Article Text

Statistics from Altmetric.com
Although there is very little high quality evidence to guide the medical treatment of valve disease, this is an important area of cardiology for two reasons. Firstly, there are many frail older people with symptomatic degenerative valve disease in whom the risks of surgical intervention are prohibitive and medical treatment is the only realistic option. Secondly, there is a real and exciting prospect of using medical treatment to influence the natural history of some forms of valve disease, thereby delaying or even avoiding the need for surgery.
Left ventricular systolic dysfunction caused by ischaemic heart disease was the underlying problem in the vast majority of patients who took part in the landmark trials of medical treatment (angiotensin converting enzyme (ACE) inhibitors, angiotensin receptor antagonists, vasodilators, β blockers, and spironolactone) for heart failure. However, some of these trials included patients with valve disease and the principles that have been learned may be widely applicable. Thus, it seems reasonable to assume that a small dose of spironolactone will benefit most patients with severe congestive cardiac failure including those with valvar heart disease. On the other hand it seems clear that the characteristic haemodynamic problems associated with individual valve lesions may influence the relative benefits and hazards of specific treatments. For example, vasodilator treatment may be unwise in patients with severe aortic stenosis because there is a risk that this will reduce aortic pressure and coronary perfusion without an equivalent reduction in the left ventricular afterload. In contrast, vasodilators may be particularly beneficial in patients with aortic or mitral regurgitation because they might be expected to reduce the regurgitant fraction and increase forward flow. Similarly, by prolonging diastole and left ventricular filling, β blockers may harm patients with aortic regurgitation but benefit patients with mitral stenosis.
Medical treatment might be able to alter the natural history of valve disease in two ways. Firstly, it is conceivable that outcome might be improved by treatments that suppress the disease process in the valve itself—for example, it may be possible to restrict fibrosis, scarring and calcification by using anti-inflammatory treatments in some forms of degenerative and rheumatic valve disease. Secondly, it may be possible to prevent or ameliorate the deleterious effects of secondary heart muscle disease—for example, vasodilator treatment may help to protect the myocardium in patients with left ventricular volume overload caused by chronic aortic or mitral regurgitation.
This article will review the medical treatment of the four major left heart valve lesions (aortic stenosis, mitral stenosis, aortic regurgitation, and mitral regurgitation). The optimum timing of surgery, the role of anticoagulants, and the prophylaxis of infective endocarditis have been covered in separate reviews in this series.
AORTIC STENOSIS
Pathophysiology
Calcific aortic stenosis may be caused by progressive calcification of a congenitally bicuspid valve, when it typically presents in the fourth and fifth decades of life, or senile calcification of a morphologically normal tricuspid valve when it tends to present later in life (fig 1). The disease appears to be an active process that has much in common with atherosclerosis and is probably mediated by mechanical stress (“wear and tear”), lipid deposition, and inflammation; significant coronary artery disease is present in approximately 50% of patients with calcific aortic stenosis and the two conditions share many of the same risk factors, with a similar level of risk (table 1).1,2 Rheumatic disease of the aortic valve usually causes mixed stenotic and regurgitant lesions and is commonly associated with mitral valve disease.
