalents (METs) and up to 10.6 METs is associated with the lowest CVD risk
-
A one MET increase is equivalent to a 14% reduced risk in premature CVD death.
The MET is a unifying expression of fitness that defines peak levels of activity, as multiples of the energy cost, above that required to maintain a seated position at rest. One MET (or 3.5 mL of oxygen per kilogram of bodyweight per minute) is equal to the amount of oxygen used each minute during seated rest. Walking, at a natural cadence, is equivalent to 3 METs or three times the energy cost of sitting, whereas jogging is equivalent to 7 METs.
Fitness (or exercise capacity) is often measured directly using treadmills or cycle ergometers, which enable physical fitness units (eg, time, speed, gradient, load, and distance) to convert to METs. There are compendiums outlining MET costs for all types of physical activity that can help clinicians tailor physical activity and exercise training prescriptions.164
NICE guidelines recommend the following for physical activity:165
-
Over a week, this should add up to at least 150 min (2.5 h) of moderate intensity physical activity in bouts of 10 min or more.
-
Alternatively, comparable benefits can be achieved through 75 min of vigorous intensity activity spread across the week or combinations of moderate and vigorous intensity activity.
-
All adults should also undertake physical activity to improve muscle strength on at least 2 days a week.
-
They should minimise the amount of time spent being sedentary (sitting) for extended periods.
There is recent evidence that certain ethnic groups (eg, South Asian men) may benefit from higher levels of physical activity to improve CVD risk profiles.166
Physical activity status plays a significant role in predicting CVD risk over time. If someone is physically active at the recommended level, they are much less likely to suffer a premature CVD event.159 ,161 Physical activity status (eg, frequency and duration of activity) has been successfully measured using motion devices (eg, pedometers or accelerometers). Alternatively, Leisure Time Physical Activity (LTPA) and sedentary behaviour questionnaires have been successfully used to assess the impact of interventions.
NICE guidance concludes that physical activity:165
-
Prevents and helps to manage conditions such as CHD, type 2 diabetes, stroke, mental health problems, musculoskeletal conditions, and some cancers.
-
Has a positive effect on wellbeing, mood, sense of achievement, relaxation, and release from daily stress.
In 2007, Haskell et al159 reviewed the evidence and concluded that physical activity interventions were effective, in adults, in the short term. In 2013, Shortreed et al161 investigated the impact of long term physical activity compared to long term inactivity on CVD risk, all-cause mortality, and CVD related mortality using Framingham observational data collected over 40 years. Over time, long term physical activity had a protective effect (stronger in men than women) seen through a lower incidence of all-cause and CVD related mortality compared with physical inactivity.
Cardiac rehabilitation and prevention programmes are proven interventions that improve health related lifestyle outcomes in people with established CVD,167 ,168 and improve risk profiles in those at risk of CVD.169 ,170 The evidence for physical activity and exercise training is presented in figure 29 where it is shown that moderate to high intensity, longer duration approaches are most beneficial.
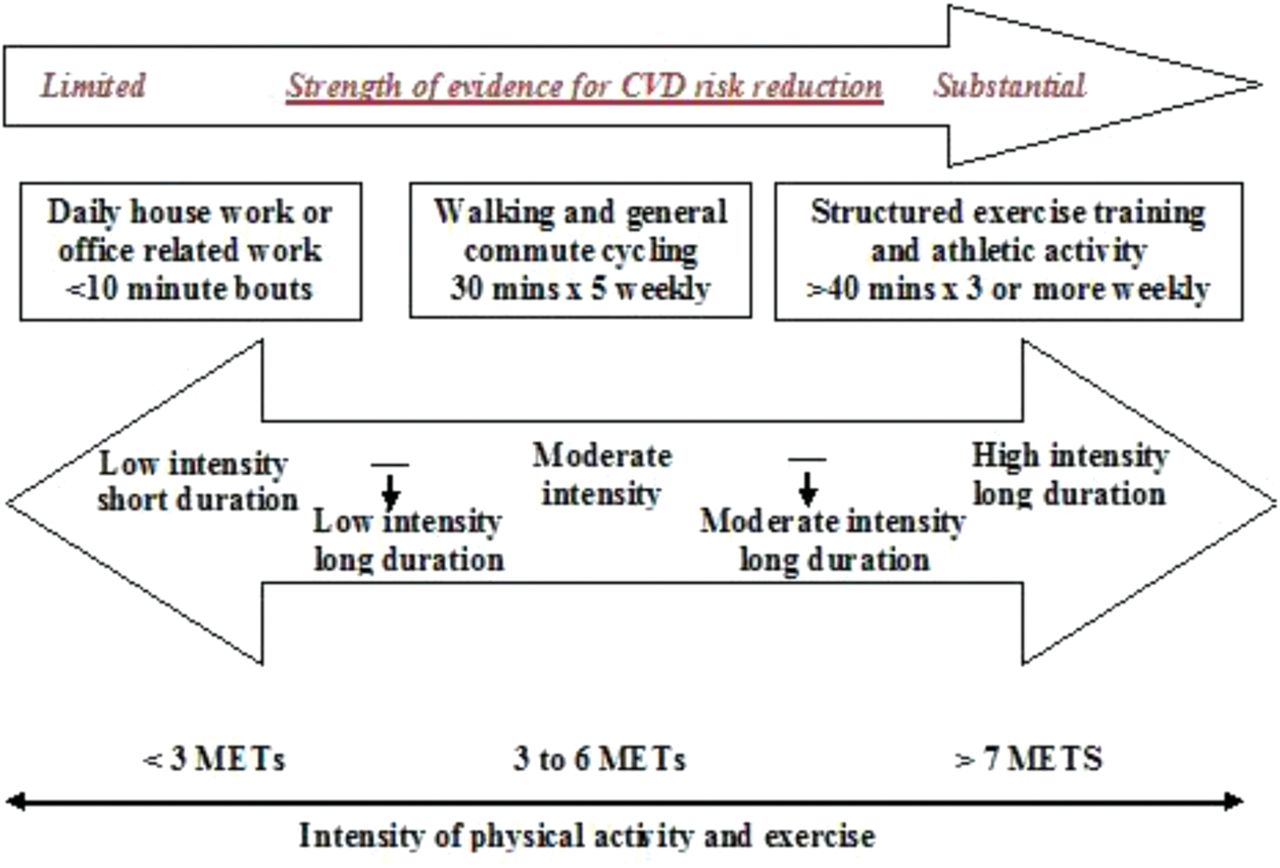
Cardiovascular disease risk reduction associated with physical activity and exercise training. CVD, cardiovascular disease; METs, metabolic equivalents.
Treatment approaches
Brief advice on physical activity, exercise on referral, and community based exercise initiatives have been used successfully in the general population and in those at low to moderate risk of CVD.159 ,165 ,167 The major emphasis from these guidelines is to reduce the amount of time spent in prolonged static sedentary activities (such as sitting at a computer or watching TV). Where sitting is part of an individual’s working life or leisure time it should be interspersed with regular periods of movement.
Exercise training this should be performed at moderate to high intensity, three times per week, for 40–50 min each time. The mode of exercise should be aerobic and continuous, thus allowing for a steady progression in effort —for example, walking programmes, cycling, jogging, swimming, or circuit based exercise and resistance training.
In patients with established CVD and those considered at high risk of CVD, the intensity of exercise training should be moderate and performed three times per week for 30–40 min each time. Exercise intensity is best guided by using heart rate within the range of 60–80% of maximum or ‘moderate to hard’ (but not strenuous) scores on routinely available rating of perceived exertion scales.168–170
Recent NICE guidance, for patients following MI, recommends lifestyle change, including regular physical activity, plus attendance and completion of cardiac rehabilitation.171 The British Association for Cardiovascular Prevention and Rehabilitation (BACPR) have published minimum standards and agreed a set of core components that recommend all eligible individuals are assessed early, treatment goals are tailored and agreed by patients, and that reassessment occurs following the intervention.172 The model of CVD prevention and rehabilitation proposed in JBS3 reflects the position of the Department of Health and BACPR and is also applicable as part of a wider CVD prevention and chronic disease management based strategy. This approach emphasises the multifactorial nature of lifestyle advice and the importance of an integrated and sustainable approach.
1.5.5 Summary
-
Prolonged sedentary activity should be reduced and interspersed with regular breaks that incorporate physical activity.
-
Fitness levels and physical activity status are important in understanding CVD risk profiles and mortality trends.
-
When combined with CVD risk scores, physical fitness improves the predictive capability of the estimation in terms of risk reduction and mortality benefit.
-
Physical activity and exercise training approaches make a significant contribution to CVD risk reduction and should be included as part of a lifestyle approach.
1.6 Childhood and adult obesity
Recommendations
-
Multidisciplinary approaches to obesity management in children and young people are required with a ‘lifetime risk’ message. These may include interventions during the early postpartum period, as well as regular monitoring of childhood weight and family counselling.
-
With appropriate training, all healthcare professions should be able to Ask and Assess adiposity and Advise appropriate adult patients on evidence based ways to target weight change.
1.6.1 Obesity in children
Background
JBS3 recommendations for CVD risk assessment and management focus, appropriately, on adults, but it is clear that a major threat to the future health of the nation comes from the alarming increase in adiposity and obesity levels among children and adolescents. This is well documented in the National Child Measurements Programme Report of Changes in Children's BMI between 2006/7 and 2011/12.173 One third of the children in the UK are now overweight or obese, and four out of five teenagers will become obese adults. Furthermore, the socioeconomic and ethnic distribution of obesity (which is more prevalent in lower socioeconomic groups) may exacerbate inequalities in future CVD and life expectancy.
There are a number of compelling reasons to tackle childhood adiposity/obesity and to discuss this issue in JBS3. Obese children have a greatly increased risk of becoming obese adults and this is determined and reinforced by tracking of health related behaviours such as diet and exercise.174 Childhood adiposity has the same relationship with CVD risk factors as that seen in adults. Increasing BMI is accompanied by a rise in inflammatory markers and non-HDL-c, and a fall in HDL-c together with a rise in systolic BP. This is not confined to obese children and there is a continuous relationship across the whole adiposity spectrum in the young.175 In particular, there is a strong association between childhood adiposity levels and risk of type 2 diabetes, which can now occur even before puberty. Thus, the cardiovascular consequences of childhood obesity are largely those of adult obesity, with even more impact because of prolonged exposure to excess fat.176 Recent prospective evidence has confirmed that childhood obesity adversely affects both CVD morbidity and mortality and all-cause mortality, mediated predominantly by metabolic and BP effects.177
In the populations of developed countries, such as the UK, the obesity epidemic in the young threatens to undo the CVD benefits which have resulted from the enormous joint efforts of the medical profession, healthcare providers, and politicians to reduce exposure to other major CVD risk factors such as smoking. Furthermore, childhood obesity is not confined to developed nations and the current worldwide increases in obesity are likely also to exacerbate the growing epidemic of CVD in the developing world.178
Mechanisms
The increase in childhood obesity reflects a major change in lifestyle with a decline in levels of physical activity, and thus energy expenditure, together with an increase in calorie intake, with emerging evidence (across all age groups) favouring excess intake of calories being more important.179 There is also evidence that weight trajectories, CVD risk factors, and complications may be programmed in fetal or early postnatal life.180 ,181
Treatment
Tackling childhood obesity is a major health opportunity. Efforts to encourage weight loss should focus on the young, in whom lifetime behaviour patterns become established and in whom dietary change and exercise are practical.183 Furthermore, at this stage of life, the beneficial consequences of weight loss (including BP lowering and resolution of insulin resistance) are likely to translate into leveraged gains in later CVD outcomes. Medical attention usually focuses on children with severe obesity but, in common with other CVD risk factors, the future burden of CVD will be predominantly among individuals with lesser degrees of obesity. New evidence from observational data suggests that early success in restoring normal weight in overweight or obese children may return their future levels of CVD risk to those seen in individuals who have normal BMIs throughout their life.182 The solutions to the problem, however, are not straightforward. There are complex ethnic, wealth, and behavioural relationships with obesity and many parents are ‘in denial’ about their children being too fat. The results of diet regimes in children have been very disappointing and family based programmes appear to be more successful.184 Teaching adults to take responsibility for their own CVD health will thus have an additional favourable impact on their children.
The medical profession needs to play a major role in promoting the JBS3 message of ‘lifetime investment in CVD health’, but will need to work in partnership not only with individuals and their families but also with a broad range of other groups who are concerned about public health. Changes to the school curriculum to ensure protected time for sport and recreation, and review of school meals, transport links, and the broader environment of the increasingly urbanised population, will be required. Lifestyle services for management of overweight and obesity in children and young persons are the subject of a NICE public health guidance.185 This has developed and proposed a structured approach to lifestyle management in the young which will require central funding. Politicians will need to support these efforts further, as evidence is accumulating that legislation on food composition, taxation, and marketing of calorie-dense food and drinks to children may be the best and most cost effective way to achieve sustainable improvement of population levels of adiposity.67 ,186 Physicians should take every opportunity to discuss the importance of adiposity with their patients and their families and provide a sensitive but clear message.
Timely interventions during the early phase of development may lead to improved lifetime health and present an exciting new opportunity to benefit public health. Pregnant women should not smoke and excessive gestational weight gain is a further risk factor for childhood obesity. Two postnatal factors—duration of breast feeding and sleep during infancy—may also be important. A difference in the prevalence of obesity ranging from 4% to 28% in children aged 7–10 years has been reported, depending on the presence or absence of these four factors.187
Pregnancy and infancy are good opportunities for education and intervention, as women are willing to modify behaviour during these relatively brief periods and medical/nursing contact is frequent. If an obese girl grows up to be an obese adult and becomes pregnant, the ‘vicious cycle’ may repeat. Thus targeting maternal behaviours (including diet and weight gain) and postnatal feeding may result in important public health benefits. Several large scale trials are in progress and the findings will have an impact not only on obesity prevention but also on other health outcomes.188
1.6.2 Obesity in adults
While there are no randomised trials demonstrating that obesity reversal or prevention lessens CVD, evidence from bariatric surgery,189 and more recently genetic studies,190 confirms that obesity is a causal risk factor for CVD. There is also recent evidence that obesity is causally linked to diabetes, hypertension, and abnormal lipids.191 Thus, prevention or treatment of obesity in adults remains an important means to lessen CVD risk. A discussion about obesity is possible anytime a heathcare professional (HCP) meets a patient, and in general, the HCP should take the following approach, which could be summarised as the 3A's. They should first Ask patients if they are happy and ready to discuss their weight, and potential interventions if required, as not all patients will be. If patients are happy to discuss, the HCP should Assess their BMI and then give Advice on the potential courses of action, dependent on the patients measured BMI and levels of comorbidity. Several clinical guidelines, for example, NICE CG43,185 ,192 ,193 exist for management of obesity in adults and HCPs are directed to these. It should also be recognised that some commercial weight loss providers can be superior to the NHS in helping patients lose weight,194 thereby providing another potential resource for evidence based weight management.
1.6.3 Summary
-
While a large proportion of adults are overweight or obese, the increase in population levels of obesity has been fastest in children and young adults.
-
Childhood obesity:
-
Tracks to adult obesity
-
Disturbs metabolic profile and BP, even over ‘normal’ BMI ranges
-
Accelerates development of type 2 diabetes
-
Is associated with premature CVD and death.
-
-
Prenatal and early postnatal factors may ‘programme’ higher risk of childhood obesity and permanently alter morbidity and mortality in adult life.
-
Early weight restoration may normalise CVD risk.
-
Physicians need to play a major role in multidisciplinary approaches to obesity management in children and young adults with a ‘lifetime risk’ message.
-
Obesity in adults leads to CVD risk in large part by affecting lipid values, BP, and diabetes risk. Targeting of adult obesity to lessen CVD is an important goal for many individuals.
-
With appropriate training, all healthcare professions should be able to Ask, Assess and then Advise patients on evidence based ways to target weight change.
Section 2: high risk of cardiovascular disease
2.1 Lipids
Recommendations
-
Non-fasting blood samples should be taken to measure TC and HDL-c. The JBS3 risk calculator enables entry of these two measures and it is expected that non-HDL-c (TC minus HDL-c=non-HDL-c) will replace LDL-c in clinical practice as well as in clinical trials.
-
All high risk people should receive professional lifestyle support to reduce TC and LDL-c, raise HDL-c, and lower triglycerides and to reduce their cardiovascular risk.
-
Cholesterol lowering drug therapy is recommended in:
-
Patients with established CVD
-
Individuals at high risk of CVD: diabetes >40 years, patients with CKD stages 3–5, or FH
-
Individuals with high 10-year CVD risk (threshold to be defined by NICE guidance)
-
Individuals with high lifetime CVD risk estimated from heart age and other JBS3 calculator metrics, in whom lifestyle changes alone are considered insufficient by the physician and person concerned
-
-
Statins are recommended as they are highly effective at reducing CVD events, with evidence of benefit to LDL-c values <2 mmol/L which justifies intensive non-HDL-c lowering.
-
Statins are safe with trial evidence showing no effects on non-cardiovascular mortality or cancer. There is a small increase in risk of developing diabetes, but the benefits of cholesterol lowering greatly exceed any risk associated with diabetes. If statin intolerance develops a stepwise strategy involving switching agents and re-dosing is recommended.
-
Despite low HDL-c values contributing to CVD risk, drug therapy to raise HDL-c has not been shown to reduce CVD risk and is not currently indicated.
2.1.1 Background
There is a continuous relationship between cholesterol concentrations and CVD risk. This is principally determined by values of TC and HDL-c, both in people with and without CVD. The absolute benefit of cholesterol reduction is related to the level of baseline CVD risk. Compelling evidence for cholesterol lowering comes from statin trials in a range of populations with varying levels of CVD risk.
A Cholesterol Treatment Trialists (CTT) collaboration meta-analysis, based on data from 170 000 participants in 26 RCTs, showed that standard statin regimens typically reduce LDL-c by approximately 30%, but that using either higher doses of traditional statins or utilising newer, more potent statins may reduce LDL-c by up to 50%.11 These most recent analyses show that further reductions in LDL-c (down to between 1 and 2 mmol/L) reduce the incidence of CVD events, and there is no heterogeneity in treatment effect in trials of statins versus placebo, and in the ‘more versus less intensive’ statin trials. The reduction in major CVD events is directly proportional to the absolute LDL-c lowering, with similar relative benefits across the distribution of LDL-c even when the starting LDL-c is already <2 mmol/L. Overall, for a 1 mmol/L reduction in LDL-c a 22% proportional reduction in major vascular events was observed. For a 2 mmol/L reduction in LDL-c a 40% proportional reduction was observed, while a 3 mmol/L reduction resulted in a 50% proportional risk reduction. There was no evidence that such reductions in LDL-c resulted in any adverse events, including haemorrhagic stroke, nor any adverse effect on cancer incidence. This, together with the good safety profile for most statins, supports the use of higher doses of statins in individuals who have sufficient CVD risk to warrant drug therapy.
2.1.2 Treatment approaches
Lipid assessment
All adults from 40 years should have their TC and HDL-c measured on a non-fasting blood sample as part of a CVD risk assessment in primary care. Where FH is suspected, a subsequent fasting sample to enable LDL-c estimation may be required.
Currently statin therapy has been recommended in those who have a 10-year absolute CVD risk of ≥20%. This threshold was developed at a time when many statins were under patent protection and had uncertain safety and efficacy. Approaches to broaden the prescription of statins to those at lower risk levels have been prompted by accumulating evidence for their safety and efficacy. A radical suggestion to reduce the statin prescribing threshold from 20% to 7.5% in the recent AHA/ACC guidelines has been controversial. Updated NICE guidance is anticipated which will review lowering the UK risk threshold for statin use, based on impact, cost effectiveness, and practicality.
Where possible, at least one repeated measurement of lipids is advised before initiating drug therapy. Secondary causes of elevated lipids should be considered before drug treatment is given, and these include alcohol abuse, diabetes, renal disease, liver disease, and hypothyroidism. Lifestyle advice should be given and lipids monitored to assess the effects of changes in diet and physical activity.
Those who are not found to be at high CVD risk, or who are started for other reasons on drug therapy to lower BP, lipids or glucose, should have their lipids and risk assessment repeated, ideally every 5 years.
Acute coronary syndromes, major surgery, and other vascular and acute inflammatory events result in lowering of TC and HDL-c (triglycerides may rise). This generally lasts <6–8 weeks, but can be longer if the event is severe. Despite this, non-fasting lipids should still be measured as soon as possible in the acute phase to determine whether the patient could have FH, prompting screening of first degree relatives. Lipids should be measured about 8–12 weeks following the acute event while on statin therapy to assess if adequate control of non-HDL-c has been achieved. Secondary causes of elevated lipids, where these have not already been fully investigated during the hospital admission, should be considered at the same time.
In people with established CVD, or diabetes mellitus, or who are above the threshold for treatment based on 10-year risk of developing CVD, the non-HDL-c value should be lowered to <2.5 mmol/L (which is broadly equivalent to an LDL-c of <1.8 mmol/L). Statins will lower non-HDL-c and LDL-c by about the same amount, as their primary action is on LDL-c with only minor effects on HDL-c.