Risk factors for aortic valve calcification
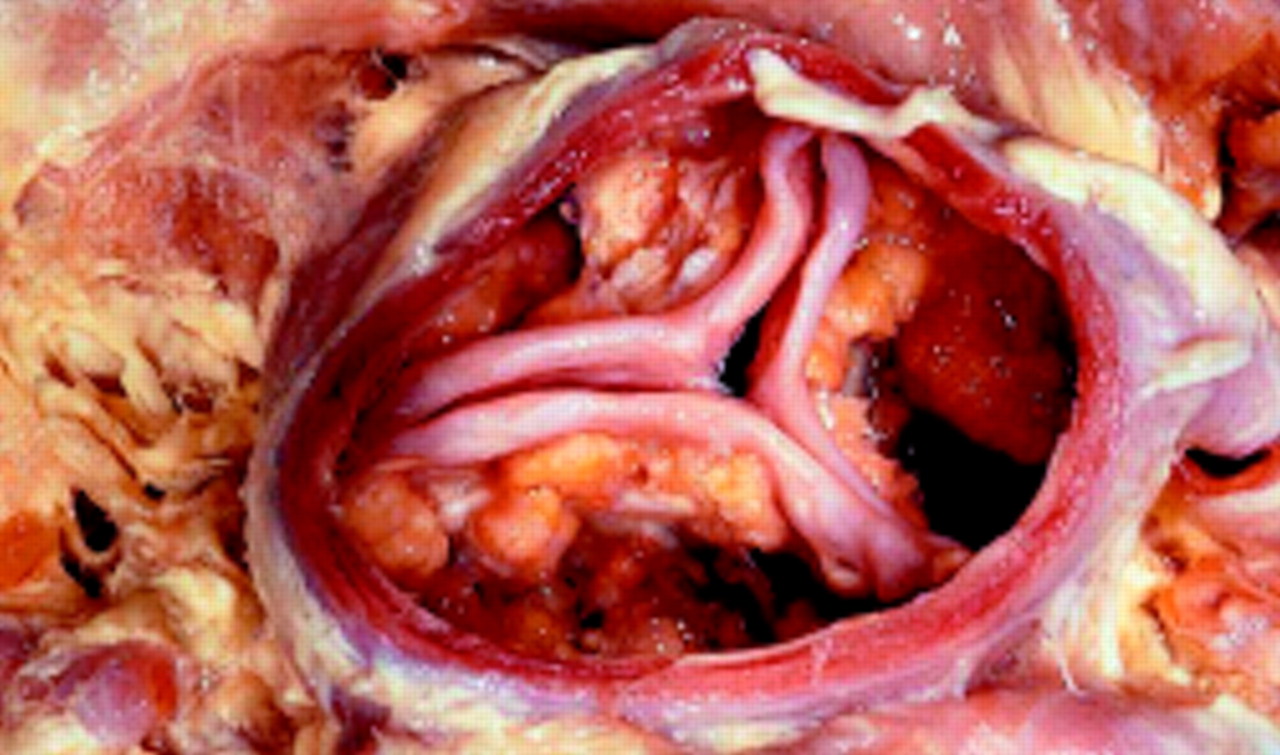
Calcific aortic stenosis: a calcified stenotic tricuspid valve.
Acquired aortic stenosis develops slowly and the cardiac output is initially maintained at the cost of a steadily increasing gradient across the aortic valve. The left ventricle becomes increasingly hypertrophied and coronary blood flow may become inadequate; patients may therefore develop angina, even in the absence of concomitant coronary disease. The fixed outflow obstruction limits the increase in cardiac output required on exercise and effort related hypotension and syncope may occur. Eventually the left ventricle can no longer overcome the outflow tract obstruction and left ventricular failure supervenes. Patients with aortic stenosis typically remain asymptomatic for many years but deteriorate rapidly when symptoms develop; thus, death usually ensues within 3–5 years of the onset of symptoms.3
Symptom control
Symptomatic aortic stenosis is a surgical condition and has become the most common reason for valve replacement in the developed world. However, it is also an important cause of angina and heart failure among frail elderly subjects who are unsuitable for surgery, and in these people conventional medical treatment may provide the only means of alleviating symptoms. The cautious use of β blockers and nitrates may control angina. Unfortunately, nitrates may cause symptomatic hypotension, especially if they are used shortly after exertion. Diuretics may relieve the symptoms of pulmonary congestion but it is important to appreciate that patients with severe aortic stenosis are dependent on adequate filling pressures and excessive diuretic treatment may be hazardous. Digoxin may benefit those with atrial fibrillation or depressed left ventricular systolic function. Atrial fibrillation is often poorly tolerated and in this situation attempts to restore sinus rhythm by means of early DC cardioversion, or antiarrhythmic treatment with amiodarone, should be considered.