Measurement of transaminases (alanine aminotransferase (ALT) or aspartate aminotransferase (AST)) is recommended before statin treatment and again within 3 months (when lipids are assessed) to rule out significant liver dysfunction. It should be noted that non-alcoholic fatty liver disease (NAFLD) is not a contraindication for statin therapy. It is common practice to measure baseline creatine kinase (CK) before starting treatment with a statin as some people may have high CK values that are physiological rather than pathological. If CK is normal, further measurements are not indicated, unless the person develops symptoms. Acute myopathy, progression to non-fatal or fatal rhabdomyolysis, is extremely rare.
HDL-c is inversely related to the risk of CVD, but there is no treatment target for HDL-c. CVD risk rises with elevation of triglycerides, especially when HDL-c values are low, but there is no treatment target for triglycerides. Triglyceride level does not add to CVD risk once cholesterol and HDL-c are factored in.
Management of blood lipids
Several treatment strategies have been proposed for the management of lipids including ‘the lower the better’, ‘fire and forget’, and ‘treat to target’—the latter being the recommendation of JBS1 and JBS2.3 ,4
There is now good evidence for a benefit of LDL-c lowering to below previous targets. This supports a more intensive strategy to achieve non-HDL-c of <2.5 mmol/L and/or LDL of <1.8 mmol/L.
Previous NICE guidance recommended a ‘fire and forget’ policy of simvastatin 40 mg for primary prevention in high risk individuals. This has limitations. Firstly, patients with high pretreatment LDL-c values may not get the maximum benefit from lipid lowering. Secondly, patients may need follow-up to ensure adherence to prescribed therapy. This choice of statin and approach to treatment is under review.
In JBS3, a non-HDL-c measure is proposed as evidence is accumulating that this provides better prediction of risk and treatment response than LDL-c. This is particularly relevant in the increasing number of patients with type 2 diabetes in whom an increase in atherogenic lipoproteins is not reflected by LDL-c values. Non-HDL-c is a sum of cholesterol contained in all atherogenic ApoB lipoproteins (LDL-c and VLDL-c), whereas ApoB is a measure of the number of LDL particles. Not surprisingly, these two measures are highly correlated. Furthermore, a recent meta-analysis in statin treated patients showed that non-HDL-c had the strongest association with CVD events and that changes in non-HDL-c explained the largest proportion of the CVD protective effect of statin intervention. Measurement of non-HDL-c has practical advantages: (1) it can be simply calculated by subtraction (unlike LDL-c which requires a more complicated calculation using the Friedewald formula); (2) there is no need for a fasting sample as the strength of associations is unaffected (whereas the Friedewald formula includes triglycerides which need to be measured on a fasting sample); and (3) it represents the TC circulating in both LDL-c and other apolipoprotein B containing triglyceride rich particles. Measurement of ApoB concentrations is an alternative but is less commonly available, more costly, and harder to standardise. Any potential superiority over non-HDL-c (not established) is not felt sufficient to justify its routine use. A non-HDL-c concentration of <2.5 mmol/L is broadly equivalent to an LDL-c of <1.8 mmol per litre and this value should be achievable in most patients. Failure to do so warrants checks on adherence and investigation of potential factors which might attenuate response to statins (such as alcohol, drugs, or underlying diseases). The full effect of statin treatment is typically seen 6–8 weeks after initiation or titration of the dose and blood lipid monitoring promotes adherence. A pragmatic approach is to recommend an annual non-fasting TC and HDL-c measurement once the patient is established on an effective maintenance dose of a statin.
When to start lipid lowering therapy
People with established CVD
All people with established CVD (coronary, cerebral, and peripheral), but not cerebral haemorrhage, should be prescribed a statin in hospital regardless of the initial non-HDL-c value. The rationale for this policy is as follows. Firstly, trials of early initiation of statin treatment show evidence of early CVD benefit. Secondly, the vast majority of such people will have a high non-HDL-c value ≥2.5 mmol/L. Thirdly, measurement of lipids in the acute phase of the disease will usually underestimate pre-disease values, and so even a relatively low non-HDL-c in the acute situation is not a reason to delay treatment with a statin. Fourthly, it emphasises to the person with the CVD the importance of lipid lowering for their future CVD health. Finally, starting treatment in hospital is more likely to result in the same treatment being continued in general practice.
Statin use in people with diabetes
Statin recommendations for patients with type 1 and type 2 diabetes are provided in the diabetes section. Statin use is associated with a modest, but statistically significant, overall increase in the odds for new-onset diabetes (∼10% compared to placebo or usual care).195 More intensive statins appear to increase risk further.196 However, statin therapy reduces major CVD event rates in all patients, regardless of their risk level for diabetes or whether they have existing diabetes or, indeed, develop diabetes. Importantly, in all cases, whether in primary or secondary prevention, several CVD events are prevented for each excess case of diabetes associated with statins.195 ,196 Thus, statins should continue to be recommended, with appropriate monitoring and guidance, for lowering non-HDL-c in patients with and without diabetes or risk factors for diabetes. Patients eligible for statins but considered at high risk of diabetes should have a pre-statin check on glycaemia status (fasting blood glucose (FBG) or HbA1c) which could be repeated 3 months after commencement of statins. All patients without diabetes who are eligible for statins should be informed of the very slight diabetes risk, but that this risk is far outweighed by the CVD benefits. Patients should also be told that adopting lifestyle changes will not only further lessen CVD risk on top of statin but will help mitigate any slight diabetes risk.
People at high risk of developing CVD
For high risk individuals with no history of CVD, new NICE guidance will recommend the threshold for statin therapy based on 10-year risk. For others, the JBS3 risk calculator will allow an informed decision on the need for statin therapy where lifestyle interventions alone have been insufficient. An intensive statin dose should be prescribed with no difference from the approach taken in patients with established CVD.
Familial hypercholesterolaemia
FH is an autosomal dominant disorder caused by mutations in at least three separate genes for the LDL receptor, apolipoprotein B and PCSK9. All result in elevation of LDL-c (of varying degree) and premature CVD. Historically, if untreated, clinical complications in heterozygotes frequently manifest in men in the fourth decade and women in the fifth decade. The Simon Broome registry in the 1980s, before statins, identified a 100-fold increase in CVD mortality in young adults with FH, aged 20–39 years.
Statin therapy has resulted in a substantial decline in CVD mortality in FH. A large meta-analysis of 26 randomised clinical trials in non-FH patients demonstrated incremental benefit from intensive statin treatment compared to less intensive regimes. All-cause mortality was reduced by 10% per 1.0 mmol of LDL-c lowering. FH therefore represents a major opportunity for improvement in CVD outcomes from lifetime lowering of LDL-c. CVD risk estimation is not required in FH.
Homozygous FH is present in approximately 1 in a million and results in extremely aggressive CVD. These rare patients require specialist treatment, which may include lipid apheresis. Early diagnosis of FH is crucial, but it is thought that >80% of cases remain undetected. The prevalence of heterozygous FH in the general population may be higher than the figure of 1 in 500 which is often quoted, with considerably higher rates in some populations. The clinical diagnosis is based on family history, clinical findings, and cholesterol concentration which are used in the Simon Broome registry and in the Dutch Lipid Criteria to classify patients into definite, probable, and possible FH. Individuals who fall within the clinical categories of definite or probable FH should be offered genetic testing. Genetic testing may give a definite diagnosis, by detection of a pathological mutation, and NICE has endorsed the clinical benefits and the cost effectiveness of this approach. Once FH has been diagnosed, cascade screening of families should be undertaken using clinical and genetic testing. This has proved very effective in a national programme in Holland and a similar strategy is currently being undertaking by several other countries including Wales, Scotland, and Northern Ireland. There has been, however, patchy uptake of systematic screening in England, and funding from the British Heart Foundation is trying to address this.
Treatment
The diagnosis and management of FH patients should involve referral to specialist lipid services. Current guidelines recommend reduction in LDL-c of at least 50%, with the aim of reaching LDL values found in the general population. If this cannot be achieved, the use of maximum therapy without side effects is recommended. There is uniform consensus that statins are first line treatment for lipid lowering and can lower risk of CVD in heterozygous FH by up to 80% when started early. Despite intensive regimens, however, cholesterol values remain elevated in many patients, with almost half failing to achieve >50% lowering of LDL-c and only 21% reaching LDL-c concentrations of <2.5 mmol. Statins may be combined with ezetimibe and bile acid sequestrants, but there is no evidence currently for decreased CVD events using combination therapy.
Even with current combination therapies, cholesterol values remain high in around one third of patients, emphasising the need for new treatments to decrease LDL-c values further. This is an exciting area of drug development and several promising new classes of drugs are under evaluation. PCSK9 has emerged as a pivotal regulator of LDL-c and can be lowered by antisense molecular based therapy, monoclonal antibodies, and small interfering RNAs. Clinical studies have shown substantial LDL-c lowering on top of statins, and several outcome trials are in progress. Other pharmacological approaches to lower LDL-c are being tested in FH patients.
Lifestyle changes including smoking cessation, regular physical activity, weight and BP control should be emphasised, together with adherence to dietary guidelines.
Lifetime lowering of LDL-c is indicated from diagnosis, even in childhood, with pharmacological interventions usually required to supplement lifestyle measures. A statin is first choice in children from age 8 years as there is solid evidence that atherosclerosis begins in childhood and that its progression is slowed by early lowering of LDL-c. If, however, parents are concerned about starting children on statins before puberty, testing for FH early, with commencement of statin therapy after puberty, is a reasonable alternative.
Familial combined hyperlipidaemia
Familial combined hyperlipidaemia (FCH) comprises a heterogeneous group of lipid disorders of variable inheritance pattern. They are characterised by raised cholesterol and/or triglycerides, and premature CVD in family members. For more information visit PRODIGY (http://www.prodigy.nhs.uk). People with FCH and their families should also be managed by lipid specialists.
Drug therapy
Statins
Numerous randomised clinical trials have shown benefits of lowering LDL-c, and statins are the first line therapy for most patients. Adverse event rates are uncommon and the benefit/risk ratio is extremely high. Simvastatin has been recommended up to now, by NICE because of its cost effectiveness after patent protection was lost. Since JBS2 however, atorvastatin is now off patent and is now considered first line therapy. This applies especially to the higher doses in acute coronary syndromes, where the evidence base for benefit is predominantly for atorvastatin 80 mg. Furthermore, simvastatin 80 mg has been shown to have a significantly increased rate of myopathy and rhabdomyolysis and should not therefore be used.
Statin intolerance
Statins have proved remarkably free of side effects in randomised clinical trials, but in clinical practice, statin intolerance can be an issue.197 It is usually due to myalgia but the incidence is hard to quantify. Before a patient is diagnosed as truly statin intolerant, the following stepwise therapeutic approach for a patient who requires therapy but is apparently intolerant of simvastatin 40 mg or atorvastatin 40–80 mg daily is recommended. This should be followed if they experience myalgic symptoms (sufficient to reduce their quality of life to stop taking the statin), or a rise in CK (>5 times the upper limit of normal (ULN)) which then improves after cessation of the therapy.
-
Ensure that no contraindications or drug interactions exist for the chosen statin which could explain the development of symptoms.
-
Challenge the patient with simvastatin 10 mg or atorvastatin at 10 mg daily dose, using a statin that the patient has not previously taken. If tolerated, the dose can be gradually increased as required.
-
If not tolerated, prescribe low dose pravastatin (10 mg/day) or rosuvastatin (5 mg/day). If myalgic symptoms have been severe or accompanied by elevations in CK, rosuvastatin can be prescribed at a reduced frequency (eg, rosuvastatin 5 mg every second day, or even once weekly) and then titrated up, as required, if no side effects occur.
-
If unable to tolerate any statin, or if the cholesterol is considered inadequately controlled on the achieved statin dose, consider the addition of a bile acid sequestrant or ezetimibe 10 mg daily.
-
Failure to establish statin therapy in a patient with established CVD or with suspected FH, or a rise in CK >5× ULN on a statin, requires specialist lipid advice.
Coenzyme Q supplementation in patients with statin related muscle symptoms is not recommended.198
Combination therapy
Other lipid lowering drugs for further non-HDL-c lowering may be needed in some people, usually in combination with a statin or in place of a statin (statin intolerance). In contemporary clinical practice in the UK, the most commonly used combination therapies involve statin plus either ezetimibe, a fibrate or, until recently, nicotinic acid.
Ezetimibe
Ezetimibe monotherapy lowers LDL-c modestly (approximately 18.5%) and has very little effect on other lipoproteins. Study of Heart and Renal Protection (SHARP) was the first study to demonstrate that the combination of ezetimibe and simvastatin 20 mg reduced the incidence of major CVD events in patients with CKD. The IMPROVE- IT trial is testing the effect of simvastatin alone or in combination with ezetimibe 10 mg after acute coronary syndrome.199
Bile acid sequestrants
The anion exchange resins, cholestyramine and colestipol, bind bile acids in the intestine. This results in increased LDL-c receptor activity in the liver which increases the clearance of LDL-c from plasma. RCTs have shown that this class of drug reduces non-fatal and fatal coronary events. In people who can tolerate resins, treatment may be appropriate if there is severe elevation of LDL-c, as in FH.
New therapies
New approaches to lowering LDL-c with, for example, PCSK9 inhibitors are currently in development, but not yet licensed. These have resulted in substantial LDL-c lowering (by more than 60–70%) and they are effective in those already treated with statins (PCSK9 is up-regulated in those treated with statins and it blocks the recycling of LDL receptors). Thus, PCSK9 inhibitors have the potential to produce further improvements in outcome in patients with persistent elevations of LDL-c despite statins, and in patients with FH. Results of ongoing clinical endpoint trials will help determine their role in lipid lowering algorithms.
Statins and fibric acid derivatives
Fibrates are peroxisome proliferator activated receptor α (PPAR-α) agonists that lower plasma triglycerides and elevate values of HDL-c. The clinical utility of therapy with fibric acid derivatives (either as monotherapy or as adjunctive therapy with statins) is not supported by two recent clinical trials, FIELD and ACCORD,200 ,201 which both failed to achieve their primary endpoints of reducing CVD events. Meta-analyses of all the fibrate trials show no benefit in terms of all-cause mortality.202 Fibrates may still have a place in the management of rare dyslipidaemias in specialist lipid clinics, and are mainly used when triglyceride values are very high (>10 mmol/L).
Combination therapy for HDL-c elevation
Most attention in clinical practice has appropriately been paid to the lowering of LDL-c. However, despite major outcome benefits from use of statins considerable residual CVD risk remains. As a result, other modifiable lipid sub-fractions such as HDL-c have become important targets for treatment.
In observational studies, a low HDL-c value is a well established CVD risk factor and HDL-c values have an inverse relation to risk, even in subjects with low LDL-c. Furthermore, this remains after treatment, and after high dose statins. A high HDL-c value, however, has not been shown to protect against CVD and recent genetic studies have cast doubt on the causal role of HDL-c in CVD.
The Aim High trial, which evaluated the safety and efficacy of niacin, was stopped prematurely, and the recent HPS2 Thrive study also failed to show benefit. CETP (cholesterylester transfer protein) inhibitors produce significant elevation of HDL-c (together with LDL-c lowering with some agents). However, torcetrapib, the first in the class, was withdrawn due to excess mortality from off-target drug effects, and the subsequent dalcetrapib programme was abandoned on the grounds of futility, after the Dal Outcomes trial. Recent work has suggested that the properties of HDL-c may be substantially altered in inflammatory conditions, renal disease, and CVD and that its function rather than merely the plasma level may have an important influence on its clinical effects. A recent meta-analysis showed that baseline HDL-c values were strongly related to CVD events in statin treated patients. HDL-c values were strongly associated with reduced CVD events even in those with very low LDL-c values, but an increase in HDL-c was not associated with reduced risk of major CVD events. In contrast, ApoA1 values were predictors both of the risk and of the benefit from treatment. Further evidence from ongoing trials, including CETP inhibition, should clarify the value of HDL-c elevation. The findings for ApoA1 suggest that several new approaches which can modify ApoA1 values may have clinical value. At present, however, measurement of HDL-c to assess CVD risk is justified, but the use of treatments to raise HDL-c is not supported.
2.1.3 Summary
FH
-
Patients with FH are at high risk of premature CVD and need early ‘lifetime’ treatment. Referral to a specialist lipid clinic is recommended.
-
Current treatments which lower LDL-c substantially improve CVD evolution and reduce clinical events.
-
New drugs will likely enable LDL-c values to be lowered substantially more than with statins alone or with combinations of other currently available agents.
-
Detection of FH cases in the population is low and systematic screening is advocated and supported by NICE guidance.
-
Despite this there has been patchy implementation of a systematic diagnosis programme in England despite screening programmes in Scotland, Northern Ireland, and Wales.
-
FH is an excellent example of the potential benefit of early diagnosis and lifetime lowering of CVD risk factors (especially in LDL-c) which results in substantial improvement in CVD outcomes.
Lipids
-
Non-fasting blood samples should be taken to measure TC and HDL-c. The JBS3 risk calculator enables entry of these two measures and it is expected that non-HDL-c (TC minus HDL-c=non-HDL-c) will replace LDL-c in clinical practice as well as in clinical trials.
-
All high risk people should receive professional lifestyle support to reduce total and LDL-c, raise HDL-c, and lower triglycerides and to reduce their cardiovascular risk.
-
Cholesterol lowering drug therapy is recommended in:
-
Patients with established CVD
-
Individuals at particularly high risk of CVD: diabetes >40 years, patients with CKD stages 3–5, or FH
-
Individuals with high 10-year CVD risk (threshold to be defined by NICE guidance)
-
Individuals with high lifetime CVD risk estimated from heart age and other JBS3 calculator metrics, in whom lifestyle changes alone are considered insufficient by the physician and person concerned
-
-
Statins are recommended as they are highly effective at reducing CVD events, with evidence of benefit to LDL-c values <2 mmol/L which justifies intensive non-HDL-c lowering.
-
Statins are safe with trial evidence showing no effects on non-cardiovascular mortality or cancer. There is a small increase in risk of developing diabetes, but the benefits of cholesterol lowering greatly exceed any risk associated with diabetes. If statin intolerance develops a stepwise strategy involving switching agents and re-dosing is recommended.
-
Despite low HDL-c values contributing to CVD risk, drug therapy to raise HDL-c has not been shown to reduce CVD risk and is not currently indicated.
2.2 Blood pressure
Recommendations
-
Hypertension should be suspected when office BP is persistently elevated, ie, ≥140/90 mm Hg.
-
ABPM is recommended to confirm the diagnosis of hypertension (daytime mean ABPM ≥135/85 mm Hg).
-
All high risk people should receive professional lifestyle support to reduce their BP which may avoid the need for, or complement the use of, drug therapy for hypertension and reduce CVD risk.
-
People with an office BP >160/100 mm Hg, a 24 h day time ABPM average or home ABPM average of >150/95 mm Hg (stage 2 hypertension) should be offered pharmacological therapy to reduce BP.
-
People with an office BP >140/90 mm Hg, but <160/100 mm Hg, a 24 h daytime ABPM average or home ABPM average of >135/85 mm Hg (stage 1 hypertension) and established CVD, hypertensive target organ damage, diabetes, CKD, or a high lifetime risk assessed by JBS3 calculator, should be offered pharmacological therapy to reduce BP.
-
People with stage 1 hypertension without established CVD, hypertensive target organ damage, diabetes, CKD, or a significant increase in lifetime risk assessed by JBS3 calculator, should receive advice on lifestyle interventions and be scheduled for annual BP and lifetime risk assessment to inform future need for therapy.
-
Pharmacological treatment for patients with hypertension should follow the current NICE guidance (CG127) treatment algorithm:
-
Patients <55 years of age should be offered an ACE inhibitor or ARB as preferred initial therapy
-
Patients aged ≥55 years should be offered a CCB as preferred initial therapy
-
-
Combinations of drug treatment are usually required to optimise BP control for the majority of patients.
-
Thiazide-like diuretics are an alternative to CCBs and are preferred for patients intolerant of CCBs, or with heart failure or at high risk of heart failure.
-
β-blockers are not preferred unless there are specific indications for use, ie, in patients with symptomatic angina or chronic heart failure.
-
The recommendations of the NICE guideline CG107 Hypertension in pregnancy should be followed for pregnant women or women planning pregnancy.
2.2.1 Background
Routine BP measurement is now commonplace in the UK. The screening, diagnosis, treatment, and follow-up of patients with elevated BP accounts for approximately 12% of all primary care consulting episodes and £1 billion in annual drug costs alone.203 Once BP is elevated to ≥140/90 mm Hg, it is classified as hypertension, which is present in ≥25% of British adults and >50% over the age of 60 years. BP increases with age and as BP increases, so does the risk of stroke, CHD and heart failure, such that the risk of CVD events doubles for every 20/10 mm Hg rise in BP from a baseline of 115/70 mm Hg.37 Elevated BP is also associated with an accelerated rate of decline of cognitive function and renal function.204 ,205 BP is normally distributed in the population, and epidemiological studies demonstrate that the CVD risk associated with increasing BP is log-linear—there is no obvious cut-point above or below which risk starts or ends.37 Hence the definition of hypertension is arbitrary. The results of clinical trials have determined a pragmatic definition of hypertension: “the level of BP at which there is evidence that BP lowering does more good (in terms of reducing CVD risk) than harm”.
Although BP is an independent risk factor for CVD, that risk is importantly modified by the presence of established target organ damage or manifest CVD, and/or other risk factors for CVD.206 Therefore, total CVD risk management, beyond BP lowering alone, is essential in hypertensive patients in order to maximise risk reduction. The absolute risk reduction will be greatest in those at highest risk. Data from many RCTs provide compelling evidence of the effectiveness of antihypertensive therapy at reducing the risk of CVD, across the age range of 40–90 years.203 ,207 A treatment induced reduction in BP by an average of 10/5 mm Hg can be expected to reduce stroke by 40% and CHD by 20%.37 Cognitive impairment associated with increasing age has also been reduced by BP treatment in some, but not all, trials.208 ,209 Among patients <40 years, no trial data are available to guide practice, but recent epidemiological evidence demonstrates a clear rise in longer term risk of CVD mortality from the age of 18 years, emphasising the importance of ‘lifetime’ exposure to high BP.210
Finally, there has been an increased focus recently on defining better the BP phenotype beyond conventional clinic BP measurement, with emphasis on wider use of home or ambulatory BP measurement to improve the specificity of diagnosis of hypertension and to monitor BP control.203 Further recent evidence has also suggested that long term (visit-to-visit) BP variability (BPV) maybe a stronger predictor of CVD events (particularly stroke) than mean clinic BP levels, and that this BPV may be differentially influenced by the BP treatment strategy.211 ,212
2.2.2 Diagnosis of hypertension
In the UK, adults from 40 years onwards should have their BP measured as part of an opportunistic CVD risk assessment at least once every 5 years as part of the NHS Health Check programme.213 BP measurements should be made under standardised conditions using accurate, validated and well maintained monitors with an appropriate cuff size.203
Hypertension, based on clinical BP readings, should be suspected in adults (aged ≥18 years) when the clinic systolic BP is ≥140 mm Hg and/or the diastolic BP is ≥90 mm Hg when measured on more than one occasion, while seated under standardised conditions.203
The most recent NICE hypertension guideline recommends the routine use of ABPM to confirm the diagnosis of hypertension in people who have elevated chronic seated BP levels.203 Thus, when hypertension is suspected based on seated clinic readings, ABPM should be offered to confirm the diagnosis with at least 14 daytime BP readings. A mean daytime ABPM average of ≥135 mm Hg systolic BP and/or diastolic BP ≥85 mm Hg is being used to define hypertension. This recommendation was based on data from systematic reviews which showed ABPM to be: (1) a stronger predictor of clinical outcomes than conventional clinic BP readings; (2) more specific at defining hypertension, eliminating approximately 25% of patients with so-called ‘white coat hypertension’ who would otherwise have been erroneously labelled as hypertensive based on clinic BP alone; and (3) a very cost effective strategy for the diagnosis of hypertension and potentially cost saving after 5 years.
Home BP monitoring (HBPM) is an alternative to ABPM where the latter is not available or declined by the patient. When using HBPM, BP should be measured seated, under standardised conditions, twice at each sitting, on two occasions each day, for a minimum of 4 days and ideally for 7 days, with the readings on the first day excluded from the average of all subsequent readings. The BP threshold for diagnosing hypertension according to the HBPM average is the same as that for the ABPM daytime BP average —that is, ≥135 mm Hg systolic BP and/or diastolic BP ≥85 mm Hg. It is important to note that ABPM and HBPM readings, using automated BP devices, can be unreliable in patients with significant pulse irregularity, for example, AF, and in such patients conventional clinic based sphygmomanometry and auscultation is the only reliable method of measuring BP.
While recognising the continuous nature of BP levels, two grades of hypertension are defined, stage 1 and stage 2, as crude measures of severity, with potential implications for the urgency of initiating therapy. The corresponding clinic and ABPM/HBPM values are shown in table 2.
Blood pressure staging and diagnostic thresholds for hypertension according to clinic, ABPM and HBPM
Routine investigations for people with hypertension
People with hypertension should undergo a series of routine investigations to assess their CVD risk and target organ damage, to assist in their risk profiling and in making the decision to treat (box 3).
Routine investigations for patients with hypertension
-
Urine dipstick for protein and blood
-
Urine albumin:creatinine ratio
-
Renal function (eGFR)/electrolytes
-
Blood glucose (fasted)/glycated HbA1c
-
Lipid profile
-
ECG
-
Fundoscopy for retinopathy
eGFR, estimated glomerular filtration rate.
2.2.3 Treatment approaches
BP thresholds for treatment
People with a persistently high-normal clinic BP (135–139/85–89 mm Hg) have a high rate of progression to overt hypertension214 and should receive ‘lifestyle advice’ to help reduce their BP and CVD risk, using the JBS3 calculator.03
Recommended lifestyle changes to reduce BP and CVD risk are shown in box 4. Lifestyle modification can also reduce BP and obviate the need for drug therapy in people with stage 1 hypertension, or reduce the number of drugs required to control BP in people with drug-treated hypertension.203 ,215 (For more detailed discussion or lifestyle interventions to reduce CVD see Lifestyle section.)
Lifestyle recommendations
-
Lifestyle measures that lower blood pressure
-
Weight reduction
-
Reduced salt intake
-
Limitation of alcohol consumption
-
Increased physical activity
-
Increased fruit and vegetable consumption
-
Reduced total fat and saturated fat intake
-
-
Measures to reduce cardiovascular disease risk
-
Cessation of smoking
-
Reduced total fat and saturated fat intake
-
Replacement of saturated fats with monounsaturated fats
-
Increased oily fish consumption
-
BP thresholds for intervention with drug therapy are outlined in table 3. People with stage 2 hypertension, including the very elderly (ie, aged ≥80 years), are at sufficiently high CVD risk on the basis of BP levels alone to require drug therapy to reduce their BP. The decision to treat people with stage 1 hypertension will depend on three factors: (1) the presence of clinical evidence of CVD or diabetes; (2) the presence of target organ damage (box 3); and/or (3) their estimated CVD risk using the JSB3 risk calculator. People with stage 1 hypertension and clinical evidence of CVD or diabetes or target organ damage or a 10-year CVD risk estimated to be ≥20%, or a high modifiable lifetime CVD risk, should be offered BP lowering drug therapy.203 People with stage 1 hypertension, but without CVD, diabetes or target organ damage, should have lifetime risk assessment on an individual basis to inform lifestyle strategies. They should have their BP and lifetime CVD risk reassessed annually, and be considered for BP lowering drug therapy based on the benefits of lifetime risk reduction for the individual.
Blood pressure treatment targets
BP treatment targets
The benefits of BP reduction are primarily driven by the quality of BP reduction.216 Systolic BP is generally more difficult to control than diastolic BP.217 Recommended treatment targets are shown in table 3. Although ABPM has been recommended to confirm the diagnosis of hypertension, there is insufficient evidence at present to use anything other than clinic BP to monitor the BP control of treated hypertension.203 Thus, seated clinic BP is recommended to monitor BP control. However, for patients noted to have a pronounced discrepancy between their clinic BP levels and those from ABPM or HBPM at the time of diagnosis, it may be necessary to use ABPM or HBPM to monitor their BP control.
The limited data available suggest that BP should be treated to a seated clinic systolic BP target of <140 mm Hg, aiming for a systolic BP of 130–135 mm Hg. The recommended diastolic BP treatment target is <90 mm Hg, aiming for a diastolic BP of 80–85 mm Hg. These treatment targets apply to all patients except those initiating treatment at the age of ≥80 years, in whom the BP target should be <150/90 mm Hg.203 If ABPM or HBPM monitoring is used to monitor BP control, the BP target would be <135/85 mm Hg, or <150/85 mm Hg in those aged ≥80 years.
Previous guidelines recommended lower clinic BP targets (ie, <130/80 mm Hg) for people with established CVD, diabetes or CKD. However, there are no reliable prospective clinical trial data to support such a recommendation. Furthermore, some post-hoc, retrospective data suggest that, among some subgroups of patients, a J-shaped relationship between systolic BP achieved and CVD risk may pertain.218 ,219 Hence, pending good prospective trial evidence, this lower BP target can no longer be recommended for all high risk patients. However, such treatment targets may still be appropriate in younger high risk patients, but this has not been confirmed in clinical trials. See sections for specific recommendations in diabetes and CKD.
Selection of drug therapy
Randomised controlled clinical trials have consistently demonstrated that BP lowering, based on various classes of drug therapy, is effective at reducing CVD, cerebrovascular and renal morbidity and mortality.207 ,216 Meta-analyses and overviews of treatment of hypertension have concluded that the main driver of benefit from antihypertensive therapy is BP lowering per se.205 ,207 ,216 Furthermore, most hypertensive patients require more than one drug to achieve BP control.220 Thus, the emphasis of treatment is on defining an optimal treatment strategy rather than an optimal drug therapy. The most cost effective drug treatments for hypertension are ACE inhibition or ARBs (A), CCBs (C), or the thiazide-like diuretics (D).203 β-blockers are significantly less cost effective, largely because of less effective stroke and CHD prevention than the aforementioned treatments. ‘No treatment’ is the least cost effective option of all.203 Thus, a trio of treatments A, C, and D should form the basis of the treatment strategy for most people with hypertension.
In clinical trials of BP lowering drugs, most people have required at least two BP lowering drugs to achieve recommended BP targets. In clinical practice in England, the majority (54%) of treated patients receive more than two drugs. Despite this, fewer than two thirds (63%) of treated hypertensive people in England have their BP optimally controlled. A key message is that monotherapy (currently used by 45% of treated patients in England) is usually insufficient therapy for hypertension.
Recommended drug treatment algorithm
NICE, in its most recent hypertension guideline in collaboration with the British Hypertension Society (BHS), recommended a simple treatment algorithm based on the aforementioned trio of treatments (A, C, D) (figure 30), to assist practitioners in logical sequencing and combinations of drug therapy.203

Hypertension treatment algorithm. ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker.
The recommended drug combinations and sequencing are similar to those used in many contemporary clinical trials of BP lowering drugs.207 ,216 People who are younger (ie, aged <55 years) are recommended to initiate therapy with an A drug (ie, an ACE inhibitor or ARB). This recommendation reflects the fact that younger people generally have a more active renin–angiotensin system, and thus an A drug is likely to be the most effective initial BP lowering therapy. The caveat to this recommendation relates to women of childbearing potential. ACE inhibitors or ARBs should be avoided in pregnancy. In women planning pregnancy or at risk of pregnancy, a β-blocker or methyldopa may be suitable alternatives.221 People aged ≥55 years should receive a CCB as initial therapy. In such patients, a thiazide-type diuretic (ie, chlorthalidone or indapamide) is a possible alternative in those with peripheral oedema, heart failure or at risk of heart failure, such as the very elderly or those intolerant of CCB. For thiazide-type diuretic therapy, low dose therapy with chlorthalidone (12.5–25 mg) or indapamide (2.5 mg or 1.5 mg SR (slow release)) is preferred to low dose conventional thiazide diuretic, for example, bendroflumethiazide or hydrochlorothiazide, as there is no evidence of benefit on CVD outcomes with the latter class of agents.203 A CCB (or thiazide-type diuretic) is also recommended as initial therapy for people of black African/Caribbean origin at any age.
Monotherapy is insufficient to control BP in most patients, and at step 2 a combination of A+C is recommended.220 This is the preferred two-drug combination, unless a thiazide-type diuretic has been indicated. For those in whom BP is still not controlled, step 3 treatment is indicated, that is, A+C+D.203 This treatment strategy should be sufficient to control BP in the majority of patients. Combination therapy can be prescribed as free combinations of drugs or as single pill combinations (hitherto frequently and inaccurately described as fixed dose combinations). Systematic reviews have suggested that single pill combination therapy may improve adherence to treatment,222 BP control,223 and to be cost effective.224 The use of single pill combinations should be preferred, unless a clear cost disadvantage to their use is apparent.
β-blockers are not recommended as part of the treatment algorithm because they are no more effective at preventing CVD events than the recommended alternatives and are less effective at preventing stroke.203 ,225 ,226 However, β-blockers should be considered for patients with others indications for their use, for example, patients with symptomatic angina, heart failure, or post-MI, or in women anticipating or at risk of pregnancy.
Recent trials have also demonstrated that combining ACE inhibitors and ARBs for the treatment of hypertension provides no additional CVD protection, and renal outcomes are worsened when compared with either agent used as monotherapy227; hence, this combination should not be used. Prescribing information for all BP medications should be considered before use.
Resistant hypertension
Resistant hypertension is defined as a BP that is not controlled (clinic BP >140/90 mm Hg) as confirmed by ABPM (daytime average BP >135/85 mm Hg), despite treatment with optimal or best tolerated doses of at least three medications (ideally A+C+D), having excluded treatable causes of secondary hypertension.203 ,228 The true prevalence of resistant hypertension is not known, but is likely to be <10% of patients. This is supported by data from the Health Survey for England, which showed 8% of patients with uncontrolled BP despite prescribed treatment with at least three BP lowering medications. True prevalence estimates for resistant hypertension are confounded by apparent treatment resistance being commonly as a result of poor adherence to treatment.228 ,229 ,230 There have been no formal clinical trials to define the optimal treatment strategy for resistant hypertension. Observational data suggest that further diuretic therapy, most commonly with low dose spironolactone (eg, 25 mg once daily), can be very effective,203 ,231 but renal function and potassium values must be monitored within a month of initiating therapy, and spironolactone should be avoided in people with significant renal impairment (stage III kidney disease) and/or a baseline potassium ≥4.5 mmol/L.203 Even at these low doses (12.5–25 mg once daily), a small proportion (∼6%) are unable to tolerate spironolactone due to gynaecomastia, and in such patients treatment with eplerenone or amiloride can be offered instead. Other treatments, such as α-blockers (based on observational data)232 or β-blockers can also be considered for the treatment of resistant hypertension.203 Patients with resistant hypertension should be referred to a BP specialist.
Renal denervation has emerged as a potential treatment strategy for true resistant hypertension.233 ,234 Data on the safety and efficacy of this technique suggest that the initial findings relating to efficacy may have been exaggerated.
Indications for specialist referral
Most patients with hypertension can be managed in primary care. Some patients, however, should be considered for specialist referral to evaluate further potential secondary causes of hypertension and for advice on the management of treatment resistance or complex cases of hypertension (box 5).
Indications for specialist referral for patients with hypertension
Urgent treatment needed
-
Accelerated hypertension (severe hypertension and grade III–IV retinopathy)
-
Particularly severe hypertension (>220/120 mm Hg)
-
Impending complications, eg, transient ischaemic attack, left ventricular failure
Possible underlying cause
-
Any clue in history or examination of a secondary cause, such as hypokalaemia with increased or high normal plasma sodium (Conn's syndrome)
-
Elevated serum creatinine
-
Proteinuria or haematuria
-
Sudden onset or worsening of hypertension
-
Resistant to multidrug regimen (≥3 drugs)
-
Young age (any hypertension <20 years; needing treatment <30 years)
Therapeutic problems
-
Multiple drug intolerance
-
Multiple drug contraindications
-
Persistent non-adherence or non-compliance
Going beyond BP to reduce CVD risk in hypertensive patients
Patients who present with hypertension should have their CVD risk assessed using the JBS3 risk calculator. Their lifestyle and drug treatment should be guided by their CVD risk, and treatments to reduce other CV risk factors may be beneficial. The Anglo-Scandinavian Cardiac Outcomes (ASCOT) trial demonstrated that statin therapy greatly reduced the risk of CHD and stroke in patients in whom average BP was controlled to the currently recommended BP target, irrespective of the baseline cholesterol value.235 Furthermore, antiplatelet therapy should also be considered in patients with established ischaemic heart disease or prior ischaemic stroke or TIA.
2.2.4 Summary
-
Hypertension should be suspected when office BP is persistently elevated, ie, ≥140/90 mm Hg.
-
ABPM is recommended to confirm the diagnosis of hypertension (daytime mean ABPM ≥135/85 mm Hg).
-
All high risk people should receive professional lifestyle support to reduce their BP which may avoid the need for, or complement the use of, drug therapy for hypertension and reduce CVD risk.
-
People with an office BP >160/100 mm Hg, a 24 h daytime ABPM average or home ABPM average of >150/95 mm Hg (stage 2 hypertension) should be offered pharmacological therapy to reduce BP.
-
People with an office BP >140/90 mm Hg, but <160/100 mm Hg, a 24 h daytime ABPM average or home ABPM average of >135/85 mm Hg (stage 1 hypertension) and established CVD, hypertensive target organ damage, diabetes, CKD, or a high lifetime risk assessed by JBS3 calculator, should be offered pharmacological therapy to reduce BP.
-
Pharmacological treatment for patients with hypertension should follow the current NICE guidance (CG127) treatment algorithm:
-
Combinations of drug treatment are usually required to optimise BP control for the majority of patients.
-
For pregnant women or women planning pregnancy, when BP treatment is being considered, the recommendations of the NICE guideline CG107 Hypertension in pregnancy should be followed.
-
2.3 Established cardiovascular disease and differences in post-myocardial infarction and stroke management
Recommendations
General recommendations
-
For all patients with established CVD, an intensive approach to risk factor modification is recommended, including lifestyle intervention and the use of pharmacological therapy for secondary prevention based on NICE, SIGN, and ESC guidance.
-
Statins should be prescribed with a ‘lower is better’ approach, to achieve values of at least <2.5 mmol/L for non-HDL-c (equivalent to <1.8 mmol/L for LDL-c).
Post-MI
Antiplatelet therapy
-
Antiplatelet therapy with low dose aspirin (75–100 mg) is recommended indefinitely after MI.
-
In patients with true aspirin intolerance, clopidogrel 75 mg should be considered as an alternative.
-
More potent antiplatelet agents (such as prasugrel or ticagrelor) are recommended as dual antiplatelet therapy, in combination with aspirin, in patients with acute coronary syndromes.
-
Dual antiplatelet therapy is recommended for up to 12 months post-MI with a minimum of:
-
1 month for patients also receiving a bare metal stent
-
6 months for patients also receiving a drug eluting stent
Lipid lowering therapy
-
-
Intensive statin therapy is recommended in all patients following MI in the absence of a contraindication or intolerance, irrespective of initial cholesterol values.
-
Statins should be prescribed with a ‘lower is better’ approach to achieve values of at least <2.5 mmol, for non-HDL-c (equivalent to <1.8 mmol/L for LDL-c).
β-blockers, ACE inhibitors/ARBs, aldosterone antagonists
-
Use of β-blockers, ACE inhibitors/ARBs and aldosterone antagonists post-MI is recommended, in line with existing NICE, SIGN, and ESC guidance.
Post-stroke
BP lowering
-
Optimal BP levels on treatment for patients with established cerebrovascular disease are unclear, but levels of <130/80 mm Hg are recommended. Care should be taken not to reduce BP rapidly in those with significant carotid/vertebrobasilar stenosis. Treatment should usually be started within 1–2 weeks of the acute event.
Lipid lowering
-
Statin therapy is recommended for patients with ischaemic stroke. Its introduction should be delayed for 2 weeks post-stroke, but there is no need to discontinue statins in patients already on therapy
-
Statin therapy should be avoided in individuals with a history of haemorrhagic stroke, particularly in those with inadequately controlled hypertension, unless there is a compelling indication, such as concomitant coronary artery disease.
Antithrombotic therapy
In the absence of AF, recommendations for patients who have had an ischaemic stroke follow the current NICE guidelines2:
-
After acute ischaemic stroke, patients should initially receive 300 mg of aspirin daily for 2 weeks, then be changed to long term clopidogrel 75 mg daily. For patients who have a contraindication or intolerance to clopidogrel, modified release dipyridamole plus aspirin is an alternative. For people who have a contraindication or intolerance to both clopidogrel and aspirin, modified release dipyridamole alone is recommended.
-
For patients with TIAs, modified release dipyridamole 200 mg twice daily plus aspirin 75–150 mg daily is an alternative treatment option to clopidogrel. For people who have a contraindication or intolerance to aspirin, modified release dipyridamole alone is an alternative treatment option.
In the presence of AF (valvular or non-valvular), patients with a TIA or ischaemic stroke:
-
Should be anticoagulated with warfarin to achieve a target INR on warfarin of 2.5 (range 2.0–3.0) or with one of the new oral anticoagulant agents.
-
Anticoagulation should not be started until brain imaging has excluded haemorrhage, and not usually until 14 days have passed from the onset of a disabling ischaemic stroke.
-
Anticoagulation should not be used for patients in sinus rhythm, unless a cardiac source of embolism has been identified.
2.3.1 Established CVD
Background
Individuals with prior MI, stroke or AF have already manifest complications of established CVD and guidelines are consistent in prioritising lifestyle interventions and therapeutic prevention strategies. The risks of recurrence and of major complications are sufficiently high to justify secondary prevention treatment in all, except for those with isolated AF and no additional risk factors (CHADS2VASc score=0).
Although these different CVD conditions share several pathogenic features, there are key differences in the contribution of CVD to their progression and to subsequent complications (figure 31). Thus, they share many secondary prevention strategies, but there are also differences that relate to CV organ specific mechanisms and comorbidity.