Most doctors avoid ACE inhibitors in patients with aortic stenosis and heart failure on the grounds that these drugs are unlikely to reduce left ventricular afterload and may cause dangerous hypotension. These fears have not been substantiated by small clinical studies evaluating short term treatment with a variety of vasodilators including ACE inhibitors, prazosin, hydralazine, nitroprusside, and nitrates.4 For example, two small clinical series describing the acute effects of captopril in severe aortic stenosis (mean aortic valve gradients 78 and 93 mm Hg) have shown not only that first dose hypotension did not occur, but that mean cardiac output increased substantially and pulmonary capillary wedge pressure decreased significantly in the majority of patients. In one of these studies mean cardiac output increased by 41% among patients with overt heart failure; moreover, symptomatic benefit from long term treatment was documented among those who had a beneficial haemodynamic response. Further studies are warranted but it seems clear that some patients with heart failure and aortic stenosis may benefit from treatment with ACE inhibitors provided that these drugs are introduced cautiously in hospital.
Secondary prevention
In established aortic stenosis, natural history studies have shown that the annual reduction in valve area is approximately 0.1 cm2/year, with an average increase in Doppler jet velocity of approximately 0.3 m/s/year (equivalent to an increase in gradient of 7 mm Hg/year)5; however, this varies considerably and tends to be greater in the elderly, those with heavy aortic valve calcification, and, in some studies at least, those with hyperlipidaemia. In one series of 170 consecutive patients a serum cholesterol concentration of more than 5.2 mmol/l (200 mg/dl) was associated with double the rate of reduction in aortic valve area.6 Moreover in a recent non-randomised retrospective study the use of hydroxymethyl glutaryl coenzyme A (HMG CoA) reductase inhibitors (statins) was associated with a significantly lower rate of decrease in aortic valve area (mean (SD) 0.06 (0.16) cm2/year v 0.11 (0.11) cm2/year).7.
These observations have obvious implications for secondary prevention in patients with calcific aortic stenosis, and several randomised controlled trials have been set up to test the hypothesis that lipid lowering treatment with HMG CoA reductase inhibitors will retard the progression, or even induce regression, of the disease. Trials of aspirin and antihypertensive treatment are also warranted.
MITRAL STENOSIS
Pathophysiology
Mitral stenosis is almost always rheumatic in origin; however, in the elderly, heavy calcification of the mitral valve apparatus can produce a similar syndrome.
The mitral valve orifice is slowly diminished by progressive fibrosis, calcification of the valve leaflets, and fusion of the cusps and subvalvar apparatus. The flow of blood from the left atrium to the left ventricle is therefore restricted and left atrial pressure rises, leading to pulmonary venous congestion and breathlessness. There is dilatation and hypertrophy of the left atrium, and left ventricular filling becomes more dependent on left atrial contraction. Any increase in heart rate shortens diastole (the time the mitral valve is open) and produces a further rise in left atrial pressure; situations that demand an increase in cardiac output will also increase left atrial pressure. Exercise and pregnancy are therefore poorly tolerated. At first, symptoms occur only on exercise; however, in severe stenosis left atrial pressure is permanently elevated and symptoms may occur at rest. Reduced lung compliance, caused by chronic pulmonary venous congestion, contributes to breathlessness, and a low cardiac output may cause fatigue.
Atrial fibrillation caused by progressive dilatation of the left atrium is very common. A minority of patients (less than 20%) remain in sinus rhythm; many of these individuals have a small fibrotic left atrium and severe pulmonary hypertension.
Symptom control
Medical treatment is a reasonable option for patients with mild symptoms but mechanical relief of the obstruction, by balloon valvuloplasty or surgery, should always be considered in patients with more severe symptoms, those with new onset atrial fibrillation, and those with evidence of moderate or severe pulmonary hypertension.3 Diuretics will usually reduce left atrial pressure and the symptoms of pulmonary congestion (breathlessness, haemoptysis); however, they may also reduce cardiac output and worsen fatigue. β Blockers and rate limiting calcium antagonists (for example, diltiazem, verapamil) slow the heart rate, at rest and during exercise, and may improve left ventricular filling by prolonging diastole. They will often relieve effort related symptoms and are particularly effective in patients with sinus tachycardia (for example, pregnancy, anaemia), atrial fibrillation, and other tachyarrhythmias.
Atrial fibrillation
Atrial fibrillation is a common complication of mitral stenosis, particularly in older patients, and is associated with a high risk of arterial embolism, especially stroke, and an adverse prognosis (10 year survival of 25% compared to 46% for patients in sinus rhythm3). Although no randomised controlled trials have specifically examined the efficacy of anticoagulant treatment in mitral stenosis there is compelling evidence to support the use of anticoagulants (target international normalised ratio (INR) 2–3:1) in those with all forms of atrial fibrillation and those who have already suffered an embolic event.8 A high proportion of emboli occur at or shortly after the onset of atrial fibrillation and it is therefore desirable to introduce anticoagulants while the patient is still in sinus rhythm. Older patients, those with severe mitral stenosis, and those with left atrial dilatation are at greatest risk and are most likely to benefit from early anticoagulation.
The onset of atrial fibrillation is often accompanied by pronounced haemodynamic deterioration precipitated by a dramatic reduction in left ventricular filling caused by the effects of tachycardia and the loss of atrial contraction. Good rate control is essential to relieve symptoms. Digoxin, β blockers, and rate limiting calcium antagonists can be used to control heart rate, at rest and during exercise, and are all effective.8,9 However, digoxin has a narrow therapeutic index, and is inferior to β blockade in terms of preventing paroxysms of atrial fibrillation, and controlling the heart rate at the onset of atrial fibrillation and during exercise or other forms of stress. Combination drug treatment is often necessary and a few patients require atrioventricular node ablation and pacing.
Paroxysmal atrial fibrillation may respond to treatment with amiodarone or group 1c drugs such as flecainide, but usually gives way to permanent atrial fibrillation. Chemical or electrical cardioversion may have a limited role in the management of persistent atrial fibrillation but, unless the mitral stenosis is relieved by surgery or valvuloplasty, the arrhythmia invariably recurs.
Secondary prevention
There are no treatments that have been shown to retard the rheumatic process of chronic fibrosis and scarring, but eradication of streptococcal infection and prophylaxis against further attacks of rheumatic fever are thought to be beneficial. Most guidelines recommend long term treatment with 250 mg phenoxymethyl penicillin (penicillin V) orally twice daily or, if compliance is in doubt, 1.2 million units of benzathine penicillin intramuscularly every four weeks; a sulfonamide or erythromycin can be used if the patient is allergic to penicillin. The optimum duration of antibiotic prophylaxis has not been established and will depend to a large extent on practical issues such as compliance and the likelihood of coming into contact with populations that have a high prevalence of streptococcal infection. The American Heart Association/American College of Cardiology (AHA/ACC) guidelines recommend that in most patients with established rheumatic heart disease it is advisable to maintain prophylactic antibiotic treatment until the age of 40 years and for at least 10 years after the last attack of rheumatic fever.3
AORTIC REGURGITATION
Pathophysiology
In aortic regurgitation the main determinants of regurgitant volume are the regurgitant orifice area (which is typically fixed), the duration of diastole (a function of the heart rate), and the diastolic transvalvar pressure gradient (aortic minus left ventricular diastolic pressure).10 Both bradycardia and hypertension are therefore undesirable and should be treated energetically.
Aortic regurgitation imposes volume overload and a high afterload on the left ventricle. In slowly progressive chronic aortic regurgitations adaptive remodelling processes, including left ventricular dilatation and hypertrophy, mean that the heart can accommodate large volumes of regurgitant flow for many years with little or no change in filling pressures or cardiac output.11 However, eventually these adaptive processes fail and myocardial dysfunction and left ventricular failure ensue.
The potential haemodynamic benefits of vasodilator drug treatment in aortic regurgitation are obvious. Arterial vasodilators redistribute left ventricular stroke volume by increasing forward flow and reducing regurgitant flow; venodilators and diuretics diminish preload and will reduce both left ventricular end diastolic volume and pressure.10,11 These drugs can therefore be used both to alleviate the symptoms and signs of heart failure and to preserve left ventricular function by reducing wall stress.
Symptom control
Diuretics and vasodilators remain the drugs of choice for the relief of symptoms in patients with aortic regurgitation who are considered unsuitable for aortic valve replacement because of associated comorbidity. Short term vasodilator treatment may also be given to patients with severe heart failure and severe left ventricular dysfunction to improve their haemodynamics and clinical condition before aortic valve replacement.3
Preservation of left ventricular function (secondary prevention)
Several studies have tested the hypothesis that vasodilators can be given chronically to asymptomatic patients with severe aortic regurgitation to reduce systolic blood pressure and afterload mismatch, and thereby preserve left ventricular function, prevent heart failure, and delay the need for aortic valve replacement.