{kind=link}
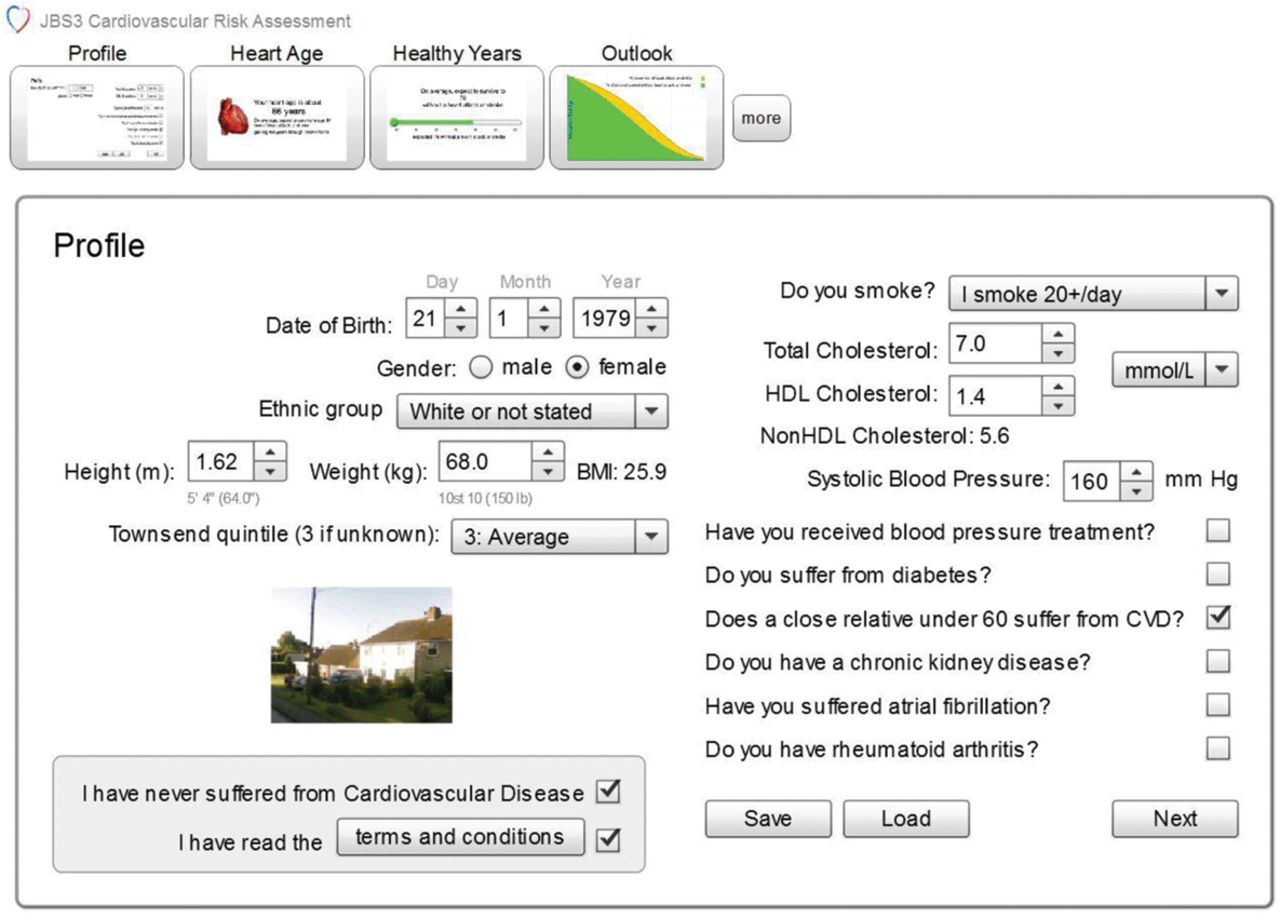{kind=link}
{kind=link}
{kind=link}
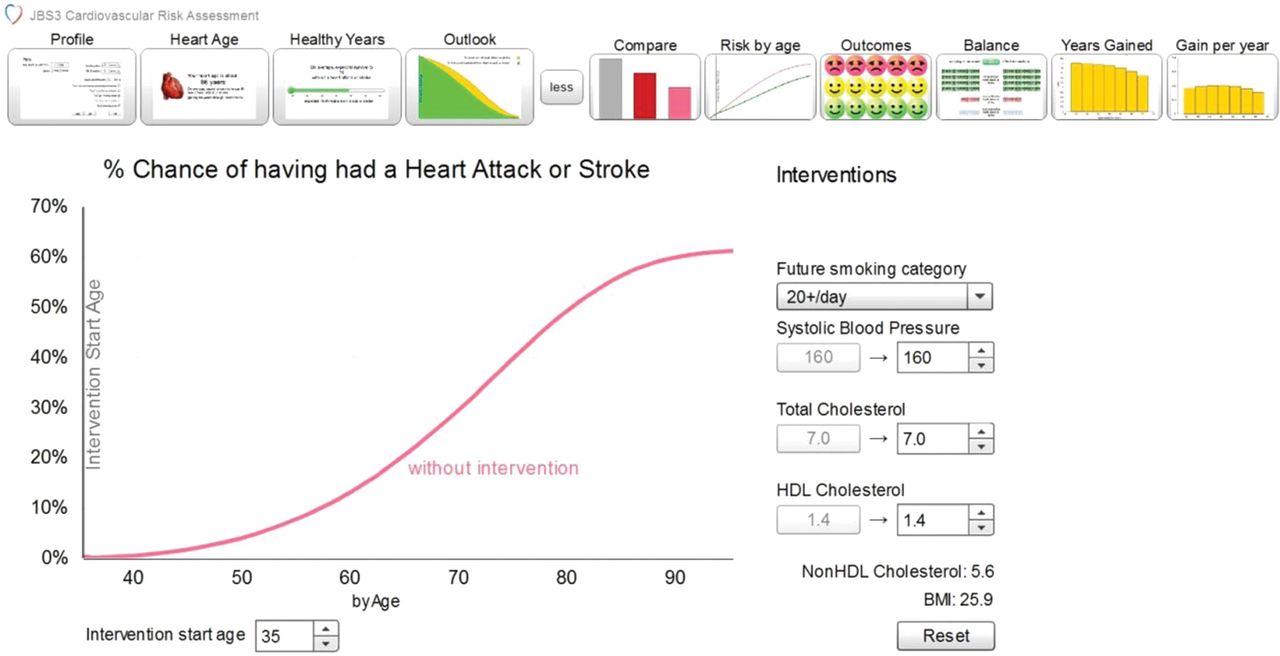{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
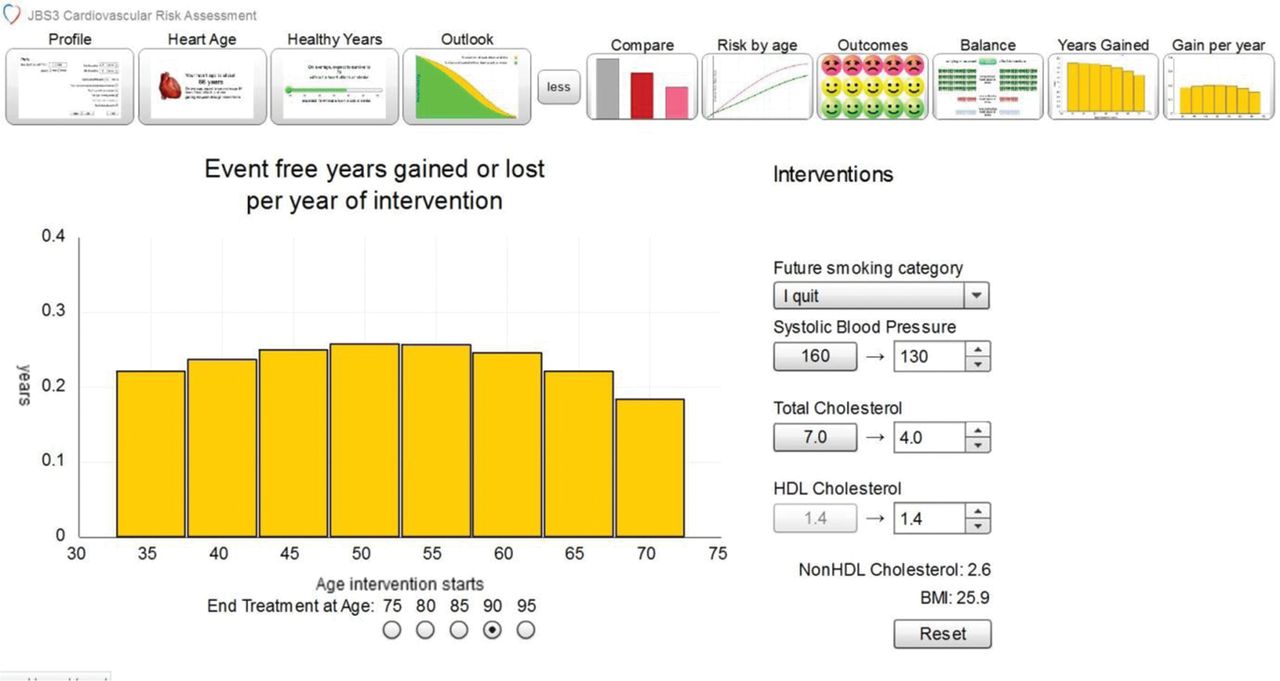{kind=link}
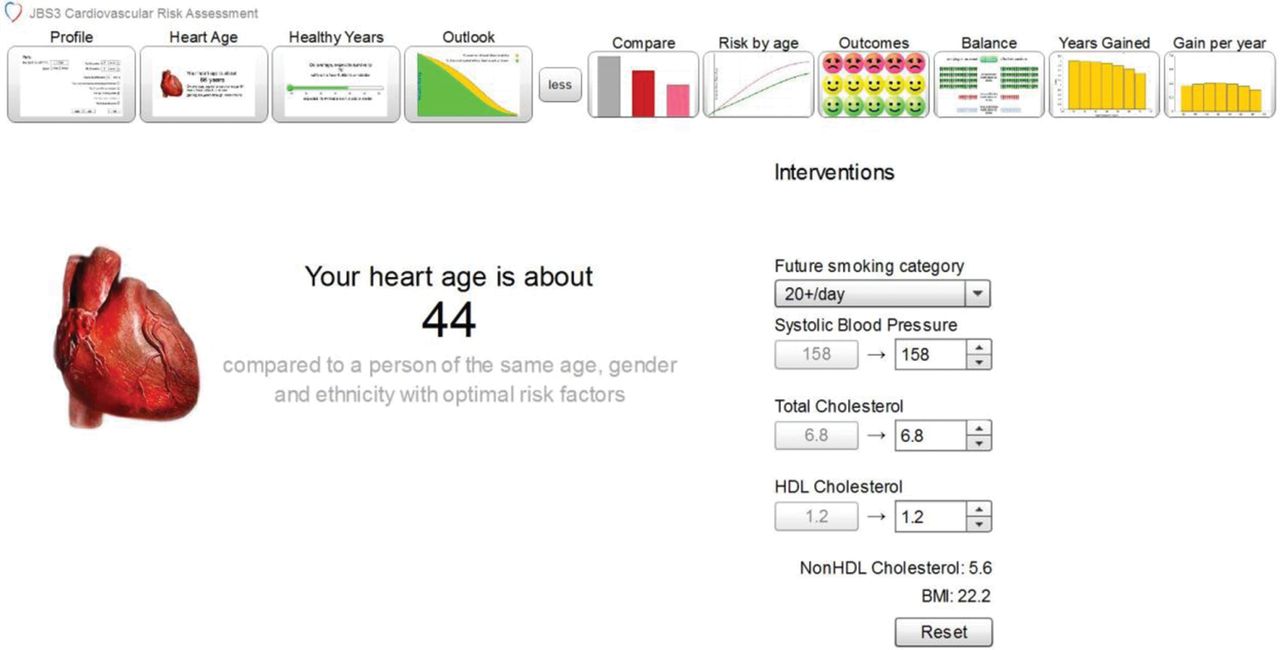{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
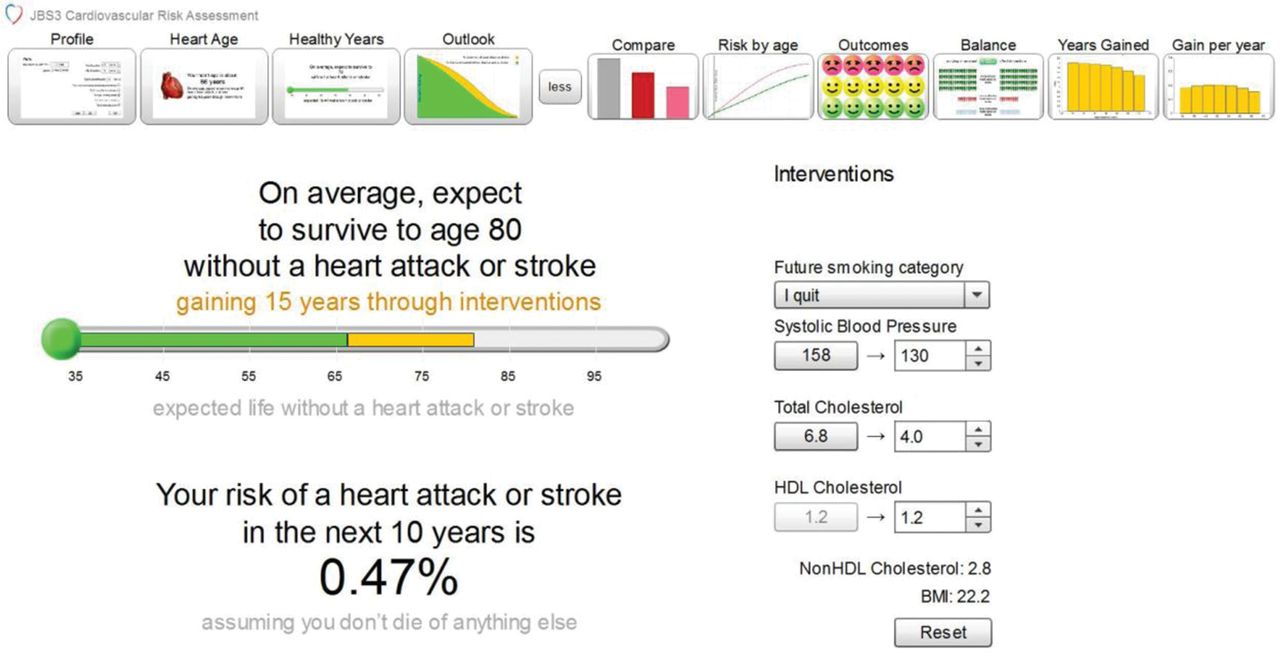{kind=link}
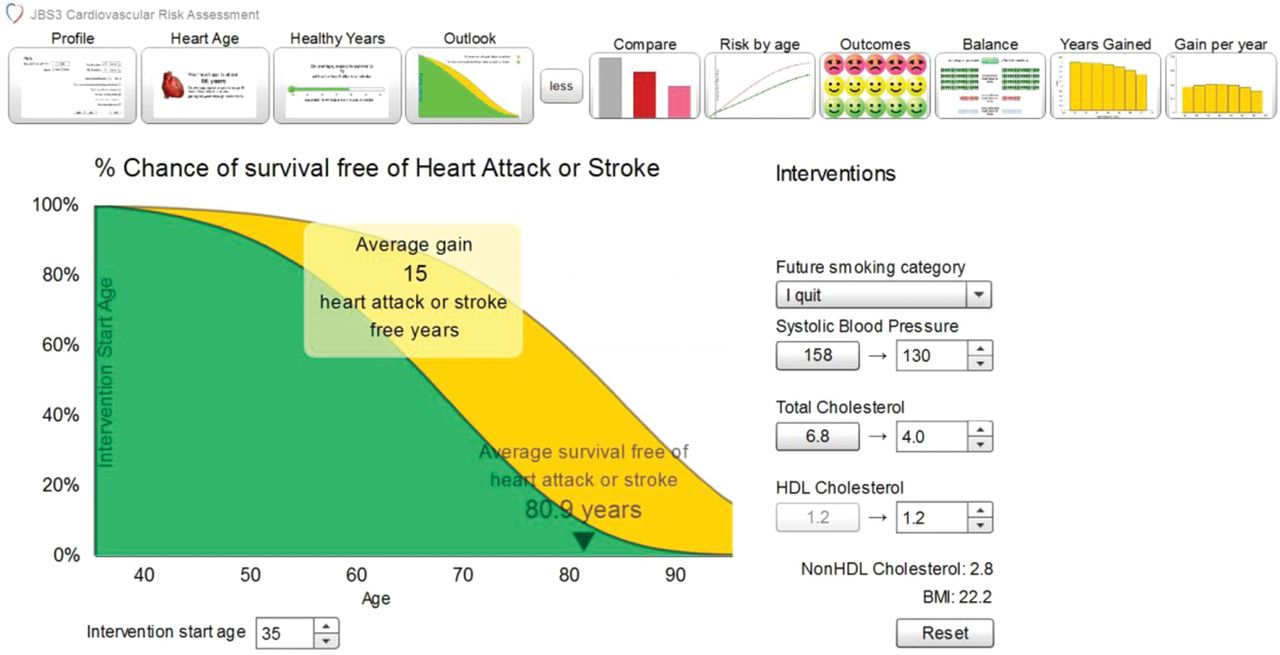{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic representation of the contributions of cardiovascular disease to disease conditions manifest in different organ systems.
Treatment approaches to patients with established CVD
NICE, SIGN, and ESC guidelines are consistent in their major secondary prevention recommendations.236–242
For all patients with established CVD, an intensive approach to risk factor modification is recommended, including lifestyle intervention and the use of pharmacological therapy for secondary prevention. As indicated previously, there are particular considerations for patients with other comorbidities, such as diabetes and CKD.
Nevertheless, the EUROASPIRE III survey reveals major shortfalls in achieving targets: for example, only 48% of those with established CVD achieved smoking cessation, only 34% had regular physical activity, and only 18% had a BMI <25 kg/m2. Only 50% achieved BP levels of <140/90 mm Hg and only 55% achieved an LDL-c of <2.5 mmol/L.14
2.3.2 Post-MI
Risks of future complications are influenced by the extent of left ventricular dysfunction and the extent of coronary artery disease. Following the acute phase of MI, assessment of left ventricular function using echocardiography is recommended with MRI as an alternative approach. For patients with multivessel disease, or in whom revascularisation of other vessels is being considered, stress imaging or imaging for ischaemia and viability is indicated.240 ,243
Initiation of evidence based therapies is recommended before hospital discharge for MI, in order to increase the proportion of patients started and then maintained on secondary prevention therapies. It must be emphasised that the medications are in addition to lifestyle interventions and not alternatives. The input of the cardiologist, GP, rehabilitation specialist, pharmacist, and dietician is required to optimise prevention strategies.
Lipid lowering therapy
Evidence for the benefits of statins in secondary prevention is robust and specific trials have shown early benefit and superiority of more intensive statin therapy.244 ,245 This is manifest by reductions in risk of CVD death, non-fatal MI, ischaemic stroke, and revascularisation. The proportional reductions are independent of the initial LDL-c concentration and hence treatment should be started early during admission, in all patients, with a treatment goal of at least LDL-c <1.8 mmol/L equivalent to non-HDL-c of <2.5 mmol/L. For those with true intolerance to statins, alternative agents including ezetimibe should be considered. Newer approaches to lower LDL-c, for example, PCSK9 inhibitors, are in development (see Lipid section).
There is evidence that low concentrations of HDL-c are associated with increased CVD events (mainly from epidemiological studies).14 Although in some studies, pharmacological approaches to raise HDL-c have shown evidence of improvement in intermediate endpoints, trials have not yet demonstrated improvements in rates of CVD death or MI.
Antithrombotic therapy
Life long aspirin treatment is recommended based upon a meta-analysis of all of the trials in secondary prevention after MI.14 ,236–243 For long term treatment, lower doses of aspirin are generally used to minimise bleeding complications (70–100 mg). Patients with true intolerance of aspirin (rare) should receive clopidogrel (75 mg/day) as long term secondary prevention.245
Novel approaches to platelet inhibition, involving antagonism of the platelet thrombin receptor, for example, with vorapaxar, have not shown sufficient evidence of a favourable risk–benefit balance to be included in guideline recommendations.246 ,247 In all of the studies of more potent antiplatelet and antithrombotic therapy, there is evidence of a trade-off between efficacy and safety. Identification of suitable patients is critical and patients need to be selected on the basis of the potential for benefit with least increase in bleeding risk (using clinical risk scores for outcome and for bleeding risk). Some patients exhibit reduced inhibition of platelet aggregation with aspirin or with thienopyridines (especially clopidogrel), and it was hoped that in vitro assays of platelet aggregation might identify those with the potential for greater benefit from more potent antiplatelet therapy. Although patients with persistently upregulated platelet aggregation have more adverse CVD outcomes, trials of dose escalation and of more potent antiplatelet agents have not resulted in significantly improved outcomes, but have shown an increase in bleeding hazards.
Dual antiplatelet therapy
In the CURE trial, dual antiplatelet therapy with clopidogrel and aspirin was superior to aspirin alone in preventing a composite of outcome events.248 More potent platelet inhibitors (prasugrel or ticagrelor) have each been shown to be superior to clopidogrel in large scale trials in which the therapies were initiated in the acute phase and continued for approximately 12 months, and hence they are recommended in the guidelines.14 ,240–243 There is no evidence to support dual antiplatelet therapy beyond 12 months and studies of aspirin plus clopidogrel in patients with CVD disease have not, overall, shown evidence of significant benefit.248 Nevertheless, further trials with novel agents are underway. Some test the novel agent without aspirin, with the aim of minimising bleeding risk.
In the ATLAS-ACS TIMI 51 study, the addition of a low dose of anticoagulation with rivaroxaban was tested on top of antiplatelet therapy, predominantly aspirin plus clopidogrel.249 The optimal balance of benefit versus risk was achieved with the lowest dose of 2.5 mg twice daily rivaroxaban (a quarter of the dose used in AF) and this therapy is approved by the European Medicines Agency. This combination provides an alternative treatment option without increased risks of bleeding. It remains unclear whether this combined therapy is better or worse than aspirin plus a newer antiplatelet agent (ticagrelor or prasugrel).
Stent implantation
Dual antiplatelet therapy is also required to reduce the risk of stent thrombosis and reinfarction. In trials, a thienopyridine plus aspirin was better than aspirin alone, and both prasugrel and ticagrelor have shown a reduced frequency of stent thrombosis compared with clopidogrel treatment (each on top of aspirin). As a consequence, patients who receive a bare metal stent should be prescribed dual antiplatelet therapy for a minimum of 1 month, versus a minimum of 6 months for those who receive a drug eluting stent.14 ,240 ,241 ,243–245 Robust evidence for benefit compared to risk does not extend beyond 1 year of treatment. Thus, when considering the duration of treatment and, each patient should be assessed in relation to their underlying thrombotic and bleeding risks. Abrupt discontinuations, especially unplanned discontinuations, of dual antiplatelet therapy have been associated with increased risks and particular efforts are required to educate the patients and physicians to manage minor bleeding events without discontinuation of antiplatelet treatments, if possible.250
β-blockers, ACE inhibitors, ARBs
Evidence supports the use of β-blockers after STEMI (for up to 1 year) but is not available beyond this or in other patient groups. β-blockers are indicated in the management of stable ambulant patients with heart failure (together with ACE inhibitors, ARBs, and aldosterone antagonists).245
Detailed consideration of each secondary prevention strategy is beyond the scope of this section and the reader is referred to specific national and international guidelines. 236–242
Atrial fibrillation
Both rhythm and anticoagulation management are considered in recent ESC guidelines.251 There is robust evidence that AF remains undetected in many individuals and is untreated or poorly managed in many others. The ESC guidelines recommend opportunistic screening for AF in patients over 65 years of age, by taking the pulse and then performing an ECG, if an irregular pulse is detected. There is a class 1A recommendation for antithrombotic therapy to prevent thromboembolism and stroke in all patients with AF, except in those who are at very low risk (age <65 years and lone AF) or in those with contraindications. In those with very low risk (CHA2DS2 -VASc score of zero), no antithrombotic therapy is recommended. In those with a CHA2DS2-VASc score of ≥2, oral anticoagulation is recommended (class 1A recommendation). The novel anticoagulants show advantage over warfarin and all novel agents reduce the risk of intracranial haemorrhage (dabigatran, rivaroxaban, apixaban, edoxaban). They do not require dose adjustment and do not have the food and drug interactions of warfarin. The ESC guidelines recommend the approved novel agents, where available, over warfarin. For patients who are poorly controlled or unable to manage warfarin, a novel anticoagulant is recommended in the guidelines.
The role of aspirin has been downgraded in the ESC guidelines.251 Recent trials have shown that the risks of bleeding from aspirin can be as high as those of anticoagulation (eg, with a novel agent), and yet the stroke risks are higher with aspirin than with anticoagulation. Bleeding risk should be assessed (eg, HAS-BLED score) in all patients. This may influence the choice of anticoagulant and indicate whether the benefits may outweigh the risks.
AF in stroke patients
Anticoagulation should be considered for TIA or cerebral infarction patients with permanent or paroxysmal AF where underlying cerebral haemorrhage has been excluded.252 Anticoagulation should be delayed for 2 weeks in those with a severe disabling cerebral infarction.
2.3.3 Stroke
Background
Despite the falling stroke incidence and mortality over the last decade,253 in the UK there are approximately 150 000 strokes per annum, nearly 50 000 of which are recurrent events. There are an additional 40 000 TIAs.
Treatment approaches
BP lowering
Hypertension remains the most important treatable risk factor for the prevention of stroke recurrence. Antihypertensive therapy results in significant benefit in secondary stroke prevention, but is of unproven value immediately following cerebral infarction.254 ,255 Trials suggest that, following a cerebral infarct, primary intracerebral haemorrhage (PICH) or TIA, patients with a clinic BP ≥140/90 mm Hg or even lower benefit from antihypertensive therapy.256–258 Although optimal treatment target BP levels are not established, a goal of <130/80 mm Hg is currently recommended. Secondary prevention regimens based on a thiazide-like agent, for example, indapamide258 or thiazide diuretic,259 with the addition of an ACE inhibitor, as necessary, for control, have been shown to be of benefit.257 A recent systematic review of BP reduction after stroke found that treatment decreased stroke recurrence (OR 0.71, 95% CI 0.59 to 0.86) and all CVD events (OR 0.69, 95% CI 0.57 to 0.85).260 Most trials of BP management after stroke have either excluded PICH patients or the numbers of such patients were too small to enable separate analysis. However, where data are available, this group appears to gain a greater risk reduction with treatment than cerebral infarction patients.257 Those eligible for BP lowering therapy following a TIA or stroke should start therapy within 1–2 weeks of the event. Despite the potential benefits from antihypertensive treatment after stroke, many patients remain untreated and/or have poorly controlled BP levels.261
Lipid lowering therapy
Statin therapy is recommended in ischaemic stroke to reduce CVD events. A recent Cochrane systematic review of lipid lowering therapy in those with cerebrovascular disease showed that if the results for all trials of lipid lowering therapy are combined, there is no treatment benefit on stroke recurrence.262 However, trials of statin therapy alone did show a marginal benefit in reducing subsequent cerebrovascular events in those with a previous history of stroke or TIA (OR 0.88, 95% CI 0.77 to 1.00) by reducing subsequent ischaemic stroke (OR 0.78, 95% CI 0.67 to 0.92). There was no evidence that statins, however, reduced all-cause mortality or sudden death (OR 1.00, 95% CI 0.83 to 1.20). The statin based trials in stroke patients did, however, demonstrate a significant decrease in subsequent serious CVD events (OR 0.74, 95% CI 0.67 to 0.82).263–265 There is evidence from some, but not all, studies that statins may increase the risk of haemorrhagic stroke, and they are probably best avoided in patients with cerebral haemorrhage, especially in the acute phase, unless there is a very strong indication for their use in preventing ischaemic events in other vascular territories. It is recommended that statins are started within 1–2 weeks after cerebral infarction. However, for patients already on statins at the time of cerebral infarct, they need not be discontinued.266
Antiplatelet therapy
A recent NICE Technology Appraisal Guidance, which included nearly 49 000 patients with stroke or TIA (the majority being randomised several weeks after the acute event), suggested that there was a further risk reduction for recurrent stroke in patients taking clopidogrel alone (RR 0.75, 95% CI 0.60 to 0.93) or modified release dipyridamole plus aspirin (RR 0.76, 95% CI 0.62 to 0.92) compared to patients randomised to aspirin alone.267 Patients treated with modified release dipyridamole alone were at significantly higher risk of any recurrent stroke than patients treated with either clopidogrel or the combination of modified release dipyridamole and aspirin. The high risk of further cerebrovascular events after a recent TIA or ischaemic stroke means that antiplatelet management in those in sinus rhythm should be initiated as soon as the diagnosis is made, having excluded a PICH. Treatment should start with aspirin and then be changed to clopidogrel 75 mg daily after 1–2 weeks. No clear guidance can be given for those who have a cerebrovascular event while already taking an antiplatelet agent, but dual therapy such as aspirin plus clopidogrel for a limited period (6–8 weeks), should be considered.
Ongoing and unresolved issues
The SPS3 trial in patients with lacunar stroke failed to show that BP treatment to lower levels (systolic BP <130 mm Hg) resulted in improved stroke prevention compared to higher treatment values (systolic BP 130–140 mm Hg). The study, however, was probably underpowered and there is a clear need to define appropriate BP targets after stroke for both cerebral infarct and PICH patients.268 Although lipid lowering with statins following ischaemic stroke is of benefit, optimal lipid levels and the timing of stating treatment after cerebral infarct remain unclear. The best treatment of patients who have a cerebral ischaemic event while on an antiplatelet agent is also unclear. The risks, especially in terms of significant haemorrhage on long term dual antiplatelet therapy (eg, aspirin plus clopidogrel), seem to outweigh any potential benefits. With the current ability to manage more intensively CVD risk factors, it is uncertain whether intensive medical treatment offers advantages compared to current standard therapy in secondary stroke prevention, while remaining cost effective and not increasing the risk of adverse side effects.
2.3.4 Summary
-
Patients with CVD disease share common pathophysiological mechanisms, irrespective of whether the disease presents in a cardiac, cerebral or peripheral vascular territory.
-
Lifestyle modification with reduction in risk factors, BP management, lipid lowering and certain antithrombotic therapies are recommended for those with CVD disease, provided there are no contraindications.
-
In all patients, the benefits versus potential hazards of therapy need to be considered, especially with more potent antiplatelet and antithrombotic therapies.
-
The concept of ‘lower is better’ is supported by evidence for LDL-c reduction. However, the same is not necessarily true for BP management and glycaemic control.
-
The evidence for the new oral anticoagulants in stroke prophylaxis in AF shows equivalent or greater protection than warfarin, with slightly lower risk of haemorrhage. INR monitoring is not required.
-
Novel strategies have the potential for even greater benefits than existing therapies. However, from a population perspective, the biggest gain would be achieved by consistent adherence to establish secondary prevention therapies, including lifestyle management.
2.4 Peripheral arterial disease (PAD)
Recommendations
-
Patients with PAD should have intensive risk factor modification, including intensive statin therapy and BP managed in line with NICE guidelines.
-
Patients with PAD should be screened for diabetes and CKD.
-
Patients with PAD should be encouraged to exercise and supervised exercise programmes should be available for appropriate patients.
-
Patients with PAD should be started on an antiplatelet agent, with clopidogrel being the agent of first choice.
2.4.1 Background
Patients with PAD are at increased risk of coronary and cerebrovascular events, and more than half of patients with PAD have significant coexisting coronary disease.269 Indeed, in the Reduction of Atherothrombosis for Continued Health (REACH) registry, the additional presence of PAD in patients with coronary disease increased the mortality risk by approximately 50%.270 ,271
All patients with suspected PAD should have the diagnosis confirmed with measurement of the ABPI. An ABPI <0.90 is 90% sensitive and 95% specific for PAD. As well as being a diagnostic tool, ABPI is a marker of generalised CVD risk, and a number of cohort studies have reported a graded inverse relationship of decreasing ABPI to CVD events in both men and women.44 ,272 It has also been suggested that asymptomatic individuals with low ABPI may represent a subgroup of higher CVD risk.273 As a result, calls for wider screening to detect PAD in at-risk populations (elderly, diabetics, and those with other CVD risk factors) have been made.274–277 Currently, however, the value of screening asymptomatic individuals using ABPI is unclear.278 ,279
2.4.2 Treatment approaches
The management of PAD can be divided into two strategies, which are not mutually exclusive: reducing the patient's CVD risk; and walking distances. The first approach involves smoking cessation, BP management, diabetes management, lipid lowering therapy, and antiplatelet therapy, whereas the latter focuses on relieving symptoms, improving daily functional activities, and increasing exercise performance. It may involve the use of pharmacological agents, such as naftidrofuryl and cilostazol, or supervised exercise programmes. NICE has recommended naftidrofuryl oxalate as a first line option for the pharmacological treatment of symptoms in intermittent claudication in people with PAD for whom vasodilator therapy is considered appropriate, after taking into account other treatment options.280
Smoking cessation
Smoking is the strongest risk factor for PAD and current smokers are almost four times as likely to develop asymptomatic PAD as non-smokers.281 However, no benefit of cessation on walking distance has been found in four cohort studies.282 Nevertheless, in terms of CVD and respiratory health, it remains an important part of management in PAD patients.283 ,284
Physical activity and exercise
The risk of PAD is inversely related to previous levels of physical activity, suggesting a protective effect of exercise.285 A Cochrane review of 22 studies showed that compared with usual care or placebo, exercise significantly improved maximal walking time and distance with an overall improvement in walking ability of 50%–200%.286 Supervised exercise therapy has the best effects.287
Antiplatelet therapy
Antiplatelet therapy can reduce the risk of fatal and non-fatal CVD events in PAD patients. Evidence from meta-analyses confirms that the long term use of antiplatelet agents reduces the rate of MI and ischaemic stroke in patients with symptomatic PAD.288 ,289 NICE recommends clopidogrel as the agent of choice in PAD, rather than aspirin.267
In the CAPRIE trial of clopidogrel versus aspirin, the benefits of clopidogrel over aspirin were most pronounced in the PAD subgroup (relative risk reduction 23.8%).290 In the CHARISMA trial of clopidogrel and aspirin versus aspirin alone, there was no benefit for dual antiplatelet therapy overall or in the PAD subgroup.291 In patients with intermittent claudication, antiplatelet therapies are associated with lower all-cause and CVD mortality compared with placebo. Compared with all antiplatelet therapies, the strongest evidence exists for thienopyridines, such as clopidogrel.292
Lipid lowering therapy
Statins have a wide range of benefits and all PAD patients should receive them, if tolerated.283 ,284 ,293 A systematic review of lipid lowering therapies in PAD, including 18 trials, found no significant effect on overall mortality or on total CVD events.294 However, a subgroup analysis did show a reduction in coronary events. Pooling of the results from several small trials of a range of lipid lowering agents indicated an improvement in total walking distance and pain-free walking distance but no significant impact on ankle brachial index (ABPI). The conclusion was that lipid lowering therapy is effective in reducing CVD mortality and morbidity in people with PAD, and may also improve local symptoms. A separate systematic review has confirmed the beneficial effect of statins on intermittent claudication (IC) distance.295 Currently, the use of a statin in people with PAD is recommended by most guidelines as an essential part of PAD management.283
Hypertension
Both the HOPE study and more recently the ASCOT trial have reported on subgroups of patients with PAD and have shown that they obtain the same benefit as other groups of patients with CVD, without an increase in adverse event rates.296–298
In a Cochrane review of BP control in PAD, four studies were included.299 The conclusion was that evidence on various antihypertensive drugs in people with PAD is poor, so that it is unknown whether significant benefits or risks accrue from their use. However, lack of data, specifically examining outcomes in PAD patients, should not detract from the compelling evidence of the benefit of treating hypertension and lowering BP available from other sources.
2.4.3 Summary
-
PAD is an atherosclerotic condition with an anticipated risk equivalent to established coronary disease.
-
A strong case exists for intensive modification of CVD risk factors.
-
Management of PAD and CVD risk factors has the potential to improve substantially the outlook for these high risk patients.
2.5 Type 1 and 2 diabetes mellitus
Recommendations
Type 1 diabetes mellitus
Lipid lowering
All people with type 1 diabetes should receive professional lifestyle advice. Statins should be offered in type 1 diabetes for the following categories:
-
All patients with type 1 diabetes aged ≥50 years.
-
The majority aged 40–50 years, unless short duration of diabetes (<5 years) and absence of other CVD risk factors.
-
Those aged 30–40 years with any of the following features: long duration of diabetes (20 years) and poor control (HbA1c >9% (75 mmol/mol)), persistent albuminuria (>30 mg/day) or eGFR <60 mL/min, proliferative retinopathy, treated hypertension, current smoking, autonomic neuropathy, TC (>5 mmol/L) with reduced HDL-c (<1 mmol/L for males and <1.2 mmol/L for females), or central obesity, or with a family history of premature CVD (<50 years).
-
Those aged 18–30 years should receive statins if persistent albuminuria is detected, with caution exercised in women of childbearing potential.
Blood pressure
-
This should be maintained at 130/80 mm Hg, with consideration of lower values (120/75–80 mm Hg) in younger patients with type 1 diabetes (aged <40 years) with persistent microalbuminuria.
-
ACE inhibitors should be the drug of first choice.
Aspirin
-
There is no role for aspirin in primary prevention of CVD in type 1 diabetes.
Glycaemic control
-
Glyceamic control, to achieve and maintain an HbA1c of 48–58 mmol/L, should be considered the ideal approach to long term care of type 1 diabetes.
Type 2 diabetes mellitus
Lipid lowering
All people with type 2 diabetes should receive professional lifestyle advice.
-
Statin therapy remains the best and only effective lipid modifying agent to lessen CVD risk in type 2 diabetes.
-
Statin therapy is recommended for all patients with type 2 diabetes >40 years of age irrespective of cholesterol value.
-
Intensive statin therapy is recommended for diabetes patients with existing CVD, and those with persistent proteinuria or CKD with eGFR 30–60 mL/min. Intensive statin treatment is also recommended for patients who do not achieve non-HDL-c targets.
-
Statins should also considered for patients with type 2 diabetes under 40 years of age, if evidence of persistent albuminuria, eGFR <60 mL/min, proliferative retinopathy, treated HBP, or autonomic neuropathy.
-
Fibrates, used as monotherapy or in combination therapy, have not been shown to provide overall CVD benefit in type 2 diabetes, and should not be prescribed for CVD risk reduction.
-
Fibrates show promise in prevention or treatment of retinopathy in type 2 diabetes in a manner independent of lipid lowering action.
Blood pressure
-
Lowering systolic BP in the majority of type 2 diabetes patients to around 130 mm Hg appears beneficial. Pursuing lower targets does not reduce coronary event rates, although stroke incidence may be reduced.
-
The degree of BP appears to be the critical aspect in reducing CVD risk, rather than the method or agent used to lower BP, although renin–angiotensin system blockade appears to reduce overall mortality as first line therapy.
-
The ACE inhibitor and ARBs reduce development and progression of albuminuria and reduce major renal outcomes.
-
However, blockade of the renin–angiotensin system with ACE inhibitors, ARBs or direct renin inhibitors in any combination, is associated with worse cardiorenal outcomes and should not be used.
Glycaemic control
-
The effect of intensive glucose lowering cannot be conclusively quantified, but trial results suggest a 9% and 15% reduction in CVD and CHD, respectively, for around a 0.9% (10 mmol/mol) reduction in HbA1c.
-
Recent trial findings and observational studies have noted that younger onset type 2 diabetes has an especially poor prognosis, requiring earlier intensive glucose lowering and reduction of all CVD risk factors, whereas intensive glucose lowering may not be appropriate in older patients and/or those with existing CVD.
-
The CVD benefits of intensive glucose lowering are less than can be achieved with statins or BP lowering therapy.
Aspirin
-
Low dose aspirin is not recommended for primary prevention of CVD in patients with type 2 diabetes.
2.5.1 Type 1 diabetes mellitus
Background
An increased risk of CVD in type 1 diabetes was observed over 30 years ago.300 While earlier reports indicated a four- to 10-fold relative risk compared with a younger control population without diabetes,301–307 a more contemporary large study in Scotland observed a lower relative risk of CVD of 2.3 in men and 3 in women.308 The risk of CVD is highest among those with diabetic nephropathy. A reduced incidence of nephropathy has been observed over this period, 301 ,302 ,30,9 so it appears that there has been a reduction in CVD incidence in the last 10–20 years.
There is uncertainty as to whether type 1 diabetes, acquired in childhood, accelerates CVD in all cases.3,10 Studies demonstrate that the most consistent predictors of CVD risk are age and markers of nephropathy, primarily albuminuria.302–307 ,310–31,2 Measures of dyslipidaemia, such as reduced HDL-c and hypertriglyceridaemia and, to a lesser extent, central adiposity, independently predict higher CVD risk.307 ,31,1 ,31,2 Although albuminuria has primacy in CVD risk prediction, the presence of proliferative retinopathy and autonomic neuropathy also independently added to the risk.307 ,3,10 ,31,1 There is a need to develop CVD risk scores specifically for patients with type 1 diabetes.
Treatment approaches
Lipid-lowering therapy
The rate of major CHD event rates in observational studies of type 1 diabetes were 0.98% per annum in the Pittsburgh Epidemiology Study (a small cohort of adults aged 30–40 years with duration of diabetes of 20–30 years),302 and 0.69% per annum in almost 7500 UK adults aged 35–45 years.303 A similar incidence of macrovascular disease (5% over 6–9 years follow up) was noted in over 2000 adults with type 1 diabetes in Scotland.305 The most recent evaluation in Scotland confirms the lower than previously reported incidence of first CVD event in all ages of patients with type 1 diabetes: 8.6 per 1000 person years in men and 6.8 in women.308
While all major guidelines make recommendations on lipid lowering, there is remarkably little CVD outcome data with statins in type 1 diabetes. The only major study is the Heart Protection Study, in which subjects benefited in line with the much larger type 2 diabetes cohort313; all were, however, >40 years of age, and there was no information on albuminuric status to better define baseline risk. In a meta-analysis demonstrating the benefit of cholesterol lowering therapy in diabetes, 1466 with type 1 diabetes were treated out of almost 19 000.314 However, the mean age of the type 1 diabetes cohort was 55 years, 56% had established CVD, and there was a high incidence of hypertension (48%) and nephropathy (mean serum creatinine 101 µmol/L). Consequently, the basis for intervention in different guidelines has been variably set depending on age, presence of additional CVD risk factors or microvascular complications, values of HbA1c, and family history.
Currently, there is no basis to support routine initiation of statins in type 1 diabetes aged <18 years, or in newly diagnosed cases aged ≤30 years without any risk factors. An international randomised trial of statins, ACE inhibitors, and the combination (AdDIT) in adolescents with type 1 diabetes is in progress. Women planning a pregnancy who are on statins should stop this therapy. In keeping with previous Association of British Clinical Diabetologists (ABCD), NICE, American Diabetes Association (ADA), and SIGN guidance,315–318 routine statin use is recommended in those with existing CVD, proteinuria or CKD, with the option of intensifying treatment.