Scognamiglio and colleagues found that nifedipine (20 mg twice daily), compared with digoxin (0.25 mg daily), given to asymptomatic patients with severe aortic regurgitation and normal left ventricular function, reduced the number of patients developing symptoms and/or left ventricular dysfunction; at the end of a six year period only 15% had undergone aortic valve replacement compared to 34% in the digoxin group12 (fig 2). Importantly, when the patients who had been receiving nifedipine came to aortic valve replacement, all survived, and left ventricular size and function improved postoperatively; therefore nifedipine did not appear to mask the development of irreversible left ventricular dysfunction. Long term treatment with nifedipine was also shown to reduce left ventricular mass in an earlier placebo controlled trial in patients with severe aortic regurgitation.13

Cumulative incidence of progression to aortic valve replacement in initially asymptomatic patients with severe aortic regurgitation and normal left ventricular function randomised to treatment with digoxin 0.25 mg daily or nifedipine 20 mg twice daily. Reproduced from Scognamiglio et al12 with permission of the Massachusetts Medical Society.
Similar data have emerged from trials of hydralazine and ACE inhibitors14–16; in these trials hydralazine had a higher incidence of side effects than nifedipine and, in one study, was less effective than enalapril.16 Nevertheless, the admittedly very limited trials of ACE inhibitors in asymptomatic aortic regurgitation have produced inconsistent results, possibly because plasma renin activity is not necessarily increased in this setting.11,14
It is important to appreciate that the goal of protecting the left ventricle in severe aortic regurgitation depends on reducing afterload mismatch by lowering systolic blood pressure14; the dose of whichever drug is chosen should therefore be titrated against blood pressure. However, it is rarely possible to reduce systolic blood pressure to normal because of the high stroke volume which is characteristic of severe aortic regurgitation.
The beneficial effects of vasodilators on left ventricular remodelling in chronic aortic regurgitation are likely to be greatest in those patients with the largest and sickest hearts.10 The clinical trials are certainly consistent with this view and there is no evidence to support the use of long term vasodilator treatment in patients with mild to moderate aortic regurgitation, or those with normal blood pressure and a normal left ventricular cavity size—all of whom have an excellent outlook anyway.
The class 1 recommendations for vasodilator treatment in chronic aortic regurgitation of the ACC/AHA task force3 for management of patients with valvar heart disease are listed in the box below.
Choice of vasodilator
There are very few comparative trials to guide the choice of vasodilator in aortic regurgitation. However, intravenous sodium nitroprusside is usually the drug of choice in acute heart failure because its short half life and rapid onset of action facilitate dose titration. In chronic aortic regurgitation ACE inhibitor treatment is particularly appealing because of the powerful evidence that these drugs reduce morbidity and mortality in patients with hypertension and/or heart failure. An ACE inhibitor is certainly the drug of choice for symptomatic patients with chronic aortic regurgitation and hypertension, poor left ventricular function or overt heart failure. Nifedipine is perhaps the best evidence based treatment that can be prescribed for patients with asymptomatic severe aortic regurgitation and well preserved left ventricular function.