Antihypertensive therapy
Antihypertensive therapy, aimed at a target BP of 120/80 mm Hg, is established practice in type 1 diabetes, with evidence of benefit from therapies that modify the renin–angiotensin–aldosterone system (RAAS) on the early development and later progression of microvascular disease in younger type 1 diabetes.319–321 Nevertheless, there are no studies of improved CVD outcome in type 1 diabetes through such an approach.
Glycaemic control
Intensive glycaemic control reduces the development and progression of microvascular disease in type 1 diabetes. The impact of glycaemic control on CVD is less clear as there appears to be a mismatch between the epidemiological observations of the relationship between hyperglycaemia and CVD,301 ,302 ,322 ,323 and the impact of intensive glycaemic control on CVD outcome in trials. These results reflect the low absolute event rates in interventional studies,324 but more recent analysis confirms that CVD reduction with tight glycaemic control may take up to 20 years to become evident.
GlyGlycaemic control, to achieve and maintain an HbA1c of 48–58 mmol/L, should be aimed for in approach to long term care of type 1 diabetes. This is feasible with structured education to effect best self-management (in order to minimise the risk of hypoglycaemia), access to regular specialist review, and use of intensive insulin regimens (including access to continuous insulin infusion treatment). Tight glycaemic control during the first decade of type 1 diabetes is considered especially important with evidence of a longer lasting legacy effect of sustained benefit. In reality, however, the majority of patients with type 1 diabetes in the UK continue to have suboptimal glycaemic control.
2.5.2 Type 2 diabetes mellitus
Background
Over 3 million (5%) of the UK population above the age of 17 years are now known to have diabetes. Type 2 diabetes had been considered as a CHD risk equivalent in terms of future CHD risk.325 It is now clear, however, that at point of diagnosis, diabetes is not a CHD risk equivalent condition,326 and certain features are required to escalate CHD risk, notably longer duration of diabetes,327 ,328 and/or presence of proteinuria.329
In the Emerging Risk Factor meta-analysis, the risk for CVD events in patients with diabetes patients was twice that of non-diabetic individuals330 and, at a population prevalence of 10%, diabetes accounts for 11% of CVD deaths. Individualisation of care in identifying cardiometabolic targets and choices of therapy is now recommended practice (NICE and ADA-EASD (European Association for the Study of Diabetes)-ESC), with a need for more intensive glucose lowering therapy earlier, especially in younger patients, and, in contrast a more conservative approach to glycaemic control and BP lowering in those aged >65 years, especially with established CVD.
Treatment approaches
Lipids
Statins are the agent of choice for patients with diabetes, based on accumulated data from several clinical trials. In the Cholesterol Treatment Trialists’ meta-analysis of outcomes in over 18 000 patients with diabetes from all relevant statin trials, a 1 mmol/L reduction in LDL-c reduced the combined endpoint of CHD death and non-fatal MI by 22%, CVD events by 21%, vascular death by 13%, and all-cause death by 9%, with no effect on non-vascular deaths.314 Similarly, coronary revascularisation was reduced by 25% and stroke by 21%.
In the UK, all patients with type 2 diabetes >40 years are considered for statin therapy. Evidence is emerging to suggest that younger patients with type 2 diabetes have higher mortality (including from CVD) than age and disease duration matched type 1 patients.16 In view of this, it would be reasonable to consider statin therapy in those aged <40 years with type 2 diabetes, particularly if any evidence of end-organ damage is present.
More intensive statin therapy should be reserved for patients with existing CVD, and those who fail to meet current non-HDL-c targets on lower doses of statins. More intensive therapy should also be considered for diabetes patients with evidence of albuminuria or CKD, as predicted by eGFR <60 mL/min, since these characteristics to confer high CVD and mortality risks, near equivalent to those with existing CVD.329 ,331 There is evidence that intensive statins are safe and effective in those with eGFR 30–60 mL/min.332
Fibrates
Two recent trials have addressed the issue of fibrate therapy in diabetes. In FIELD, a placebo controlled trial of fenofibrate in 9795 patients with type 2 diabetes, a reduction in non-fatal MI was the only significant finding, and only a minority were also on statins (17% in placebo vs 8% in fenofibrate cohorts, p<0.0001).200 The ACCORD study, which randomised 5518 patients with type 2 diabetes treated with open label simvastatin to receive either fenofibrate or placebo, found that the annual rate of first occurrence of non-fatal MI, non-fatal stroke, or death from CVD causes was 2.2% in the fenofibrate group and 2.4% in the placebo group.201 Subgroup analysis suggested that men with residual hypertriglyceridaemia and reduced HDL-c suggests possible benefited. Routine use of combination therapy with fenofibrate and simvastatin to reduce CVD risk in patients with type 2 diabetes is therefore not warranted.201 ,333 However, fenofibrate shows promise in prevention or treatment of retinopathy in type 2 diabetes independent of its lipid lowering effect.
Blood pressure
The benefits of BP lowering in type 2 diabetes are now well established. Clinical trial data (ACCORD) have suggested that CHD benefit rates are not improved below BP of 130/80 mm Hg, although stroke incidence may be reduced at lower attained levels. Although ACE inhibitors and ARBs have become established as first choice agents for BP lowering in diabetes, because of their ability to reduce the development and progression of albuminuria, a recent meta-analysis, which considered renal outcomes and mortality risks, suggested ACE inhibitors should be the first line antihypertensive treatment agent in diabetes. It also concluded that CCBs might be the preferred treatment in combination with ACE inhibitor if adequate BP control cannot be achieved by ACE inhibitors alone.334
ACCORD was the first trial to examine whether lowering systolic BP to <120 mm Hg was preferable to a 140 mm Hg target.335 The two treatment arms achieved BP results of 119 mm Hg and 134 mm Hg. Against expectations, the composite primary endpoint of non-fatal MI and stroke plus CVD death was not reduced and neither was total mortality, although stroke incidence was reduced in the intensive treatment group.
In usual clinical care, the majority of patients with type 2 diabetes require at least two, and often three, antihypertensive agents to achieve BP of 130/80 mm Hg, so the combination of renin–angiotensin system blockers with additional use of CCBs and diuretic therapy is often required. Trials have now found that combination therapy of ACE inhibitors and ARBs reduced proteinuria but at the cost of increasing the incidence of hyperkalaemia and adverse CVD events, plus reducing GFR. Thus ACE/ARB combination therapy is inappropriate.336 ,337
Glycaemic control
An understanding of the risks and benefits of intensive glucose lowering in type 2 diabetes is emerging. However, conclusions are complicated by the fact that the trials have studied differing populations, have used different agents and combinations of agents, and have pursued glucose lowering in the intensive treatment arm with varying degrees of vigour.338–341 There is support for the benefit of early (intensive) glycaemic control on the development and progression of microvascular retinal disease and albuminuria in type 2 diabetes (UK Prospective Diabetes Study (UKPDS), ADVANCE study groups). However, the ACCORD study was terminated early following the unexpected findings in the interim analysis of more all-cause and CVD deaths in the intensively treated arm. The results of four/five trials have been combined in meta-analyses.342 ,343 Both of these meta-analyses indicated that MI and major CVD events were reduced by intensive glucose control.342 However, subgroup analysis showed that whereas intensive glucose lowering was effective in lowering major CVD events in those with no known CVD, this was not the case in patients with established CVD disease. There was no apparent effect on all-cause mortality in either meta-analysis. The increases in total and CVD deaths in ACCORD and the trend towards an increase in CVD death in VADT (Veterans Affairs Diabetes Trial) have prompted concerns about the safety of intensive glucose lowering and the appropriateness of pursuing tight glucose control, particularly in older diabetics and especially in those with existing CVD. An explanation for these important findings has yet to be found, but potential suggestions include hypoglycaemia (more frequent in intensive arms), or greater weight gain. The results of these recent trials have challenged the glucocentric paradigm for prevention of CVD in type 2 diabetes, given the more robust evidence for benefits of statins and BP lowering in prevention of CVD in diabetes, as recently reviewed.344 They have also led to a patient centred approach towards the management of hyperglycaemia in type 2 diabetes.345
Finally, it should be recognised that newer classes of glucose lowering drugs have been developed in recent years and several ongoing trials will indicate whether targeting the incretin axis directly or indirectly can lower CVD risk in diabetes. Recent evidence suggests that oral gliptin therapy does not lower CVD risk in the short term (over 2 years),346 but the results of longer term studies of both gliptins and GLP-1 analogue therapies are awaited. The most recent class of agents for glycaemia are SGLT2 inhibitors, which increase glycosuria and improve glycaemia through an insulin independent renal effect. These agents also reduce weight and BP and their CVD effects are being tested in ongoing trials. However, until longer term trials with these new classes of therapy report, metformin remains the agent of choice for most patients, given its vascular benefit reported in UKPDS.
2.5.3 Aspirin in the prevention of CVD in patients with diabetes mellitus
Background
Several pieces of evidence suggest that aspirin efficacy in primary prevention of CVD in diabetes is compromised. A meta-analysis of >140 000 subjects reported that antiplatelet agents used in primary prevention (mainly aspirin) resulted in a 22% reduction in CVD events, but, in a subgroup of around 5000 diabetes subjects, the risk reduction was only 7% and not significant.347 In the Primary Prevention Project (PPP) trial involving 4495 subjects, aspirin treatment was associated with a 31% relative risk reduction of CVD events, but individuals with diabetes (n=1031) had an 11% relative risk reduction, which again did not reach statistical significance.348
Two other primary prevention studies, JPAD and POPADAD, failed to show an impact of aspirin on CVD events in diabetes.349 ,350 However, JPAD demonstrated an overall benefit in the older population and also a reduction in fatal CVD events in whole study cohort, without affecting total mortality. POPADAD was conducted in individuals with evidence of PAD and could thus be regarded as a secondary prevention study. Events rates were low in both studies.
In a meta-analysis of six studies, aspirin had no significant effect when used for primary prevention in diabetes.351 In the small Steno 2 study of high CVD risk in microalbuminuria, however, aspirin was part of a multiple risk reduction strategy and this approach was associated with a significant reduction in CVD.352 It is not, however, possible to determine the specific benefit attributable to aspirin. In contrast, it is generally accepted that aspirin is effective in secondary CVD prevention in diabetes.353
Treatment approaches
Aspirin therapy, for primary prevention of CVD in type 1 diabetes, is not currently indicated. The only potential exception is in patients with established nephropathy in whom CVD risks are very high, but further trial evidence is required to confirm this.
In type 2 diabetes, aspirin use for primary prevention is similarly no longer recommended.
2.5.4 Summary
-
CVD events rates have declined substantially in patients with type 2 diabetes over the last few decades. Such trends appear linked in part to reductions in cholesterol and BP levels in such patients.
-
While better glycaemic control can lower CVD risk, the effects are more modest than with cholesterol or blood pressure lowering and are also more difficult to achieve. Moreover, intensive glucose lowering in specific groups may be associated with harm, leading to revision of HbA1c targets, particularly in the elderly and those with existing CVD.
-
For type 1 diabetes, long term data suggest CVD rates have declined. Nevertheless, risk levels remain high and better targeting of BP, cholesterol, as well as greater efforts on smoking cessation and glycaemic control, should further reduce risk.
2.6 Chronic kidney disease
Recommendations
-
In CKD, the JBS3 risk calculator can be used to highlight the increased CVD risk and to guide appropriate risk factor modification.
Blood pressure
-
In adults with stages 3–5 CKD, with or without diabetes, BP should be treated to maintain systolic <140 mm Hg and diastolic <90 mm Hg.
-
In adults with CKD, with or without diabetes, in whom urinary albumin excretion exceeds 30 mg/day (equivalent to an ACR of 3 mg/mmol), these targets should be reduced to systolic <130 mm Hg and diastolic <80 mm Hg.
-
All antihypertensive agents are effective in adults with stages 3–5 CKD. ACE inhibitors or ARBs should be included in the antihypertensive regimen, particularly in people with albuminuria >30 mg/day (equivalent to an ACR of 3 mg/mmol)
Lipids
-
In adults with stages 3–5 CKD, lipid lowering therapy with statins should be considered in all patients.
Aspirin
-
Routine use of aspirin is not recommended for primary prevention in CKD.
2.6.1 Background
The development of a classification system based on markers of kidney damage, for example, albuminuria, and eGFR has greatly advanced our understanding of the epidemiology of CKD.354 This classification system was adopted in the UK following publication of the Renal National Service Framework in 2005,355 and modified in the NICE clinical guideline for CKD, to reflect the greater risk of adverse outcome associated with lower levels of eGFR and increased urinary protein excretion.356 Identification of people with CKD has been helped by automatic eGFR reporting by biochemistry laboratories,357 and driven by the introduction of renal indicators into the clinical domain of the Quality and Outcomes Framework (QOF). These QOF indicators are relevant to individuals with stages 3–5 CKD (ie, an eGFR <60 mL/min/1.73 m2 or <60% of normal kidney function). Publication of the CKD guideline by NICE provided a framework for the management of CKD and helped to define the remit of the providers of primary and secondary care.356
Studies in the UK indicate that the age standardised prevalence of stages 3–5 CKD (ie, an eGFR <60 mL/min/1.73 m2) is approximately 8.5% (10.6% in females and 5.8% in males), with a strong association with other comorbidities such as hypertension and diabetes.358 Importantly, prospective follow-up of individuals with CKD indicates that the risk of CVD death far outweighs the risk of progression to ‘end-stage’ kidney disease and the requirement for ‘renal replacement therapy’.359 This burden of CVD among people with CKD and the low frequency of progression has been observed in several other longitudinal studies, all of which emphasise the importance of CVD risk management in the CKD stage 3–5 population.358 ,360 ,361 Meta-analysis of the available data from the general population demonstrates that, after adjustment for age, sex, ethnicity, diabetes, BP, TC, smoking and history of CVD, a lower eGFR is associated with an increased risk of death from any CVD cause as compared to the reference group (eGFR 90–104 mL/min/1.73 m2).362 Likewise, a higher level of albuminuria is associated with an increased risk of CVD, independent of eGFR. Thus, both a low eGFR and increased level of albumin excretion are markers for CVD (and kidney) outcomes in people with stages 3–5 CKD.
Although more understanding of the mechanisms driving kidney damage and CVD risk is required, people with stages 3–5 CKD are exposed to a number of well recognised ‘traditional’ CVD risk factors such as hypertension and dyslipidaemia, which are potentially be lowered. Some of these risk factors, for example, hypertension, may drive progression of kidney disease and increase the risk of CVD complications. Prediction tools, developed on non-CKD populations, tend to underestimate CVD risk when applied to people with CKD.363 Although this might imply that traditional risk factors are less important, a number of recent interventional studies that have included or specifically targeted individuals with CKD suggest otherwise. More recently, the QRISK2 has incorporated CKD as an independent risk multiplier, rendering it an appropriate CVD risk tool for these individuals. This is incorporated in the new JBS3 calculator.
2.6.2 Treatment approaches
Blood pressure
Most trials of BP lowering, involving people with CKD, have examined progression of kidney damage rather than CVD events as an outcome. These trials have assessed both optimal BP and how best to achieve BP control using available antihypertensive regimens. Long term follow-up of individuals in the Modification of Diet in Renal Disease (MDRD) study indicated that treatment to a tighter BP target of 125/75 mm Hg instead of 140/90 mm Hg slowed progression of kidney disease in non-diabetic individuals, but this benefit was only seen in those with proteinuria (>1 g/24 h).364 This finding was endorsed by a long term follow-up of participants in the African American Study of Kidney Disease and Hypertension (AASK) trial, among whom tighter BP control slowed progression, but again only in proteinuric individuals (protein: creatinine ratio (PCR) >350 mg/24 h).365
Trials involving people with proteinuric CKD who do not have diabetes have generally favoured the use of agents that block the renin–angiotensin–aldosterone pathway over alternative strategies, at least from the perspective of slowing kidney disease progression.297 ,366 It is less certain whether the use of ACE inhibitors or ARBs is associated with cardiovascular benefits in individuals with CKD without diabetes and/or proteinuria. Several large studies comparing these agents with alternative antihypertensive strategies have included people with CKD, but analysis of data from these subgroups is inconsistent.
Thus, recommendations for the management of BP in people with CKD stage 3–5 are largely based on our understanding of the cardiovascular benefits of BP reduction in non-CKD populations, the knowledge that ‘tighter’ control of BP slows progression of kidney damage, and that agents that block the renin–angiotensin–aldosterone system may have clinical benefits over other BP lowering agents, particularly in proteinuric individuals. The NICE CKD guideline recommends controlling BP to <140/<90 mm Hg in people with CKD, unless the ACR is ≥70 mg/mmol or PCR ≥100 mg/mmol, in which case the BP should be <130/<80 mm Hg.356 These levels are endorsed by an international guideline published by Kidney Disease: Improving Global Outcomes (KDIGO) in which the albuminuria ‘cut off’ for the lower BP target was 30 mg/day.367 Both the NICE and KDIGO guidelines recommend offering agents that block the renin–angiotensin–aldosterone system to individuals with albuminuria/proteinuria, although again the thresholds for intervention are somewhat different. The more recent KDIGO guideline suggests that these agents should be used even in the presence of microalbuminuria (urinary albumin excretion 30–300 mg/day).
Lipids
CKD is generally associated with elevated triglyceride and low HDL-c values.368 Except in people with heavy proteinuria, total and LDL-c are normal or low compared to a matched population without CKD.369 Furthermore, the value of measuring TC and LDL-c concentrations in an effort to stratify CVD risk, particularly in advanced CKD, is uncertain.370 Although elevated lipid concentrations may not be the main driver of CVD in the context of CKD, the available data generally support the use of lipid lowering regimens to reduce the risk of CVD events. Post hoc identification of people with CKD stages 1–3 recruited into large ‘statin’ trials suggest that lipid lowering therapy reduces the risk of CVD events, as in individuals with normal kidney function.371 More robust, prospectively collected data are available from the SHARP study in which 9270 people with CKD (including 6247 with predominantly stages 3–5 disease not receiving dialysis at the time of recruitment) were randomised to receive either the combination of ezetimibe 10 mg plus simvastatin 20 mg or placebo.372 With an average LDL-c difference of 0.85 mmol/L (with about two thirds compliance) during a median follow-up of 4.9 years, there was a highly significant 17% reduction in major CVD events among those randomised to ezetimibe/simvastatin, as would be predicted from a meta-analysis of existing LDL lowering trials in predominantly non-CKD populations.244 Subgroup analysis on baseline total and LDL-c showed the expected trends with a greater proportional effect observed among those with higher baseline values. The approach to LDL lowering used in SHARP using a statin/ezetimibe combination avoided exposing patients to high doses of statin. Whether a similar reduction in CVD events could have been achieved with a high dose of statin alone (achieving an equivalent LDL-c reduction), with an acceptable number of adverse events, is uncertain. Recent international guidelines from KDIGO recommend that people with stages 3–5 CKD not receiving dialysis are offered a statin (or statin/ezetimibe combination), particularly if >50 years of age or at an arbitrary higher level of risk based on risk prediction equations.373
Aspirin
There have been no appropriately sized trials of aspirin examining CVD clinical endpoints in any CKD population. Some data are available from post hoc analyses of large trials. For example, in the Hypertension Optimal Treatment trial, aspirin was of benefit in a subgroup of individuals with stage 3 CKD at the time of recruitment.374 There is very little information about the effects of aspirin among those people with CKD stages 4–5 and an increased risk of minor bleeding is recognised which may offset any benefits.375 A recent Cochrane review concluded that this hazard may outweigh any benefits of aspirin in people with CKD.376
2.6.3 Summary
-
In CKD, the JBS3 risk calculator can be used to highlight the increased CVD risk and help inform appropriate risk factor modification.
-
In adults with stages 3–5 CKD with or without diabetes, BP should be treated to maintain systolic <140 mm Hg and diastolic <90 mm Hg.
-
In adults with CKD in whom urinary albumin excretion >30 mg/day (equivalent to an ACR of 3 mg/mmol) these targets should be reduced to systolic <130 mm Hg and diastolic <80 mm Hg.
-
ACE inhibitors or ARBs should be included in the antihypertensive regimen.
-
In adults with stages 3–5 CKD, lipid lowering therapy with statins should be considered in all patients.
-
Routine use of aspirin is not recommended for primary prevention in CKD.
2.7 Chronic inflammatory disease
Recommendations
-
There is clear evidence of heightened CVD risk in patients with RA as summarised in recent EULAR consensus document.
-
The JBS3 risk calculator now incorporates the appropriate multiplier for CVD risk, based on the presence of RA.
-
Intensive management of traditional CVD risk factors should be undertaken in patients with RA, taking into account their CVD risk score.
-
Optimisation of inflammation suppression with disease modifying antirheumatic drugs may also help reduce CVD risk.
-
CVD risk may be lowered by use of the minimum effective glucocorticoid dose for the shortest possible time.
-
Where anti-inflammatory drugs are indicated for symptoms, in those patients with an average gastroduodenal damage risk, the use of a conventional NSAID with gastroprotective agent is preferable to use of a COX-2 selective inhibitor.
-
Clinical judgement may be used to determine whether a risk multiplier should be applied to patients with other autoimmune conditions.
2.7.1 Background
CVD mortality and morbidity, particularly due to ischaemic heart disease and cardiac failure, is significantly increased in persons with rheumatoid arthritis (RA) or systemic lupus erythematosus compared with age and gender matched controls from the healthy general population. This is also likely to be true for a broader range of inflammatory rheumatic disorders, including ankylosing spondylitis and psoriatic arthritis.377 However, the most compelling available data is for RA, a systemic inflammatory syndrome with its major manifestations in the peripheral synovial joints and a prototypical condition associated with accelerated CVD and increased CVD events.378–382
There is a clear association between smoking and RA pathogenesis, particularly in individuals carrying certain HLA (human leucocyte antigen) DR alleles encoding a conserved amino acid sequence in the DRB1 chain. Other than this smoking association, the prevalence of traditional CVD risk factors is not significantly elevated in RA cohorts. Therefore, the driver of CVD risk is thought to be systemic inflammation, both through its adverse impact on traditional risk factors as well as by direct effects on the vasculature.383–385
The European League Against Rheumatism (EULAR) has published recommendations for managing CVD risk in patients with inflammatory arthritis.386 These include use of the systematic coronary risk evaluation score (SCORE), an assessment equation comprising multiple major traditional risk factors. Additionally, it is recommended that a multiplier of 1.5 should be applied to SCORE in RA patients who meet at least two of the following three criteria: disease duration >10 years; seropositivity for rheumatoid factor or anti-citrullinated peptide antibody; extra-articular disease features. Application of this multiplier creates a modified (m) SCORE.
Evidence suggests that traditional risk factors, assessed in the mSCORE, may underestimate CVD risk in patients with rheumatic diseases. For example, a recent study reported a risk of CVD in female RA patients of twice that predicted by the Framingham risk score and in male patients, 65% higher.387 In another study, RA patients with evidence of carotid artery plaque had an incident event rate for CVD exceeding 39%, whereas the mean Framingham score classified the cohort as having a risk as low as 7%.388 An alternative measure, the Reynolds risk assessment score, adds measurement of high sensitivity C reactive protein concentration as well as taking into account any family history of premature CVD. This refined risk assessment also, however, underestimates the true CVD risk in patients with RA.387 More recently, the findings of a large observational cohort study suggested that both traditional CVD risk factors and markers of disease activity contribute to models predicting CVD events, with an observed event rate of 3.98 per 1000 patient years.389 This weakening of the association of traditional risk factors with CVD event rates in patients with RA is presumably a consequence of the contribution of systemic inflammation to CVD risk.383 The same may be true in other chronic inflammatory musculoskeletal disorders, such as ankylosing spondylitis.390
In line with the above observations, the QRISK2 risk engine has shown that patients with RA have an elevated CVD risk independent of other risk factors, with adjusted HRs of 1.50 (95% CI 1.39 to 1.61) in women and 1.38 (95% CI 1.25 to 1.52) in men with RA, respectively.28 Thus, QRISK2 captures and incorporates the excess risk of CVD associated with RA using a categorical adjustment based on the presence of RA, and this is represented in the JBS3 risk calculator.
In RA the relationship between lipids and CVD events is inconsistent across studies,381 and, in one case, has even been reversed.391 This may in part reflect alterations in lipid biology that accompany the chronic inflammatory state, as recently comprehensively reviewed.392 The best data seem to suggest that TC and HDL-c values change in the same direction, inversely to changes in inflammation; thus consideration of both TC and HDL–c are important to determine CVD risk in RA patients regardless of what treatments they are receiving.
2.7.2 Treatment approaches
The role of conventional risk modifiers in improving CVD outcomes is not yet fully clear. Nonetheless, it is encouraging that in post hoc analyses of two prospective trials that assessed the impact of intensive compared with conventional treatment with statins on CVD outcome, patients with and without inflammatory joint disease were found to experience comparable lipid lowering effects with accompanying reductions in CVD.393 These results therefore supported findings from the Trial of Atorvastatin in RA randomised trial, which showed that RA patients have comparable LDL-c reduction with statins to those previously noted in general population studies.394
Recent findings from a large meta-analysis of clinical trials of NSAIDs show that the risk of major CVD events, mostly major coronary events, is increased by one third in people taking coxibs or high dose diclofenac. Ibuprofen significantly increased the risk of major coronary events but not major vascular events. Compared with other traditional NSAIDs (not coxibs), high dose naproxen was not associated with an increased risk of major vascular or coronary events. All NSAIDs were associated with an increase in the risk of heart failure hospitalisation.395 Similarly, therapeutic use of supraphysiological doses of glucocorticoids may be associated with increased CVD risk which may be mediated, at least in part, by elevated lipoprotein values.
CVD risk management is likely to require not only adequate treatment of traditional CVD risk factors but also tight disease activity control in RA. Treatment with methotrexate was associated with a ∼20% lower risk of CVD events in RA.396 In a retrospective observational study of 983 Swedish rheumatoid patients treated with biologic tumour necrosis factor (TNF) inhibitors and a comparator group not receiving these biologic agents, the incidence rates of new CVD events were around half in the TNF blockade recipients.397 Such benefits may be restricted to those patients who exhibited a therapeutic response with respect to synovitis reduction.398 There is, however, a lack of randomised trials to support these observations. Ongoing trials of anti-inflammatory agents on CVD outcomes in the wider CVD population are awaited with interest.
2.7.3 Ongoing/unresolved issues
The relationship between antirheumatic drugs and CVD risk is difficult to tease apart due to confounding by indication/contraindication. Furthermore, use of anti-inflammatory drugs such as glucocorticoids and NSAIDs, especially selective COX2 inhibitors, may actually accelerate atherosclerosis and coronary thrombosis, whereas other agents such as methotrexate and biologic TNF inhibitors may reduce risk. Overall, there is a lack of hard evidence with respect to CVD prevention in patients with RA and therefore many questions remain unanswered. Future work should focus on further delineating the pathobiology involved, developing and evaluating better risk assessment tools and biomarkers, and effective prevention strategies relevant to chronic inflammatory musculoskeletal diseases. Further assessment of evidence for CVD risk in autoimmune conditions other than RA is needed.
2.7.4 Summary
-
Patients with RA are at increased (approximately 1.4- to 1.5-fold) risk for CVD events, a factor now captured in the QRISK2 risk engine.
-
The excess CVD risk is thought to be driven principally by systemic inflammation.
-
Current evidence suggests disease modifying antirheumatic drugs and biologics are likely to reduce CVD risk, whereas chronic high dose steroids may increase CVD risk.
-
All patients with RA would benefit from CVD risk factor screening.
-
Patients with chronic inflammatory disease at high absolute 10-year CVD risk, as defined by NICE, and at high lifetime risk using the JBS3 calculator, should be treated with statin therapy.
-
The use of a risk multiplier for CVD risk assessment in autoimmune conditions other than RA should be considered on a patient by patient basis, depending on disease severity.
2.8 Chronic obstructive pulmonary disorder/sleep apnoea
Recommendations
-
Lifestyle advice to support weight loss should be offered to all patients with a diagnosis of obstructive sleep apnoea/hypopnoea syndrome (OSAHS) who are obese or overweight.
-
Patients with significant daytime sleepiness and confirmed OSAHS should be offered continuous positive airway pressure treatment.
-
CVD risk factors should be assessed using the JBS3 risk calculator and managed according to JBS3 recommendations in these patients.
Background
Cardiovascular impact of obstructive sleep apnoea
Obstructive sleep apnoea (OSA) is part of a spectrum of sleep related breathing disorders ranging from simple snoring through to obesity related hypoventilation syndrome. It is defined and diagnosed by the presence of apnoeic/hypopnoeic episodes that occur during sleep that are associated with oxygen desaturations followed by an arousal characterised by sympathetic nervous system activation. These are caused by either cessation of airflow (apnoeas) or reduction in airflow (hypopnoeas). The most common presenting symptoms are daytime sleepiness and loud snoring associated with witnessed apnoeas. This comprises obstructive sleep apnoea/hypopnoea syndrome (OSAHS). Severity is assessed by a combination of symptoms and objective evidence of apnoeas/hypopnoeas measured during an overnight sleep study. An apnoea/hypopnoea index (the number of events per hour slept) of <5 is considered normal; 5–14, mild; 15–30 moderate; and >30 severe.399 OSAHS is common in obese patients with multiple cardiometabolic risk factors and therefore included in JBS3. It is not yet clear to what extent it may contribute directly to CVD events or be a marker for increased CVD risk.
The overall population prevalence of OSAHS in adults is around 4% in men and 2% in women, but it is much more common in the obese; about 1% of men will have moderate to severe OSAHS. Epidemiological studies have shown associations with cardiometabolic risk factors, including hypertension, dyslipidaemia, insulin resistance, and the development of type 2 diabetes that is partly independent of adiposity400 ,401; this has also been observed in well matched case–control studies.402–404
This increase in risk factors translates into increased CVD risk. The magnitude of the effect depends on the severity of OSAHS and the presence or absence of preceding CVD, but overall a diagnosis of OSAHS results in a two- to fourfold increase in CVD events, including MI, stroke, CVD mortality, and sudden death.405 ,406
Mechanisms
There are several possible mechanisms by which the presence of OSAHS might adversely affect CVD risk, but their relative importance is uncertain. The cardinal features of OSAHS are intermittent nocturnal hypoxia and sleep disturbance, both of which might directly and indirectly influence CVD risk.402
Identified mechanisms for which there is supporting experimental evidence include:
-
Increased sympathetic nervous system activity as a result of repeated arousals from sleep—this may contribute to rise in BP and heart rate, and potentially increase risk of cardiac arrhythmias; it could also contribute to increased insulin resistance and impaired insulin secretion.
-
Increased activity of the hypothalamic–adrenal axis—this occurs as a result of sleep disruption and could contribute to development of hyperglycaemia and dyslipidaemia.
-
Intermittent hypoxia—this occurs as a direct result of apnoeic episodes and may contribute to insulin resistance and development of an inflammatory state (a recognised feature of sleep apnoea) in adipose and other tissues.
2.8.2 Treatment approaches
Continuous positive airway pressure (CPAP) ventilation is the most widely used and accepted treatment and has been shown to reduce daytime sleepiness and lower BP.407 RCTs on other cardiometabolic risk factors have shown conflicting results.408 ,409 Observational studies have shown reduced CVD mortality in patients with severe OSAHS treated with CPAP compared to those who chose not to have treatment,410 ,411 but there are no RCT data on CVD outcomes.
NICE guidelines (TA 139) recommend CPAP treatment for those diagnosed with moderate to severe OSAHS (Apnoea Hypopnoea Index ≥15).399
Those with mild OSAHS (Apnoea Hypopnoea Index 5–14) should be treated only if:
-
They have symptoms that affect their quality of life and ability to go about their daily activities, and
-
Lifestyle advice and any other relevant treatment options have been unsuccessful or are considered inappropriate.
The diagnosis and treatment of OSAHS, and the monitoring of the response, should be carried out by a specialist service.
2.8.3 Ongoing/unresolved issues
There are few RCTs of the effects of CPAP therapy on CVD risk factors and none which look at hard CVD outcomes (MI, stroke, CVD death). These trials require the use of sham devices which might affect compliance and may not be adequately blinded; it is unethical to withhold treatment for prolonged periods of time, so most trials have been too short in duration to answer these questions. Observational data does not provide sufficient evidence to support treatment with CPAP solely on the basis that it might reduce CVD risk.
2.8.4 Summary
-
OSAHS is associated with obesity.
-
Elevated cardiometabolic risk profile and diabetes are more likely to be present in patients with OSAHS, independent of obesity.
-
Clinicians should be aware of the associations between OSAHS and CVD risk factors including type 2 diabetes and enquire about daytime sleepiness in those at high CVD risk.
-
Lifestyle advice should be offered to all patients with a diagnosis of OSAHS.
-
There is good evidence from trials and meta-analysis that OSAHS treatment with CPAP in patients with moderate to severe OSAHS improves sleepiness and quality of life and results in modest BP lowering.
-
There is limited and conflicting RCT evidence that CPAP treatment in OSAHS might reduce other CVD risk factors.
-
Some observational studies suggest that OSAHS treatment may reduce CVD events, particularly in patients with moderate to severe OSAHS who are symptomatic, but there are no randomised trials.
-
Patients with significant daytime sleepiness and confirmed OSAHS should be offered CPAP treatment (alongside lifestyle advice to help them lose weight if they are obese); CVD risk factors (BP, lipids, hyperglycaemia) should be measured and managed according to JBS3 recommendations.
2.9 Implementation
Recommendations
-
All patients with established CVD should have access to evidence based prevention/rehabilitation programmes addressing lifestyle, risk factor management, and adherence to drug therapies.
-
A national screening programme for ascertainment of FH cases should be supported including cascade screening and specialist referral.
-
The JBS3 approach linked to professional and public health initiatives, such as the NHS Health Check in England, should be used to promote better uptake of lifestyle improvements (and where required drug therapy) in primary care. This should include development of a CVD prevention strategy for individuals who, despite low short term risk, are found to have a high lifetime risk of developing CVD and its complications.
2.9.1 Introduction
The challenge for JBS3 has been to develop and implement a strategy for CVD prevention that encourages the adoption and maintenance of a healthier lifestyle by the population and, at the same time, guides practitioners to provide professional lifestyle support and prescribe drugs, in a cost effective manner, to individuals to reduce their lifetime CVD risk.
The risk factors that drive CVD are familiar and, in combination, account for the majority of CVD events.412 Since JBS2, there has been considerable new information on the potential benefits of reduction of these risk factors. This can be facilitated by adoption of a lifestyle which involves a healthy diet, increased physical activity levels during normal daily life, and weight control as well as by exercise. It is also clear that there is benefit, for some individuals, from the use of drugs to achieve reduction of risk factors to substantially lower levels. For example, reduction of LDL-c to values below those recommended even 5 years ago has been shown to have clinical benefit, and can be achieved, in a cost effective manner, using statin therapy.11 For BP and glycaemia, there are also benefits from improved control, but the risk/benefit of intensive treatment for patients with advanced longstanding disease is less certain.413 Patients with manifest CVD are at the highest risk of future cardiovascular events. In addition, individuals may be at high risk because of the presence of multiple CVD risk factors and associated diseases such as diabetes or CKD. Others may be at substantially increased lifetime risk because of elevation of a single modifiable risk factor, such as those with FH.
CVD is the most common cause of disability and death in the population. As a result, CVD prevention strategies have the potential to benefit large numbers of people, and JBS3 includes recommendations for implementation of CVD prevention in all of the above categories of ‘risk’.
2.9.2 Patients with established CVD
A comprehensive programme is required for patients with the broad range of clinical CVD presentations. These include acute coronary syndrome (STEMI, non-STEMI (NSTEMI), and unstable angina), exertional angina, or transient cerebral ischaemia, stroke, and PAD. These different clinical presentations are associated with a common pathology of atherosclerosis and common underling risk factors, particularly smoking, high BP, elevated cholesterol, diabetes, obesity, and unhealthy lifestyle. Many patients presenting with one clinical manifestation of CVD also have disease in other territories. They should therefore not be managed in silos of specialist care, which can result in multiple uncoordinated consultations and often in the delivery of confusing or contradictory information. Coordinated expert care is required and this should be delivered and supported by both specialist prevention programmes and primary care. These programmes are variously labelled ‘cardiac rehabilitation’ and ‘secondary prevention’, but it is clear that they should provide a comprehensive approach including education, lifestyle, risk factor reduction, and drug therapy which is tailored to the individual needs of the patient. Meta-analysis has shown that integrated, multidisciplinary, multifactorial approaches deliver improved quality of life, fewer recurrent CVD events, and improved life expectancy.414 Despite the delivery costs of these programmes, they have been shown to be highly cost effective as they reduce readmission rates and recurrent CVD events.414 NICE guidance recommends attendance and completion of a formal ‘cardiac rehabilitation’ programme and the BACPR have published minimum standards and a set of core components (see Lifestyle section).172 These standards define the elements required for a comprehensive multifactorial approach which is sustainable. Risk factors could also be greatly improved as shown in the Aspire-2-Prevent survey of a random sample of 676 coronary patients from 19 specialist and general hospitals. Almost half of those smoking at the time of hospitalisation continued to smoke, and had a BP of ≥130/80 mm Hg or a TC of >4 mmol/L, and about one fifth had diabetes. These findings are consistent with other European countries. It is important that patients are assessed early, a treatment plan is defined, and that this is agreed with the patients and their families which may be more effective at achieving prevention goals. This model of ‘cardiac rehabilitation’ is strongly endorsed by JBS3 and supported by NHS England.
Unfortunately, the uptake of such evidence based programmes in the UK remains disappointing.7 The National Audit of Cardiac Rehabilitation (NACR) revealed daunting challenges for current NHS programmes.415 Although there are some high performing rehabilitation programmes, average uptake remains low, with only 42% of patients accessing these programmes following an MI and even longer after surgery. Those with angina or other CVD presentations are rarely included. The median waiting time to join a programme is 7 weeks which falls well short of the ambition to have patients assessed within 2 weeks of diagnosis or discharge. Improved enrolment and adherence to ‘prevention and rehabilitation programmes’ after CVD events should be a major goal of national CVD prevention. Patients with established CVD are easy to identify and improvements in their CVD prevention should be achievable with more effort and support. Ongoing research will refine prediction of risk and thus optimal behavioural and drug interventions for the increasing number of patients who survive their first CVD presentation, but who remain at very high risk.
2.9.3 High CVD risk due to genetic elevation of CVD risk factors
FH is the best example of a common genetic disorder that results in very high lifetime risk of CVD, due to elevation in a single modifiable risk factor. There is now evidence that drug treatment from an early age reduces this risk substantially. Ascertainment of these individuals and their families is therefore the key issue, but most remain undetected at present. JBS3 strongly supports current efforts to screen and refer such patients for specialist management.416 The success of this programme will depend largely on the efforts of GPs and nurse specialists.
2.9.4 Broader CVD prevention strategies
The major challenge for CVD prevention is the identification and management of individuals who have not yet had a CVD event but who are at risk in the future. JBS3 has proposed a new approach to the estimation of CVD risk that not only identifies those at high absolute short term (10-year) risk, but also the many people in the population who are at low short term risk but whose CVD risk profile nevertheless puts them at high lifetime risk of a future CVD event. Many younger subjects and women fall into this category. This change in approach offers the opportunity for a dialogue between the healthcare professional and the individual which is designed to empower them to understand their personal CVD risk and to ‘take control’ of their own management. This will involve, for most, adoption of a healthier lifestyle and, for some, the need for drug therapy. The novel displays presented in the JBS3 calculator are designed to be understood by a broad range of individuals and readily illustrate the potential gains which may be achievable over life by early and sustained lowering of risk factors, even by modest amounts.
The JBS3 approach, with utilisation of the new calculator, provides an exciting opportunity to link with the NHS Health Check programme in England to implement a comprehensive CVD prevention programme at a population level.417 This would also be applicable to similar programmes in other countries. In England, patients are invited for a structured evaluation of their CVD risk profile from the age of 40 years. At this age, 10-year risk estimates are of limited value. Communicating heart age and other lifetime risk measures at the time of the Health Check should make the risk factor measurements more meaningful. This should motivate behavioural changes. It is also hoped that it will encourage referral to comprehensive services which address smoking cessation, diet and weight management and exercise as well as control of BP, lipids, and diabetes. The CVD Outcomes Strategy in England highlights the need for enhanced participation in these programmes and has called for a “coordinated and integrated approach to assessment, treatment and care to improve outcomes including patient experience and safety”.8 The JBS3 approach will broaden indications for CV prevention efforts by lifestyle and forms the basis for a population based public health approach to reduction of CV risk across the whole spectrum of risk including, for the first time, those at high lifetime risk. Implementation of JBS3 recommendations will not only be the responsibility of cardiologists or rehabilitation specialists but will depend on the efforts and enthusiasm of GPs and practice nurses to deliver change. Effective CVD risk reduction for large numbers of individuals who have modest short term risk but high lifetime risk is likely to have a much greater impact on the cardiovascular health of the population than intensive targeting of the relatively small number of individuals at high short term risk (accepting the proven value for these individuals).
Currently, the gap between evidence based guidelines and clinical practice in primary care is even greater than for patients with established CVD. The ASPIRE-2-PREVENT survey of primary prevention showed persistent high levels of smoking, obesity, hypertension, diabetes, and dyslipidaemia 1 year after commencing drug treatment for CVD risk factors7 The JBS3 calculator emphasises the need for a multifactorial approach and enables estimation of the increased benefits from reduction in levels of multiple risk factors rather than treatment of individual risk factors. It also emphasises the benefits of long term reduction of risk factors. Local authorities, public health, and GP practises in clinical commissioning groups (CCGs) or Health Boards should work together to implement the JBS3 approach and assess its impact.
The effect of multiple risk factor intervention to reduce CV risk factors, mortality from CVD, and total mortality in patients without clinical CVD has thus far been disappointing.418 This is likely to reflect the modest success achieved in reducing risk factors and the lack of sustainability. In trials of higher risk individuals (eg, with diabetes), the impact of lowering of individual risk factors and of multiple risk factor lowering strategies on outcomes has, however, been much more impressive.419 Previous programmes, which included incentive payments in the QOF, have been associated with significant improvements in the achievement of CVD risk factor reduction, and such initiatives should be considered to support an increased emphasis on CVD prevention.420 ,421
JBS3 provides new tools for understanding of not only the short term but also the long term impact of CVD risk factors. Its implementation should be invaluable both to healthcare professionals by providing a rational framework for management of CVD risk in individual patients as well as, more widely, to engage the public in efforts to reduce the population burden of CVD. Targeting CVD risk in this way requires a reconfiguration of prevention strategies and many stakeholders will need to be engaged. Greater collaboration between clinicians, healthcare providers, commissioners of healthcare, public health, politicians, and the general public is essential. Without it the substantial gains achieved in CVD outcomes may not be maintained in the future.
2.10 Research gaps and opportunities
2.10.1 Risk calculator
The Holy Grail of CVD prevention is not only to design strategies to reduce population risk of developing the disease in the first place, but also to identify individuals at high risk who will benefit from pharmacological interventions in a cost effective manner.
It is inevitable that when formulating a set of guidelines for the prevention of any common disease, there will be gaps in the underpinning evidence base. While this is certainly true for the JBS3 recommendations, the biggest obstacle to CVD prevention in the UK is the failure to implement successfully strategies based on existing evidence. Few would dispute that less smoking and lower population BP and LDL-c values would result in a substantial reduction in CVD. Further, for many this can and should be achievable, largely by behaviour modification rather than with drugs. But, short of legislation, population behaviour change is difficult to achieve, particularly in those most in need of it. Behaviour change requires motivation and individuals will only feel motivated if they understand the benefits of changing behaviours and the risks of not changing. This is why JBS3 has focused so much on communication of risk and how and when it should be modified. The biggest change in the JBS3 recommendations from previous guidelines is the emphasis on lifetime management of CVD risk. This has been well received in limited testing, but full evaluation of the impact of this approach is required. It is surprising that very little work has yet been done to determine the attitude of the public to many of the lifestyle and drug treatment strategies that have been proposed. In the UK, there is an exciting opportunity to study the JBS3 approach based on ‘big data’. The NHS Health Checks programme and the large registries of anonymised data which have been collected in national registries will be helpful (National Institute of Cardiovascular Outcomes Research (NICOR)). Such research is now needed to understand how best to use the risk calculator in different populations as a tool to bring about beneficial behaviour change, particularly in relatively young individuals at lower short term risk, but who are potentially at high lifetime risk.
2.10.2 Risk refinement
Risk prediction is not an exact science and is based on probabilities within populations. All risk assessment tools have their shortcomings and researchers continue to explore ways of refining them to make them more relevant to particular individuals. In this context, genetic research, in particular GWAS, has so far produced disappointing results from a risk prediction perspective, although promising new pathways for therapeutic intervention have been identified. Further research is needed to establish whether genetic testing for CVD, except for testing for FH, is likely to add sufficient discriminatory power to current risk assessment algorithms to justify its routine use in future risk assessments.
For asymptomatic individuals estimated to be at moderate to high risk, in whom drug treatment is being considered, there is a need to discriminate those with occult CVD from those that remain disease free, despite their risk factors. This is important to enable drug therapy to be targeted effectively. Despite decades of research, a reliable and cheap biomarker for the presence of CVD remains elusive. Further research is needed to establish the role of circulating biomarkers, as well as measures of disease burden such as CT coronary artery calcium imaging, for identification of high risk asymptomatic individuals with or at high risk of CVD.
2.10.3 Risk factors
JBS3 reports at a time when CVD risk profiles in the population are changing, with a decrease in cigarette smoking, but a substantial increase of the prevalence of obesity especially in the young. This is predicted to have an important impact on the future incidence of CVD, mostly through levels of associated risk factors and type 2 diabetes. Prevention of childhood obesity is clearly the best but most challenging strategy, while much more research is needed to understand the underlying pathobiological mechanisms underpinning the association between obesity and CVD risk across all ages and how best to intervene to prevent CVD complications. The JBS3 calculator does not fully estimate CVD risk associated with weight and its modification as these data are not yet available.
Diabetes is a potent risk factor for CVD, but much uncertainty remains as to whether conventional pharmacological approaches to CVD event prevention, for example, with aspirin, confer an equivalent degree of protection in patients with either type 1 or type 2 diabetes, compared to that demonstrated in the non-diabetic population. Furthermore, the extent to which drugs primarily targeted at glycaemic control confer protection against atherogenesis and cardiovascular events remains far from clear. Ongoing trials are addressing these issues. In addition, better risk scores are needed to help guide the use of CVD preventative therapies in younger patients with both type 1 and type 2 diabetes.
There are also important unanswered questions about the management of traditional CVD risk factors, such as hypertension and hypercholesterolaemia. The early empirical approach to drug use for BP lowering has evolved into a more stratified approach based on physiological logic. Future research should help to define the extent to which the impact of different treatments and their combinations can be linked to understanding of the pathophysiology of hypertension. As emphasis moves towards management of lifetime risk of CVD events, more research is needed to establish which haemodynamic measurement among, for example, brachial BP, central aortic pressure, or augmentation index helps improve identification of young individuals who are most at risk of premature CVD events and how best to manage them.
The importance of LDL-c reduction in CVD prevention is now well established, although further research is still needed to understand better the role of non-LDL-c components and triglycerides in the pathogenesis of CVD and whether pharmacological manipulation of these components can confer additional benefits. Experience so far with attempts to raise HDL-c has been very disappointing, while in contrast, research into non-statin approaches to LDL-c reduction with, for example, antibodies to PCSK9 is looking promising. The ‘lower is better’ approach to LDL-c has been clearly supported in landmark trials, but the impact of achieving very low concentrations of LDL-c on progression and regression of arterial disease needs further research. The lifetime risk approach in JBS3 recommendations is based on evidence which suggests that long term exposure to risk factors promotes disease development. This represents an opportunity to benefit CVD outcomes by early and sustained risk factor lowering. This will need testing using subclinical endpoints of CVD progression initially and, in time, with clinical outcomes.
2.10.4 Novel associated diseases
JBS3 incorporates recommendations on a number of disease states which have recently been recognised to contribute to CVD risk.
Chronic kidney disease
Even modest impairment of kidney function increases CVD, but the mechanisms linking CVD mortality and CKD remain poorly understood. Current treatment strategies rely on close attention to conventional CVD risk factors in the CKD population. Nevertheless, epidemiological evidence suggests that there are other factors over and above these that confer particular CVD risk and further research is needed to identify them.
Chronic inflammatory disease
The pathophysiological basis for the well established link between chronic inflammatory disease and increased CVD risk is poorly understood and has been complicated by the relatively recent recognition that some NSAIDs can increase CVD event rates, independently from their effects on the underlying inflammatory disease. There is limited evidence on which to base CVD prevention strategies specifically in patients with chronic inflammatory diseases and much more research needs to be done in this group of patients. The opportunity to reduce CVD risk by anti-inflammatory agents, in patients with CVD but no other chronic inflammatory disorders, is currently being tested in large randomised trials. The findings will be important both for the understanding of pathophysiology and potentially for treatment.
Obstructive sleep apnoea/hypopnoea syndrome
Patients with OSAHS are at increased risk of CVD events, but the underlying mechanistic links remain poorly understood. There is no research based evidence to guide preventive treatment of this group. Further research is therefore clearly needed to determine whether the increased CVD risk is mediated through conventional risk factors that can be addressed with existing treatment approaches, or whether managing the apnoea itself, for example, with CPAP, confers any independent protection against future CVD events.
2.10.5 Clinical CVD presentations
JBS3 emphasises the diffuse nature of CVD and its associated clinical presentations. Many risk factors and treatment principles are common to cardiac, cerebrovascular, and peripheral arterial presentations but a number of specific research questions remain.
Peripheral arterial disease
PAD is common and frequently undetected despite there being a cheap and reliable clinical tool to identify it—measurement of ABPI. Patients with PAD are at high risk of future heart attacks and strokes, yet ABPI is rarely measured in primary care. Research is needed to establish whether ABPI can meet the criteria needed for recommendation by the National Screening Committee. In comparison with coronary disease and cerebrovascular disease, less research has been performed on risk factor modification in PAD. Studies are needed to determine the most effective preventive strategies in patients with PAD, who are often older and may have more advanced disease at the time of detection.
Cerebrovascular disease
While most of the measures taken to prevent ischaemic heart disease have similar or equivalent protective effects against stroke, many questions remain unanswered on how best to approach prevention in someone who has already experienced a stroke. Thus further studies are needed to determine the choice and timing of statins, antihypertensive and antiplatelet therapies following the initial event.
The past decade has seen an unprecedented increase in the prescription of drugs to healthy individuals, in the expectation that future CVD events will be delayed or averted. But drugs can have side effects and unexpected consequences, both beneficial and detrimental, that randomised clinical trials are sometimes unable, for a variety of reasons, to identify. Most such effects become apparent long after the drug has been in widespread clinical use. For example, evidence gained from patient databases has pointed to an unexpected potential protective effect of aspirin against the incidence and dissemination of some cancers, while similarly derived data on ARBs, used widely in the treatment of hypertension and heart failure, failed to confirm a postulated link between these drugs and cancer. Observations like these provide a powerful argument in favour of the current move in England to making anonymised NHS patient data more readily available to researchers. The emphasis in JBS3 in long term management of CVD risk should encourage more research in the population and in primary care.
The approach to CVD prevention tends to be similar in men and women and in different ethnic groups, yet there is substantial evidence that both CVD risk and possibly also response to preventive medication may differ by gender and ethnic origin. Further research is therefore needed both in the form of prospective randomised trials and in the form of patient data surveillance to establish how best to achieve equitable CVD prevention across both genders and different ethnic groups.
2.10.6 Lifestyle changes
Diet
While it is beyond doubt that diet has a significant influence on health, the evidence base for the contribution of specific dietary components to the development of CVD is not generally based on outcomes of randomised clinical trials, but is derived primarily from epidemiological observations. For this reason, dietary guidelines are necessarily based on expert interpretation of available data and will consequently be subject to challenge. Hence debates are likely to continue on the relative importance of different dietary components such as saturated fats, salt and sugar to the development of CVD. Access to large, population based datasets, linked to better biomarkers of dietary exposure and related genetic signals, may help to improve evidence to help refine future recommendations.
Physical activity
The effectiveness of exercise based rehabilitation is well established in research populations, but more studies are needed to test whether it delivers equivalent benefits in wider populations. Greater emphasis should be placed on high quality observational audit based research which uses data collected from patients accessing cardiac rehabilitation and prevention programmes. Further research using objective measures of activity as well as further high quality trials would also be beneficial.
Multifactorial programmes
A comprehensive, multifactorial programme to improve lifestyle and adherence to treatments is recommended, but currently, evidence for the effectiveness for this approach is weak. Further research is needed to determine how best to translate the impact of single factor interventions to multifactorial prevention programmes.
Recommendations
-
The new JBS3 risk calculator should be assessed formally in different populations and the attitude of the public to CVD prevention over lifetime needs to be evaluated.
-
The role of genetic testing, novel circulatory biomarkers and imaging for subclinical CVD to refine risk estimation needs to be determined, particularly in subjects at ‘intermediate risk’.
-
The mechanisms by which a variety of associated diseases, eg, CKD, adversely affect CVD needs further study. This should provide novel targets for treatment.
-
Research is required on how best to deliver sustained improvements in CVD outcomes from multifactorial prevention programmes involving lifestyle change and drug treatments.
Appendix
Appendix 1: technical details of risk calculator
Lifetime risk model
Age is taken as the time axis in this model, and so age does not appear as a risk factor in the model. Rather, the risk factors adjust the baseline age-specific risks for an ‘average’ individual. The term ‘hazard’ is used for the risk of an event occurring in a small interval, given CVD free survival until the start of that interval. Baseline hazards are required for the whole age range, both for CVD events and non-CVD deaths.
Hazard ratios
The following steps are carried out independently for each gender and each cause of ‘failure’, that is, CVD-events and non-CVD deaths.
Each individual provides a set of risk factors x (possibly transformed to measure deviation from ‘average’). A set of coefficients b is applied to the risk factors to create a linear score S=Σi bi xi for each of CVD events and non-CVD death.
With a proportional hazard assumption this is a log(HR). Taking the exponent eS gives the HR to be applied to the baseline hazard for each of the two causes of failure. For example, if the baseline risk of a CVD event in an age interval t is assessed to be ht, then the risk for the specific individual is ht eS. Within each age interval t, we therefore obtain the two crucial quantities:
-
at: the risk of a CVD event in interval t, given CVD-free survival up to the start of interval t
-
bt: the risk of a non-CVD death in interval t, given CVD-free survival up to the start of interval t
From these two quantities all else follows.
The ‘life-table’ below follows Ulrich et al, although it shows arbitrary age intervals (these were 5 years in Ulrich et al,33 but in QRISK the table is at a very fine scale). In our algorithm we use 2.4 months. The life table begins at the current age of the individual.
Changing the risk factors changes the hazard terms at and bt to at* and bt*: repeating the life table calculations leads to a revised CVD-free surviving proportion et* and revised cumulative CVD proportion ft*.
From these quantities we obtain the information for the risk calculator as follows (assuming we are examining 10-year risks):
-
Heart/vascular age: For the individual with risk factors x, we find a single summary risk measure f(x,age), such as cumulative CVD risk up to age 95 years or expected age at first CVD event. We then find the ‘heart age’ where f(x,age)=f(xA,heart age), where xA is a ‘normal’ person. We assume that ‘normal’ is a comparison with a population of the same age, ethnicity, and gender, but otherwise as the baseline patient. Currently, we use the cumulative CVD risk up to age 95 years as the matching measure. This is calculated iteratively:
-
CVD survival curve: et Probability of surviving free of CVD at end of age interval t
-
Median age at first event: the age at which et=0.5
-
Expected age at first event: Σt et×(width of interval t)
-
CVD-free years gained by changing risk factors: Σt (et*−et)×(width of interval t)
-
Cumulative CVD risk curve: ft Cumulative proportion with CVD events by end of age interval t
-
10-year risks: for interval t corresponding to 10 years older, et (green: alive and CVD -free) ft (red: CVD event) mt (clear: death from non-CVD cause)
-
Comparison with population: Based on 10-year risks for someone who has the same age, ethnicity, gender, but other factors match the QRISK baseline patient.
Implementation of QRISK in JBS calculator
Source of code
The JBS3 Risk calculator is a Flash programme which runs inside desktop internet browsers that support the Flash V.10.2 player. The JBS3Risk model uses a port of the QRISK-Lifetime-2011 C source to action script 3. Further details of the QRISK-lifetime-2011 code are available at http://www.qrisk.org/lifetime/index.php. The QRISK-lifetime-2011 lifetime code is licensed under the GNU Lesser General Public License V.3.0 held at http://www.gnu.org/licenses/lgpl-3.0-standalone.html. The JBS3Risk calculator contains a modified version of that code and is licensed under the GNU General Public License V.3, held at http://www.gnu.org/copyleft/gpl.html. Refer to the calculator front matter for access to source code and licence. The JBS3Risk model reads in data from verbatim copies of the QRISK-Lifetime-2011 data tables, which are published under the Creative Commons Attribution-NoDerivs 2.0 UK: England and Wales License available at http://creativecommons.org/licenses/by-nd/2.0/uk/
Validation against online version
In order to speed up the calculations, the JBS3Risk calculator accumulates values from the QRISK data tables in bins of size 0.02 years before applying the model. A suitable bin size was determined in randomised parameter tests: 99% of the random parameters generate a score within 0.2% of the native score, with worst case less than 1% error. This is for both n-year risk and lifetime risks.
Townsend
Rather than using postcodes as a predictor of the Townsend social deprivation score, the JBS3Model uses a scale based on the quintiles of the Townsend distribution, −3.94, −2.57, −0.8, +1.66 and 5.34. Quintiles were calculated from 2001 census data, published at http://www.apho.org.uk/resource/item.aspx?RID=47504.
Heart age
The JBS3Risk calculator heart age model does not use QRISKHeartAge code. The JBS3Risk heart age is the age at which a baseline patient with the same gender, ethnic group and age would match the calculated lifetime risk.
Evaluation of the Risk Calculator
During the development of the JBS3 Risk Calculator three events were organised with groups of GPs and practitionersi to evaluate the software and gain views on its potential use in practice. At each of these events the Risk Calculator was reviewed using set scenarios which the attendees worked through on laptops, accessing the Risk Calculator through a University of Cambridge site.
Once attendees had worked through the scenarios, they were then asked set questions to gain their views on the inputs for patients, the ease of navigation, how easy to understand each screen was, their preference on individual screens to be used with patients, and the interventions shown and their impact (a full list of questions is shown below).
The feedback from attendees at these evaluation events helped the JBS3 Board to select the final screens used in the Risk Calculator, to choose the order they would be shown in, to add narratives and caveats to ensure the Risk Calculator is an effective tool for practitioners to illustrate their patient's risk of CVD, and also to increase the functionality of the software.
In addition to the three evaluation events, a number of the JBS3 Board members used the Risk Calculator in their practice, giving feedback to the designers to help make the software ideally suited for today's healthcare organisations.
Questions used in evaluations sessions for the risk calculator
Inputs (profile)
In your view, are these the correct inputs used in the profile?
Is it clear what input information is required? And why?
Are there any additional inputs you would wish to consider?
Outlook (curves)
Are the red and blue areas understandable?
Do you prefer the ‘negative’ (increasing risk) or ‘positive’ (survival) framing?
Is ‘heart age’ useful?
Would you feel confident using this model to explain cardiovascular risk to your patients?
Interventions
Are the interventions shown the ones you would want or expect to see?
Is the way of specifying interventions understandable?
Are the ‘yellow’ area and the summary statistics (years gained) comprehensible?
Outcomes (Smilies)
Does the model convey a patient's cardiovascular risk in a strong enough way?
Is the presence of ‘blank’ other deaths helpful or confusing?
Would you feel confident using this model to explain cardiovascular risk to your patients?
Compare (bars)
Do you prefer bars to smilies?
Is the comparison with an ‘average population’ useful?
Would you feel confident using this model to explain cardiovascular risk to your patients?
Overall, would you say understanding this risk calculator software is:
easy moderate difficult
Would you consider using this software with patients? Yes/No
If No, what would prevent you using this software?
What do you see as the stumbling blocks to increasing understanding of CVD risk prevention among the population as a whole?…among young people?…among those identified as already at risk?
How do you feel the software could be improved to avoid these stumbling blocks?
Appendix 2: JBS3 contributors
JBS3 board
Chair of JBS3
Prof John Deanfield
Editorial Group
Prof John Deanfield, Prof Naveed Sattar, Dr Iain Simpson, Prof David Wood
Societies, main representative listed first
British Cardiovascular Society
Dr Iain Simpson
Kirsten Bradbury
Prof Keith Fox
Dr Nick Boon
Association of British Clinical Diabetologists
Dr Peter Winocour
Dr Michael Feher
British Association of Cardiovascular Prevention and Rehabilitation
Prof Patrick Doherty
Dr John Buckley
British Association of Nursing in Cardiovascular Care
Dr Catriona Jennings
Ms Jan Keenan
British Heart Foundation
Prof Peter Weissberg
Dr Mike Knapton
British Hypertension Society
Prof Bryan Williams
Prof Neil Poulter
British Renal Society
Dr Paul Stevens
Dr Maarten Taal
Diabetes UK
Prof Peter Grant
Prof Philip Home
Prof Naveed Sattar
Heart UK
Dr Alan Rees
Dr Dermot Neely
Renal Association
Dr David Wheeler
Dr David Goldsmith
Stroke Association
Prof John Potter
Prof Stephen Jackson
Risk calculator
Prof David Spiegelhalter and Mike Pearson, Cambridge University
Individuals not aligned to organisation (with area of representation)
Prof Roger Boyle (previously NHS England)
Dr Susan Connolly (Diet, previously National Co-ordinator for Prevention of CVD for ESC)
Prof Richard Hobbs (Implementation, previously Primary Care Cardiovascular Society)
Prof Aroon Hingorani (Genetics and Risk Refinements)
Dr Fran Sivers (previously Primary Care Cardiovascular Society)
Prof Gerry Stansby (PAD)
Additional contributors, not part of the JBS3 board
Dr Sonya Craig, Institute of Ageing and Chronic Disease, University Hospital Aintree
Prof Mike Kirby, Bedfordshire and Hertfordshire Postgraduate Medical School
Dr David Preiss, University of Glasgow
Dr Clare Taylor, Primary Care Clinical Sciences, University of Birmingham
Prof Peter C Taylor, Kennedy Institute of Rheumatology, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford
Prof John Wilding, Head of Department of Obesity and Endocrinology, Institute of Ageing and Chronic Disease, University Hospital Aintree
Medical writer, funded by British Heart Foundation
Lisa Lovelidge PhD of Hermes Medical Communications, collated comments, amended JBS3 drafts and conducted literature searches under the guidance of the Editorial Group.
References
Key references are indicated by an asterisk
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Supplementary materials
JBS3 Board conflicts of interest
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- JBS3 Board conflicts of interest - Online DOI-of-JBS3
Footnotes
-
Competing interests There are no significant competing interests. A full declaration of interests for each author is available online.
-
Provenance and peer review Commissioned; internally peer reviewed.
-
↵i Attendees of the Evaluation Meetings for the Risk Calculator were from Redbridge Primary Care Trust (PCT), Primary Care Cardiovascular Society (PCCS), and a breakout session during a conference run by NHS Heart Improvement.