ACC/AHA guidelines: class I* recommendations for the use of vasodilator treatment in chronic aortic regurgitation
-
Chronic treatment in patients with severe regurgitation who have symptoms and/or left ventricular dysfunction when surgery is not recommended because of additional cardiac or non-cardiac factors
-
Long term treatment in asymptomatic patients with severe regurgitation who have left ventricular dilatation but normal systolic function
-
Long term treatment in asymptomatic patients with hypertension and any degree of regurgitation
-
Long term ACE inhibitor treatment in patients with persistent left ventricular systolic dysfunction after aortic valve replacement
-
Short term treatment to improve the haemodynamic profile of patients with severe heart failure symptoms and severe left ventricular dysfunction before proceeding with aortic valve replacement
*Conditions for which there is evidence and/or general agreement that a given procedure or treatment is useful and effective
MITRAL REGURGITATION
Pathophysiology
Mitral regurgitation causes chronic left ventricular volume overload, compensatory left ventricular hypertrophy and dilatation, and ultimately progressive left ventricular failure. Without surgery, the outlook for patients with severe mitral regurgitation is poor with an average annual mortality of 5%. Most deaths are caused by deteriorating left ventricular function and heart failure, but sudden, presumably arrhythmic, death is also common.17
The proven benefits of vasodilator treatment in aortic regurgitation do not necessarily extend to patients with mitral regurgitation for two reasons. Firstly, it is important to appreciate that, in contrast to aortic regurgitation, left ventricular afterload is typically reduced (left ventricular ejection is bidirectional in mitral regurgitation but unidirectional in aortic regurgitation).10,14 Secondly, unlike aortic regurgitation, the size of the regurgitant mitral orifice is often dynamic and critically dependent on ventricular dimensions (fig 3).10 Vasoactive treatment might therefore be expected to alter the regurgitant volume in some but not all settings. For example, a reduction in preload or an increase in contractility will reduce the regurgitant volume when mitral regurgitation is caused by left ventricular dilatation in ischaemic heart disease, or dilated cardiomyopathy. Conversely, a fall in preload may produce a deleterious increase in the mitral regurgitant volume in patients with hypertrophic cardiomyopathy or mitral valve prolapse. In rheumatic heart disease the mitral orifice is usually rigid or fixed and the degree of regurgitation is not therefore influenced by preload. A clear understanding of the aetiology of mitral regurgitation is therefore vital to the logical use of vasoactive treatment.

{kind=link}
{kind=link}
{kind=link}
The relation between the cause of mitral regurgitation, drug induced changes in left ventricular preload, and the degree of mitral regurgitation. (A) In dilated cardiomyopathy the left ventricle is dilated and more spherical than normal. Mitral regurgitation is caused by stretching of the mitral annulus and chordal apparatus. A reduction in left ventricular preload will therefore reduce the degree of mitral regurgitation. (B) In mitral valve prolapse a reduction in left ventricular preload will reduce left ventricular volume and may increase the degree of prolapse and mitral regurgitation. (C) In rheumatic disease fibrous scarring and calcification of the mitral valve leaflets creates a fixed orifice so the degree of mitral regurgitation is not influenced by left ventricular preload.
Symptom control
Mitral valve repair or replacement is strongly indicated if symptoms develop or there is evidence of impaired or deteriorating left ventricular systolic function.17 However, medical treatment can be used to ameliorate symptoms if surgery is contraindicated by serious comorbidity or very poor left ventricular function. Venodilators, particularly nitrates, and diuretics have not been tested in formal trials but might be expected to relieve the symptoms and signs of pulmonary congestion; in our experience they are particularly valuable in patients with preload dependent mitral regurgitation (for example, ischaemic heart disease and all forms of functional mitral regurgitation).
Although there is very little high quality data on the effects of vasodilators in mitral regurgitation, ACE inhibitors are, in our experience, a valuable form of treatment in patients with heart failure and mitral regurgitation. Short term haemodynamic studies have shown a reciprocal relation between forward and regurgitant flow and demonstrated that hydralazine and ACE inhibitors will both typically reduce the degree of mitral regurgitation, and increase forward flow with little or no change in ejection fraction.10 Long term treatment with quinalapril has been reported to improve functional class and reduce left ventricular volume and mass in a very small study of selected patients with chronic mitral regurgitation.18 The theoretical risk that ACE inhibitors will increase the degree of mitral regurgitation in patients with mitral valve prolapse (fig 3) was not born out in one small study19; nevertheless, it seems prudent to assess the impact of vasodilator treatment in such patients by means of serial echocardiography.
Preservation of left ventricular function (secondary prevention)
There are no data to support the hypothesis that vasodilator treatment can preserve left ventricular function in asymptomatic patients with severe mitral regurgitation. There is evidence, however, that in carefully selected patients early mitral valve surgery can achieve this goal.3,17
CONCLUSIONS
Medical treatment may alleviate symptoms and improve the natural history of valvar heart disease (table 2). An understanding of the pathophysiology of different valvar lesions and the haemodynamic changes they engender helps to guide the logical administration of drug treatment.
Summary of useful medical treatments in valvar heart disease
REFERENCES
Linked Articles
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea